
Abstract
Background:
Benign biliary strictures (BBS) befall in ∼7%–23% after hepaticojejunostomy and in 0.3%–0.6% after cholecystectomies. Their treatment options include surgical, endoscopic, and percutaneous management. The percutaneous approach is an excellent mini-invasive option including balloon dilation, biodegradable stents, and sustained dilation, a procedure born endoscopically. However, when the endoscopic approach fails or it is not available, it is possible to perform it percutaneously.
Aim:
To estimate the technical and clinical success of sustained percutaneous dilation with multiple catheters (SPDMC) in hepaticojejunostomy strictures and the percentage of complications and recurrence.
Materials and Methods
: We conducted a retrospective study, from a prospective database from January 2010 to March 2019, of 17 patients with postoperative BBS who failed to percutaneous pneumatic balloon dilation and underwent SPDMC with a mean follow-up of 2 years.
Results:
Seventeen patients between 28 and 71 years of age underwent SPMDC with technical success of 100%; the average number of catheters used was 5.59 (95% confidence interval [CI] 5.12–6.06) achieving a dilatation diameter of 16.15 mm (95% CI 14.71–17.60), and the therapeutic success rate was 71%, with recurrences of stricture and complications of 29% and 18%, respectively. The mean time with SPMDC was 7.06 months (95% CI 5.56–8.56). The median follow-up after dilation was 16 months, with an average of 27.75 months (95% CI 14.15–41.34).
Conclusion:
SPMDC is a feasible technique with a high technical success rate, therapeutic success rate, and low morbidity and mortality.
Introduction
Benign biliary strictures (BBS) due to iatrogenic injuries during or after cholecystectomies befall in ∼0.3%–0.6%, after hepaticojejunostomies in 7%–23%, and after liver transplantation in 2.5%–13%. 1 They can cause jaundice, cholangitis, and in more advanced stages secondary biliary cirrhosis or portal hypertension.1–4 Treatment options for benign strictures include surgical, endoscopic, or percutaneous management. Balloon dilation, multiple plastic stents (MPS), large biliary catheters (18–20Fr), full covered metallic stent (FCMS), or biodegradable self-expanding stents (BSES) are options for the endoscopic and percutaneous approaches.5–11 As surgical management has major morbidity and mortality and also around 15% of recurrence, mini-invasive options have been gaining ground. Endoscopic or percutaneous balloon dilation has a clinical success rate of ∼60%. However, it is the first line of treatment due to its simplicity, low cost, and low morbidity and mortality. 6 For those patients with clinical failure, the next step comprise maintaining a dilation for at least 4 months. The options to achieve this dilation include MPS, FCMS, and BSES. Costamagna et al. described the endoscopic dilation with MPS with a clinical success rate of 80% with 10 years of follow-up. 12 However, this procedure is technically challenging. Therefore, the alternative of FCMS and BSES has been tested with similar results but with an increase in costs. The BSES stents have the advantage of no removal need. 13
In those patients with hepaticojejunostomy strictures, the percutaneous approach is an excellent mini-invasive choice.14,15
Therefore, the purpose of this study was to estimate the technical and therapeutic success and the percentage of complications of sustained percutaneous dilation with multiple catheters (SPDMC) in hepaticojejunostomy strictures in which the balloon dilatation had previously failed.
Materials and Methods
From January 2010 to March 2019 at the Foundation for Teaching, Assistance and Research in Minimally Invasive Surgery (DAICIM) of Buenos Aires Argentina and Bernardino Rivadavia Hospital, 17 patients were selected retrospectively from a prospective database following the inclusion criteria: adult patients older than 18 years with stenotic bilioenteric anastomoses in which the balloon dilatation had previously failed. Diagnose was based on clinical, laboratory, and imaging studies that showed the strictures (cholangiography by magnetic resonance imaging).
