
Abstract
Purpose:
Due to the small space environment, the learning curve of pediatric laparoscopic procedures is steep and requires excellent procedural skills. These are mainly gained through an apprenticeship on real patients. Computer-based virtual reality (VR) simulators offer a safe, cost-effective, and configurable training environment free from ethical and patient safety issues.
Materials and Methods:
We have developed a prototype VR simulator for core manual skills training for pediatric laparoscopic hernia repair. The simulator currently consists of a hernia suturing task on a virtual nonanatomic trainer at a real pediatric scale.
Results:
A simulation realism validation study was carried out by obtaining subjective feedback (face and content validity) through a questionnaire from 36 pediatric surgeons. The overall simulation realism was on average marked 3.08 on a 5-point Likert scale (1: “very unrealistic” and 5: “very realistic”). The participants were most satisfied with the visual realism (3.33) and most critical about the behavior of virtual tissue. The simulator showed good content validity; its usefulness as a training tool for hernia repair, suturing in general, and in learning fundamental laparoscopic skills was marked 3.61, 3.64, and 3.89, respectively.
Conclusions:
VR simulation of pediatric laparoscopic procedures can contribute to surgical training and improve the educational experience without putting our youngest patients at risk. This simulator is a first prototype, and the initial results indicate that it provides promising foundations for further development. More formal and larger studies such as construct validity and transfer of skills are envisaged as the prototype is developed further.
Introduction
Computer-generated training modules have the potential to enhance surgical training. 1 Such simulators can offer a safe, cost-effective, self-directed, and configurable training environment with objective feedback on performance, free from ethical and patient safety issues. Other advantages include progression monitoring, a large collection of cases, optimizing faculty utilization, potential for reduction in wet lab costs, and laparoscopic instruments.
The aviation world has used virtual computer-based simulation for decades, and this analogy has been used to drive the development of similar computer-based tools for surgeons. Some of the most sophisticated surgical simulation has been developed in the field of robotic surgery (RS). Where, like in the aviation industry, those of who practice RS are required to spend a minimum of 40 hours on the virtual reality (VR) simulator before being able to go into the operating theater. 2
Multiple specialties, such as Neurosurgery, Spinal surgery, General surgery, Gynecology, Orthopedic, and Bariatrics, have now published various studies on the validation of minimally invasive trainers alongside VR simulators.3,4 Seymour et al. carried out a randomized double-blinded study to demonstrate that VR training can improve skills in the operating theater environment. They concluded that the transfer of training skills from VR to the operating room sets the stage for more sophisticated uses of VR in assessment, training, error reduction, and certification of surgeons. 5 However, to date, the market has focused on adult surgery, with no VR pediatric minimally invasive surgery simulators yet available and a paucity of validated training tools for pediatric surgery in general.
Recently, Pacilli and Clarke published evidence in areas of simulation-based research with a comparison and discussion of evidence behind VR training and the acquisition of surgical skills, along with improvement in operating theater performance. They reported that few research programs exist in the field of Pediatric surgery examining technical skills specific to a pediatric surgeon, who requires the development of a unique set of skills where simulation could play an important role. 6
Laparoscopic pediatric inguinal hernia repair is an established and comparative approach to the management of pediatric inguinal hernia with potential advantages over a traditional open operation. 7 It is performed in most centers worldwide that offer advanced minimal access surgery for children and was recently shown to be superior to the traditional open repair by the International Pediatric Endosurgery Group (IPEG) guidelines on minimal access approaches to the operative management of inguinal hernia in children. 8
Inguinal hernia repair is only one of several pediatric surgical interventions that can benefit from a minimally invasive laparoscopic approach. However, the neonatal and infant abdomen is a small space and injury to adjacent bowel, vessels, and groin structures carries significant morbidity. The procedural skills needed for the pediatric population differ to the adult environment due to such small space, as well as significantly smaller instruments moving within a restricted operative field. As a result, the learning curve for laparoscopic surgery in neonates and infants is steep, demanding advanced operative skills, yet there are limited training opportunities. 6
Our aim in this project was to develop a VR simulator for pediatric inguinal hernia repair that had a high feasibility and validation score among pediatric surgeons. We aimed to design a simulator that would allow for deliberate and repetitive practice using a cost-effective and reproducible training methodology, which could be incorporated into a Pediatric Surgical training curriculum.
Materials and Methods
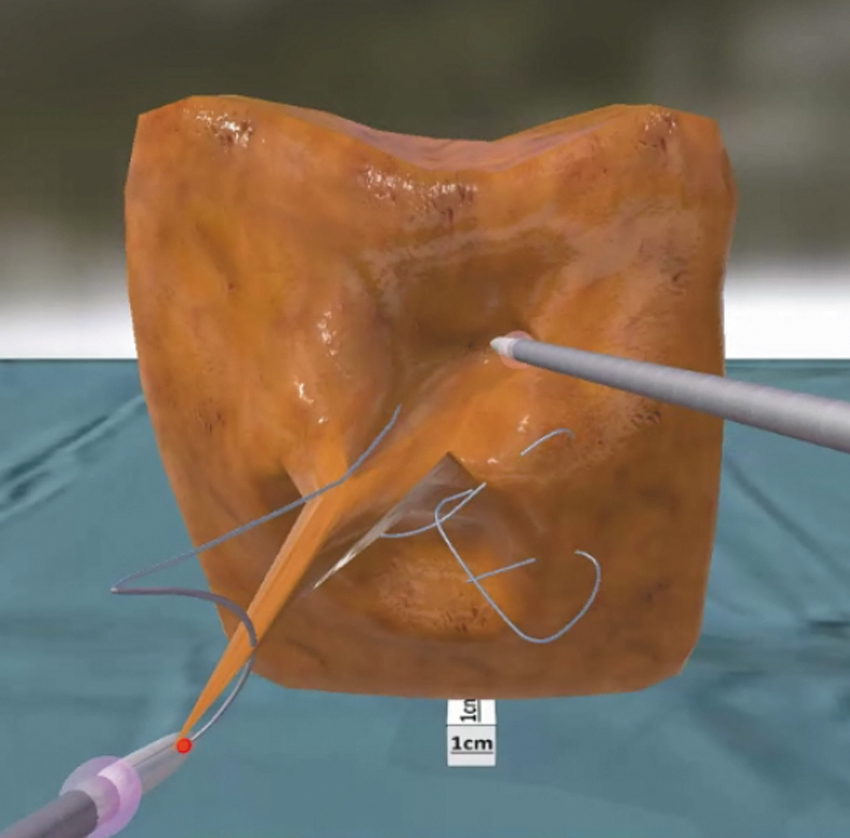
We have developed a prototype VR simulator for core manual skills training in laparoscopic pediatric hernia repair. The experimental apparatus consisted of a real-time software responsible for simulation of a hernia suturing task (Fig. 1), laptop personal computer, two-dimensional computer screen (Fig. 2a), and two Simball input devices (G-coder Systems AB, Sweden), which mimic the pediatric laparoscopic instrumentation (Fig. 2b).

Screenshot from hernia suturing simulation software. Color images are available online.

The pediatric hernia simulator:
Simulation software
The simulator software development followed an agile iterative design, with implementation and validation cycles in close collaboration with supervising clinical experts. A range of state-of-the-art physically based simulation algorithms were developed for the pediatric scenario and were responsible for the behavior of the virtual anatomy, surgical instruments, and interactions between them. The Unity3D games engine (Unity Technologies, USA) was used as development platform in combination with a bespoke medical simulation framework based on position-based dynamics (PBD).9,10 A multithreaded sequential Gauss–Seidel physics solver was implemented in C/C++. High refresh rates of up to 3–4 kHz allowed for small simulation time-steps (0.25–0.33 mseconds), essential for accurate simulation at the required small pediatric scale.
Hernia anatomy was modeled as a volumetric tetrahedral mesh (Fig. 3). Distance constraints (1712 in total) were generated along all volumetric mesh edges. Volume constraints were generated for each tetrahedron (1044 in total). The stiffnesses of distance and volume constraints were separately adjusted to recreate a wide range of biomechanical properties of the anatomy. These were visually tuned to approximate the behavior of the real anatomy based on the judgment of senior clinicians interacting with the virtual anatomy through the laparoscopic device, while achieving real-time performance at high physics refresh rate.
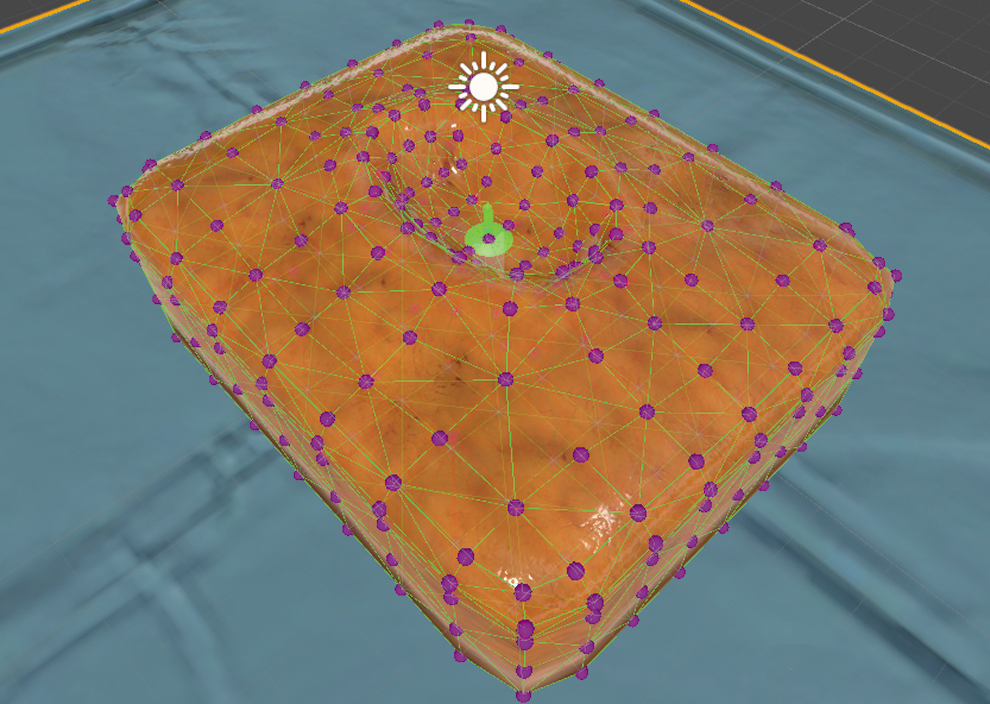
Virtual inguinal hernia benchtop model with particles (mass points) as dots and distance constraints on the surface as wireframe. Color images are available online.