Patients diagnosed with malignant stricture due to neoplastic processes, primary sclerosing cholangitis (defined as the presence of multiple intrahepatic strictures), and patients who did not desire the procedure were excluded from the study.
We conducted a retrospective study from a prospective observational and longitudinal database. The characterization variables were age, sex, the primary disease that initially caused the hepaticojejunostomy (bile duct injury [BDI], liver transplantation, pancreaticoduodenectomy, resection of the choledochal cyst), the number of catheters used, and the diameter reached in the dilation measured in millimeters. The follow-up variables were time with dilation and time of follow-up in months.
Main variables such as technical success, therapeutic success, percentage of complications were defined as follows: technical success as the percentage of patients in which all catheters could be set in place to achieve enough dilation to equal the size of the nonstenotic bile duct. The absence of recurrence after removing the SPDMC defined the therapeutic success rate.
Complications were defined as any adverse event after SPDMC, which could be minor or major according to the classification of the Society of Interventional Radiology (SIR) 16 and following Clavien–Dindo classification. 17
Procedure
Percutaneous transhepatic cholangiography was performed by previous biliary drainage, assessing the level, location, and size of the stricture. Then, a safety guidewire (0.0385″AMPLATZ/COOK) passed into the duodenum or jejunum. The D′agostino modification biliary introducer (COOK) allowed the passage of as many guidewires as needed through which the multiple catheters went by (Fig. 1).
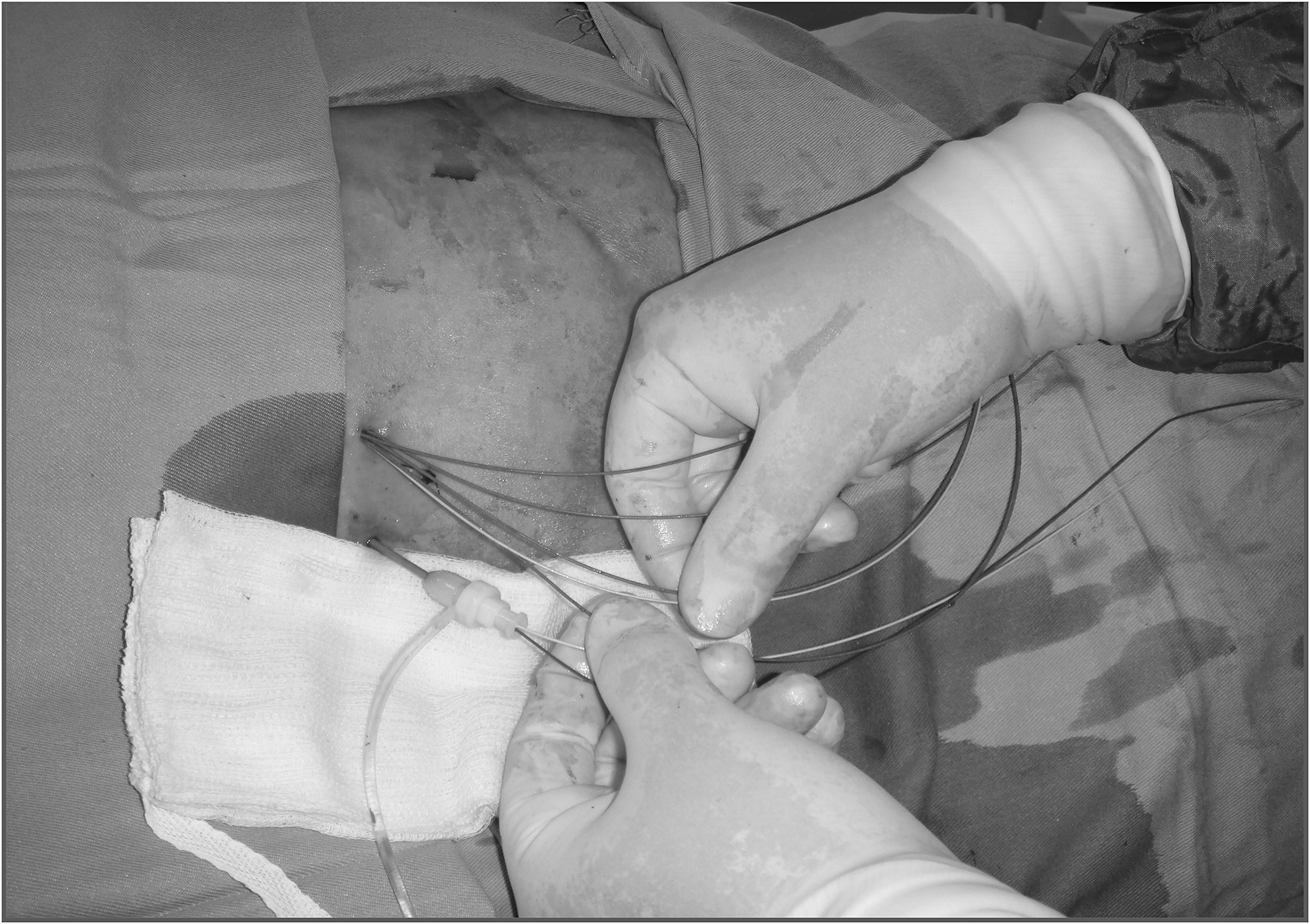
Multiple guidewires as access to catheters in sustained dilation.
Likewise, the multipurpose catheters were prepared according to the distal and proximal measurement of the stricture, making a circumferential cut on its mandrel and anchoring a 2-0 Ethilon at its proximal side acting as an external reference for subsequent removal (Fig. 2).

Preparation of multipurpose catheters that will act as internal catheters.
First, a 10.2Fr internal/external biliary catheter (COOK) was set in place, and second, the distal part of the previously sectioned multipurpose catheters was set that acted as internal plastic stents. Finally, the sectioned proximal part of the catheter was removed along with the mandrel, leaving the previous suture through the entrance hole of the internal/external biliary catheter.
Performing a transcatheter cholangiography showed permeability and total passage of contrast through the stricture (Figs. 3–5).

The multiple catheters within the bile duct.
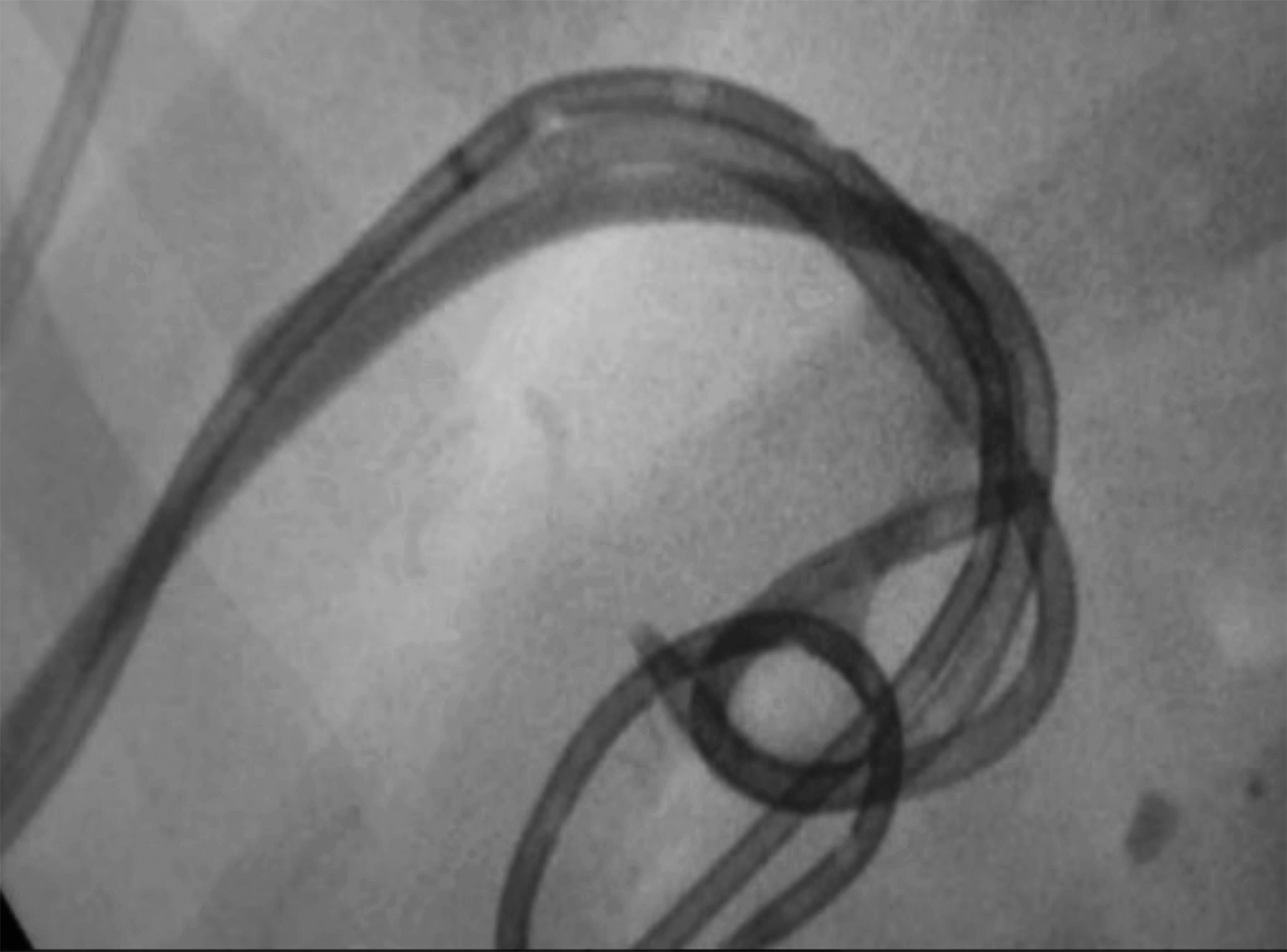
Distal end of the multiple catheters in the intestinal area.

Cholangiography at the end of the procedure.
Statistical analysis and data processing