The needle and suture consisted of 128 mass-points (particles) and 127 material frames (Fig. 4). They were simulated as a single position- and orientation-based elastic rod. 11 This enabled for realistic recreation of stretch, bend, and twist deformations in a unified way. The twist deformation was balanced out by the bend deformation and vice versa, which resulted in complex suture looping phenomenon. Moreover, such approach enabled full control over the rest shape of the virtual rods. This allowed to model a curved needle, as well as intrinsic bends of the surgical suture, which helps the operator to tie surgical knots (Fig. 5).

Material frames of the needle and thread. Color images are available online.
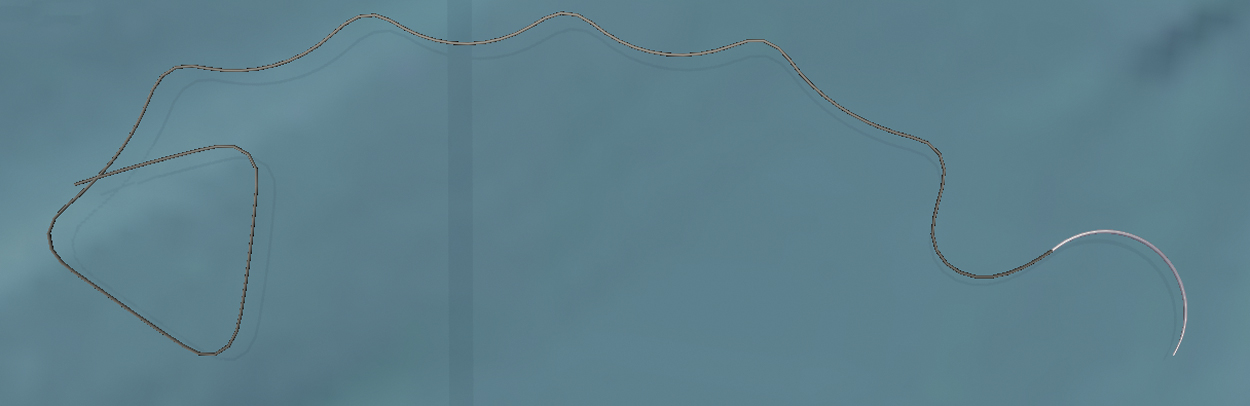
Virtual needle and thread in its rest shape modeled using elastic rod approach. We can observe the intrinsic bend of a rod material in action. Color images are available online.
Suturing was simulated by dynamically adding and removing sliding constraints between needle/suture segments and the volumetric mesh. The constraints allowed the needle and suture to slide, with friction, through the tissue mesh surface and its interior, while deforming the tissue when pulled laterally at the same time with respect to the mesh.
A dynamic bounding volume hierarchy of axis-aligned bounding boxes was used for broad-phase collision detection, with a triangle–sphere intersection used for narrow-phase collision detection. For each intersecting triangle–sphere pair, a PBD collision constraint was generated. It pushed the hernia triangles and the suture out of the collision according to penetration depth, triangle barycentric coordinates, and normal vector. We used a Coulombian friction approximation, taking into consideration positions from the previous and current physics steps to approximate velocities needed for friction calculations.
Study design
The study was approved by the Imperial College Ethics Committee (ICREC-19IC5447). Informed consent was obtained from each participant before their participation, and standard procedures were implemented regarding anonymity and confidentiality.
The procedure started with a simulated view of a virtual nonanatomic benchtop model of an internal inguinal ring (Fig. 1). The participants were required to complete three hernia repair procedures, one at a time, by creating a purse-string suture around the patent internal inguinal ring.
All qualified doctors were eligible for inclusion in this study. Participants were divided according to the level of expertise defined as below:
Experts: We have defined experts as those who perform more than 50 animal-model or human laparoscopic pediatric procedures independently per calendar year. Intermediates: We have defined intermediates as those who perform 10–50 animal-model or human laparoscopic pediatric procedures independently per calendar year. Novices: We have defined novices as those who perform less than 10 animal-model or human laparoscopic pediatric procedures independently per calendar year.
This grouping was made using a format analogous to previous studies of a similar design.12,13
Before performing their first virtual procedure, participants' operative experience, experience of videogames, demographic data (age and gender), and interest in VR simulation were recorded through an online questionnaire. Next, all participants were provided with a technical instruction sheet outlining the nature of the simulation. The aim of this sheet was to give a brief overview of the equipment, tasks, and factors, which will differ to real life owing to the limitations of performing the procedure in a simulated setting. The instruction sheet was designed so as not to instruct on the particular challenges of performing a laparoscopic pediatric hernia repair. After reading the instruction sheet, participants were allowed a maximum of 3 minutes to familiarize themselves with basic navigation of the endoscope and how to operate the instruments. Before commencing their first procedure, participants were given the opportunity to ask questions relating to the practicalities of the simulation but were not be allowed to request any technical advice as to how best to perform the procedure. No time limit was set for the procedures.
Face validity and content validity were evaluated by asking participants to complete the aforementioned questionnaire after finishing their last procedure. The questionnaire assessed graphical appearance, behavior of tools and tissue, difficulty of the procedure and overall realism (face validity), as well as the adequacy of the simulated tasks and perceived utility of the simulator as a training tool for laparoscopic pediatric hernia repair (content validity).
Results