The data for the study were collected in paper sheets and subsequently passed to a Microsoft Excel 2017 spreadsheet. The percentages of technical, therapeutic success, and complications are presented as average and medium, with ±standard deviation and confidence intervals (CIs). All analyzes were studied using SPSS software version 21.0 and subsequently presented in tables and numerical data as appropriate.
Results
Seventeen patients with hepaticojejunostomy strictures in whom the balloon dilation had failed before were included for SPDMC, aged between 28 and 71 years, all with an initial presentation of acute cholangitis at the time of diagnosis of the stricture.
The underlying disease of the patients was 70.6% BDI, 11.7% liver transplantation (four cirrhosis, one viral hepatitis), 11.7% pancreaticoduodenectomy, and 5.9% by resection of choledochal cyst (Table 1).
Characterization of the Variables
BDI, bile duct injury; CI, confidence interval; HJA, hepaticojejunostomies; PDC, pancreaticoduodenectomy.
All patients had previously undergone percutaneous pneumatic balloon dilation (PPBD) of the stricture on average, three dilations (95% CI 2.82–3.18).
The technical success rate was 100%, achieving the dilation using an average of 5.59 catheters (95% CI 5.12–6.06) in all 17 patients. The average dilation diameter was 16.15 mm (95% CI 14.71–17.60).
The mean time with SPDMC was 7.06 months (95% CI 5.56–8.56), and the median was 6 months. The median control follow-up after dilation was 16 months, with an average of 27.75 months (95% CI 14.15–41.34), minimum follow-up of 3 months, and maximum of 80 months.