In total, 36 participants took part in the study (19 male and 17 female). Nearly 90% (32 of 36 participants) classified their specialty as “Pediatric Surgery” and 4 as “Pediatric Urology.” Majority of participants (34) was right-handed. The average age was 38.8 years (standard deviation [SD] = 8.3 years). We divided the participants into three groups based on the number of laparoscopic pediatric procedures, which they perform annually independently in human (7 Novices with less than 10 procedures/year, 18 Intermediates with 10 and more but less than 50 procedures/year, and 11 Experts with 50 and more procedures/year). Table 1 provides details of participants' operative experience.
Summary of Study Participants' Surgical Experience
VR, virtual reality.
The majority of participants (60%) had previously used a laparoscopic simulator, and 28.6% had even used a pediatric laparoscopic simulator. Only 4 participants had never previously experienced training on either laparoscopic or nonlaparoscopic simulator. Most of participants stated (83.3% agreed or strongly agreed) that they are interested in pediatric laparoscopic surgery, and 77.8% stated that they are interested in VR simulation in pediatric laparoscopic surgery.
Regarding face validity (Fig. 6 and Table 2), the overall simulation realism weighted average score was 3.08 (SD = 0.88) on a 5-point Likert scale (1: “very unrealistic” and 5: “very realistic,” the weighted average score was calculated by multiplying these scale values by the number of participants who chose the corresponding value and dividing the result by the total number of participants, the SD was calculated by treating the responses as ordinal data).
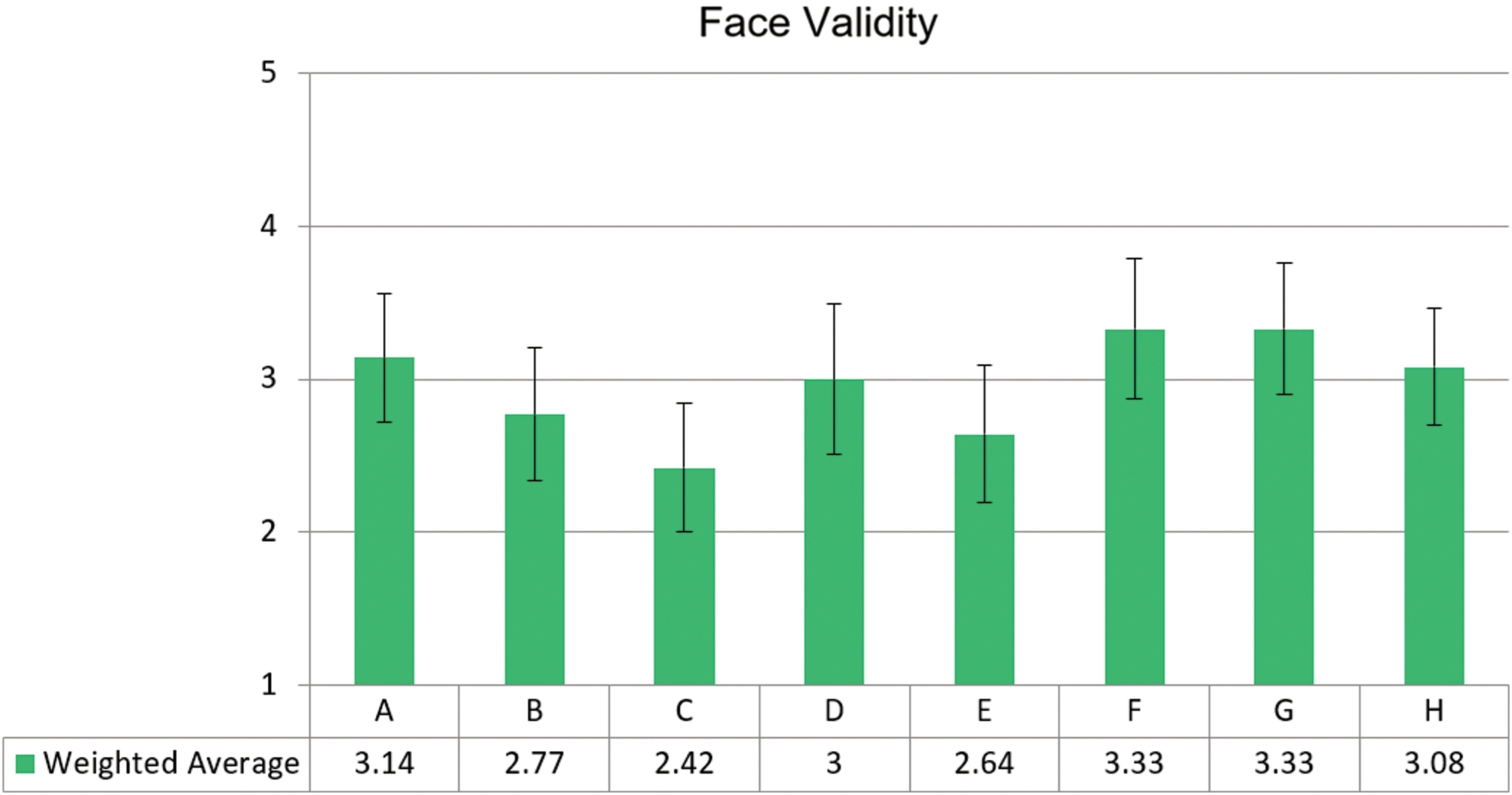
Face validity results. Color images are available online.
Face Validity Questions
The participants were most satisfied with the visual realism (average score 3.33, SD = 0.86) and with the laparoscopic hardware interface (average score 3.33, SD = 0.93). The realism of virtual laparoscopes scored on average 3.14 (SD = 0.83), whereas the realism of virtual suture and needle was 2.77 (SD = 0.86), on average. The average realism score of interactions between virtual laparoscopes and needle/suture was 3.0 (SD = 0.98), and between virtual needle/suture and tissue 2.64 (SD = 0.99). The participants were most critical about the behavior of virtual tissue, which was marked on average 2.43 (SD = 0.84). Free-text comments pertaining to face validity are shown in Table 3
Face Validity—Free-Text Comments
VR, virtual reality.
The simulator showed good content validity (Fig. 7 and Table 4). Its usefulness as a training tool for hernia repair, suturing in general, and in learning fundamental laparoscopic skills was marked 3.61 (SD = 0.90), 3.64 (SD = 0.96), and 3.89 (SD = 0.89), respectively (66.7%, 58.3%, and 72.2% participants, respectively, stated “useful” or “very useful”). Free-text comments are shown in Table 5.
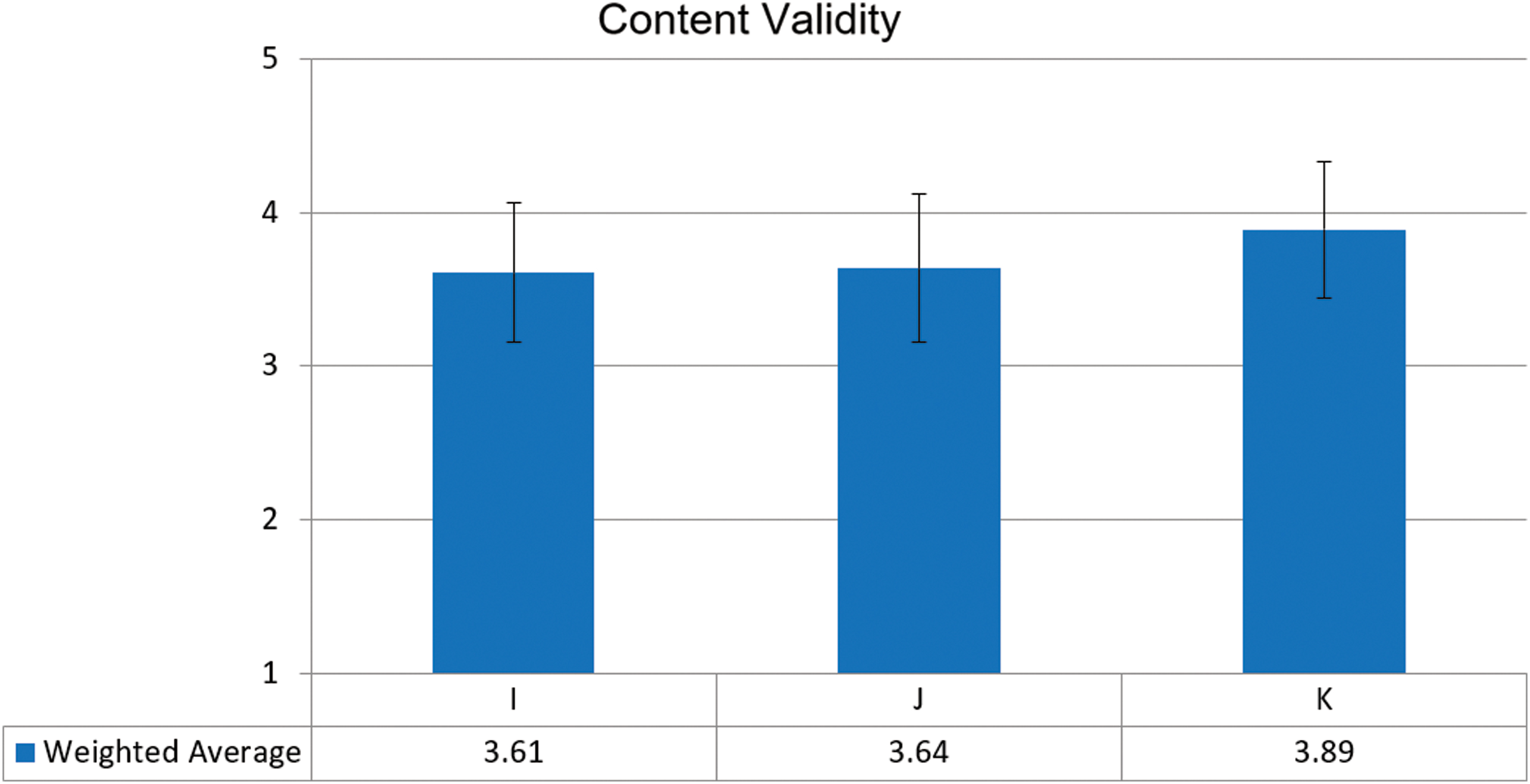
Content validity results. Color images are available online.
Content Validity Questions
Content Validity—Free-Text Comments
Finally, nearly half of the participants (48.6%) would recommend the simulator to others (Fig. 8), with the vast majority (88.9%) of participants finding VR suturing simulation as a useful tool in surgical training