Five of the 17 (29%, 95% CI 6–53) patients developed recurrent strictures between 3 and 38 months after withdrawal from SPDMC median time of 23.4 months (95% CI 8.97–37.83), giving a therapeutic success of 71% (95% CI 47–94) (Table 2).
Dependent Variables and Results
CI, confidence interval.
Of the patients with recurrent strictures, 2 patients underwent a new balloon dilation therapy, 2 have a BSES, and the last patient did not accept any new procedure for stenosis and his follow-up was lost.
Only 3 patients (18%, 95% CI 2–37) presented complications related to the procedure, which were 2 cases of postoperative cholangitis and 1 patient needing two procedures to remove one last internal catheter.
Discussion
BBS are common after biliary surgeries, and their management can be very challenging. Their treatment includes surgical, endoscopic, or percutaneous management. This study is the first to evaluate the effects of SPDMC on benign postsurgical strictures following PPBD on a variable time. We found an average clinical success rate of 71% in 2 years average of follow-up based on a 100% technical success and 18% of complications that were of a minor type.17,18
In 100% of patients, we achieved SPDMC, a result that may be comparable with some other studies where they applied only PPBD in several sessions, reporting technical successes from 98.5% to 100%.12,15,19 Percutaneous dilation with balloon, catheters, and bile duct stents is nowadays a very applicable procedure; it makes the technical failure almost very rare.
Azeemuddin et al. mentioned that surgery reparative procedures (such as hepaticojejunostomies and re-hepaticojejunostomy) are the most definitive treatment with technical success rates between 80% and 92% and recurrence rate around 20%–30%, 6 but with a substantial morbidity and mortality, 35% and 0%–5%, respectively. 20 However, they still recommended the percutaneous procedures as an alternative for BBS after primary surgery. 6 Yan et al. described an 88% 5-year stricture-free survival after primary open surgery. 21 Besides, Pottakkat et al., in a prospective study with 300 patients, showed a 92% of clinical success rate. 22
Our results are slightly lower in clinical success (71%). However, the rate of morbidity (18%) and mortality (0%) was better than surgery. These results are comparable to endoscopic studies using balloon dilation and plastic stents. 23
Costamagna et al. were the first to introduce multiple stents for BBS in an endoscopic approach, having great patency long-term result in 76%–90% of cases. The main limitation was the need for multiple sessions and repeated hospitalizations that increase the costs.12,24 Similarly, Draganov et al. performed sequential endoscopic placement of multiple stents across the BBS with a mean number of 4 procedures, a mean of 14.2 months of dilation with the stents, and a 62% of biliary patency. 25
Tal et al. in a randomized and multicenter trial achieved a recurrence of 21.2% using plastic and metallic stents on BBS, at the expense of a high cost-efficacy rate. 26 Percutaneous transhepatic procedures gained a place to be an effective alternative to surgery to treat postsurgical biliary strictures when endoscopy is not feasible or not available. 27 Using biodegradable stents is a safe option with the benefit of needing no removal. 28
In a recent study, the BSES appeared like a safe strategy to treat BBS refractory to PPBD because of free of major complications. Hydrolytic processes degrade the stent in about 3–6 months. The technical success described was 98% and 18% of recurrence, which was resolved by SPDMC (31% of patients) and the rest with other percutaneous techniques. The mean follow-up was 2 years. 29 Siiki et al. gave a shred of good evidence so far about the good compatibility and great mid-term results using the BSES with percutaneous and endoscopic approach.30,31
Limitations of this study include the retrospective nature, the limited sample size, and probably the duration of follow-up to assess the recurrence rate.
To come up with some conclusion, the technical and therapeutic success rates of SPDMC in hepaticojejunostomy stricture was 100% and 71%, respectively, with a low percentage of complications (18%), which make the technique feasible, safe, and comparable to other approaches.
Footnotes
Acknowledgments
The authors wish to thank all those who contributed to this study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.