curricula, while 83.3% thought that VR simulation in general can prove useful in such training (Fig. 9).
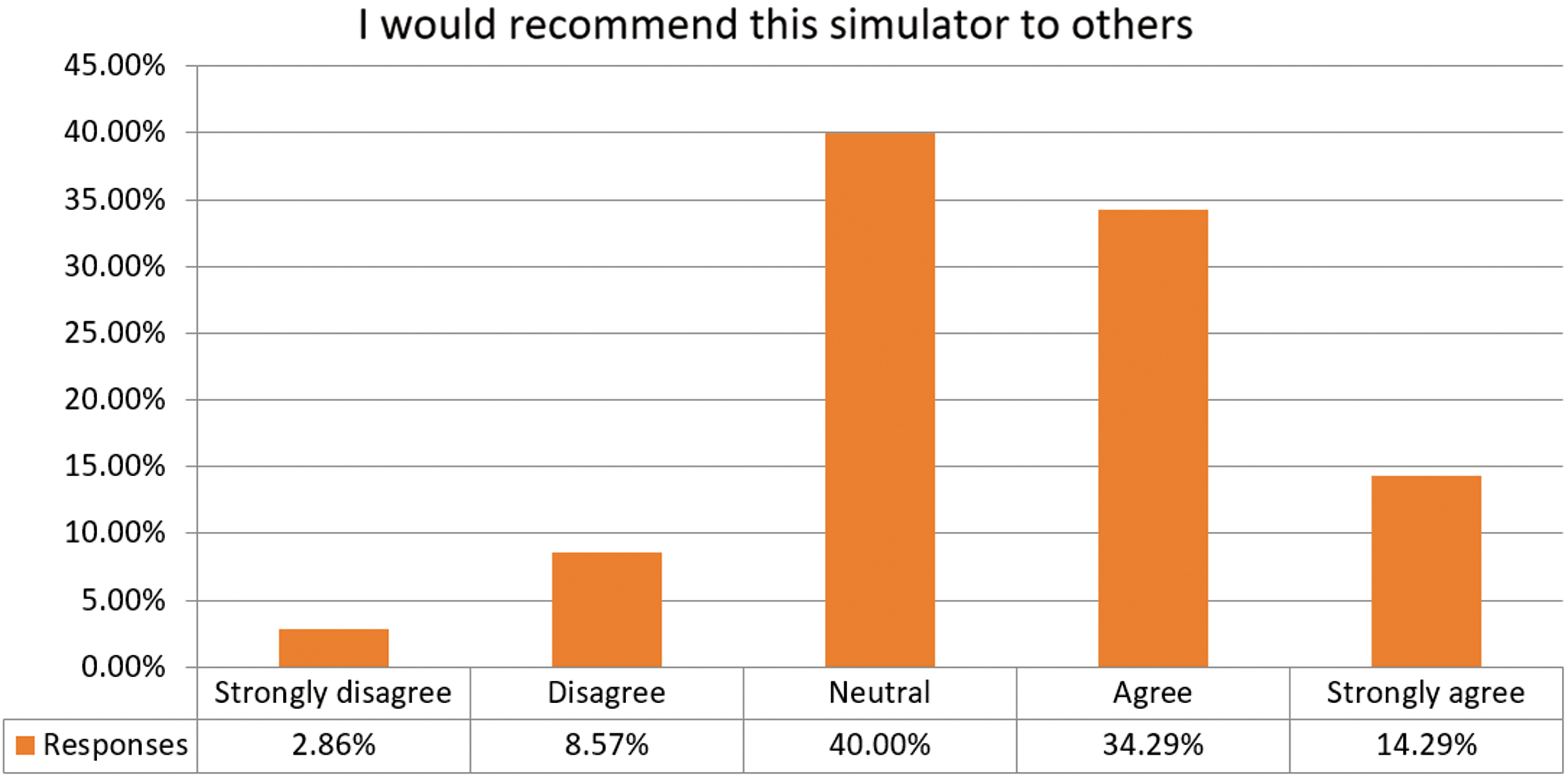
Response to “I would recommend this simulator to others” question. Color images are available online.
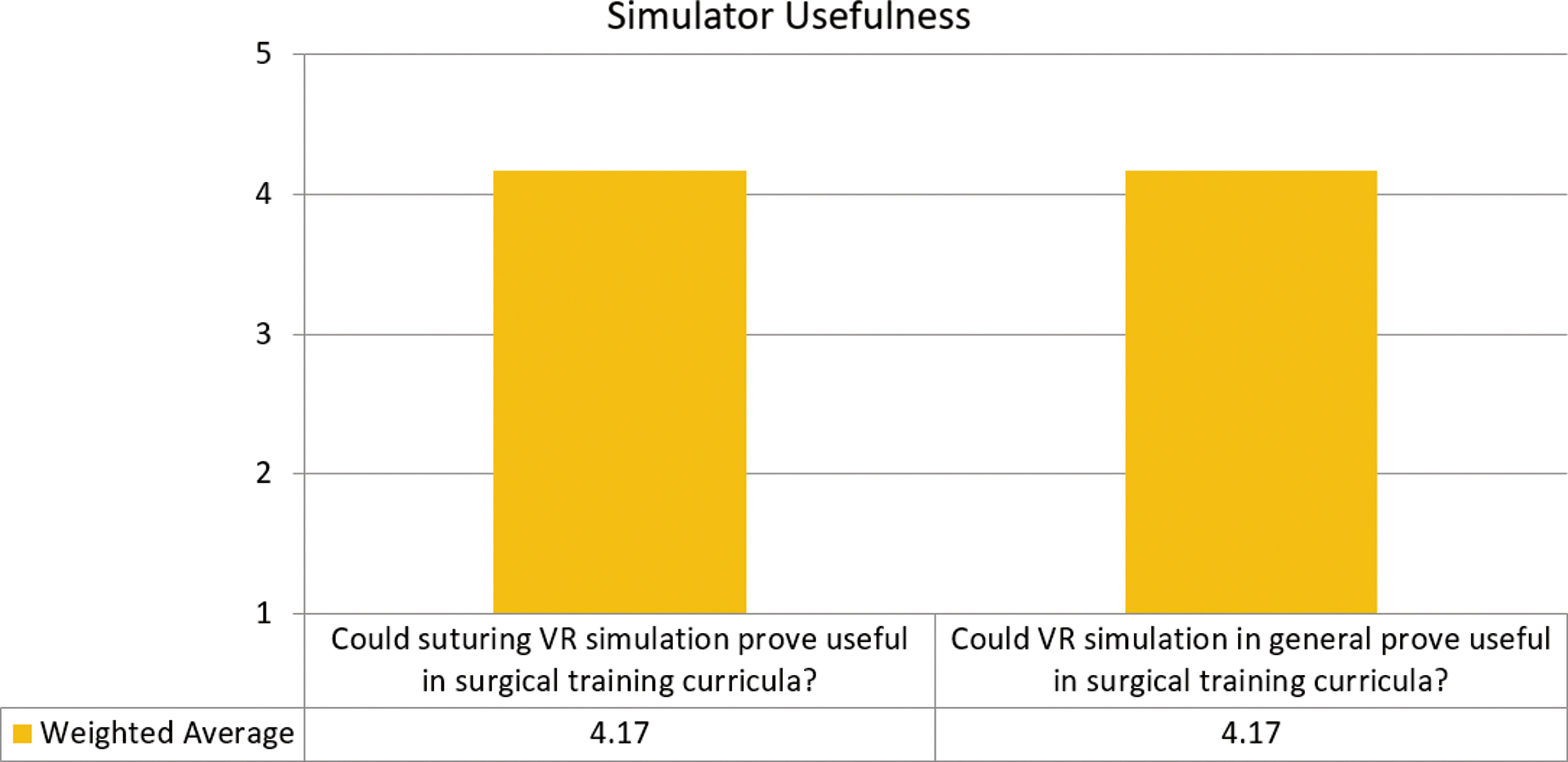
Responses to questions regarding simulator usefulness. Color images are available online.
Limitations and future work
During this initial study, several shortcomings of our simulator prototype were identified. The first one, which was often mentioned by participants in free-text comments (Tables 3 and 5), is related to lack of haptic feedback support by the Simball laparoscopic hardware interface. For many participants, this caused problems even with simple maneuvers such as passing the needle between two instruments. In any subsequent model, we aim to either adapt a generic haptic device such as Touch (3D Systems, USA) to laparoscopy or using an off-the-shelf laparoscopic haptic interface such as the Haptic Avatar (Follou Haptics, Sweden).
To maintain a high physics refresh rate, the discretization of virtual tissue was relatively low (1044 tetrahedral elements). This turned out to be problematic during large deformations, which are quite common during hernia repairs as peritoneum tissue is very stretchable. The insufficient tissue discretization could not recreate such large stretches, which resulted in large distorted triangles also described by participants as spikes (Fig. 10 and Table 3). To tackle this problem, we are looking at further improving the performance to be able to support higher tissue discretization, while maintaining high physics refresh rate. An alternative approach would be an adaptive algorithm, which would dynamically increase the discretization as needed in the regions of large deformations.
Tissue distortion (spikes) during large deformation due to its insufficient discretization. Color images are available online.
Another problem often mentioned by participants in their comments (Tables 3 and 5) is related to needle/suture collision response during complex deformation cases. This caused the suture to occasionally getting stuck inside the tissue or even tissue popping “inside-out.” Our temporary workaround was to press a button, which would deactivate collisions, if such entanglement occurred. To properly address this problem, we are looking at improving the collision detection and response systems by solving the collision constraints globally, rather than each collision sequentially in separation from others.
Finally, our simulation was nonanatomic, meaning that body structures crucial for the hernia repair procedure such as bowels, vas deferens, and testicular vessels were missing. The participants did not have to be careful not to damage them. The next version of our simulation will contain all the required anatomy.
Conclusions
We have developed a prototype VR simulator for core manual skills training for laparoscopic pediatric hernia repair. The simulator currently consists of a hernia suturing task on a virtual nonanatomic trainer at a real pediatric scale. It focuses on training and assessing the core manual skills necessary for performing the laparoscopic pediatric hernia repair procedure in a safe environment. Our goal is to enable junior surgical trainees to attain a higher degree of knowledge and technical ability of performing key operative stages in a small surgical space before consolidating them in a real operating theater.
This pilot study rated the overall simulator as moderately realistic, recognizing its usefulness as a training tool for laparoscopic pediatric hernia repair, surgical suturing, and learning fundamental laparoscopic skills, highlighting its potential for further development and widespread adoption.
VR simulation of minimally invasive pediatric procedures can contribute to training and improving the educational experience of pediatric surgery trainees without putting the youngest patients at risk. However, for improved educational outcome, such virtual training should still be supplemented by practice on laparoscopic box trainers and/or animal models.
Recent global events due to COVID-19 have further limited training opportunities for all surgical specialities.14,15 As such, simulation-based surgical education will become increasingly relevant to the skill acquisition of trainee surgeons. VR models similar to the one we have developed will afford self-directed learning and feedback in a physically distanced training environment.
Building on our existing proof-of-concept prototype, we aim to develop an anatomical and haptically enhanced version of the simulator that will allow a faster learning curve and improved translation of skills to the operating theater environment. We are also planning to explore the simulation of other less common pediatric minimally invasive surgical procedures such as esophageal atresia and diaphragmatic hernia repair. More formal and larger studies looking into assessment of training effectiveness, such as construct validity and transfer of skills, are envisaged as the prototype is developed further.
Footnotes
Acknowledgments
The authors wish to thank the study participants.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.