
Abstract
Background:
Laparoscopic pyloromyotomy has become a gold standard for the treatment of congenital hypertrophic pyloric stenosis (HPS). There have been recent reports on the use of transumbilical single-site laparoscopic surgery for congenital HPS; however, using transumbilical single-site laparoscopic surgery in pediatric cases is still controversial due to the difficulty with manipulation. In this study, some preliminary experience with the application of a novel transumbilical single-site laparoscopic approach in congenital HPS is described.
Methods:
A retrospective study was conducted involving 25 patients with congenital HPS treated in our hospital from August 2016 to August 2019. A pyloric electrocoagulation chisel combined with a left-handed main operation was completed in all of the patients and the operative times, postoperative length of stay, and operative complications were recorded.
Results:
The laparoscopic operation was completed in 25 patients with an average operative time of 21.9 ± 5.5 minutes, average postoperative length of stay of 2.5 ± 0.9 days, and no perforations of the pyloric mucosa, recurrent obstruction, surgical incision infections, and incision hernias. All of the patients had at least 3 months of follow-up, good growth and development, and the parents were satisfied with the postoperative scars.
Conclusion:
A pyloric electrocoagulation chisel combined with a left-handed main operation in the treatment of congenital HPS by a single-site umbilical laparoscopic pyloromyotomy is safe and effective, and can achieve a satisfactory cosmetic effect.
Introduction
Congenital hypertrophic pyloric stenosis (HPS) is a common gastrointestinal tract abnormality in newborns and infants. The radical treatment method is a pyloromyotomy. 1 In traditional operations, the incision is made in the right upper quadrant to deliver the pylorus from the abdominal cavity, but there would be a large scar and significant trauma. When laparoscopic treatment of HPS was first reported by Alain in 1991, 2 additional three-hole laparoscopic pyloromyotomies have been reported and shown to be effective and safe with better cosmetic outcomes than a traditional laparotomy.3–5
With the emergence of scarless operations involving the abdominal wall, single-site umbilical laparoscopic pyloromyotomy has also been reported6–10 ; however, because a single-site umbilical laparoscopy is difficult to perform in newborns and has a high probability of severe complications, such as mucosal perforation and recurrent obstruction. 11 Therefore, a single-site umbilical laparoscopic pyloromyotomy has not been greatly reported in recent years, and based on many years of experience with three-hole laparoscopic operations, we used a pyloric electrocoagulation chisel combined with a left-handed main operation to overcome many difficulties with single-site umbilical pyloromyotomies and have achieved satisfactory results, which are reported as follows.
Materials and Methods
Clinical data
The guardians of the newborns signed informed consent and our research was approved by the Ethics Committee of Taizhou Hospital of Zhejiang Province.
Twenty-five patients with congenital HPS who were treated in our hospital from August 2016 to August 2019 were retrospectively reviewed. All of the patients conformed to the following criteria: a history of nonbilious vomiting; pyloric muscle thickness examined through B-mode ultrasound ≥4 mm; lipiodolography of the upper gastrointestinal tract showed a linear change in the pyloric canal or no development with delayed gastric emptying, which prompted pyloric obstruction; and no history of an abdominal operation. Exclusion criteria: patients with other serious diseases, such as congenital heart disease and severe pneumonia.
Methods
The structure of the pyloric electrocoagulation chisel was as follows: the head end is flat and blunt; 0.3 mm thick; 3 mm wide; round body; 40 cm long, except 4 mm of the head end is not covered by insulating material; the remaining parts are covered by insulating material; and the tail end can be linked to an electric lead of a high-frequency electrotome (Fig. 1). This device was approved for use by the Ethics Committee of the hospital.

Structure of the pyloric chisel.
The operative method was as follows: before surgery, fluid status and disturbances in electrolyte balance were corrected, the trachea was intubated and general anesthesia was administered, the gastric contents was emptied through a gastric tube, the patient was placed in the supine position and the chest was slightly elevated, the display was positioned on the head side of the child. the operator stood on the left side of the child and the assistant stood on the right side of the child, a pneumoperitoneum was established with a pressure of 8–10 mm Hg (1 mm Hg = 0.133 kPa), a 5-mm arc-shaped incision was made along the umbilical nest at 12 o'clock above the manipura, a trocar was placed with a 30° lens under direct vision, 3 mm incisions were made at 3 and 9 o'clock of the manipura, the operating grasper was introduced into the abdominal cavity under endoscopic surveillance, the operator identifies the enlarged pylorus along the stomach first, then places the grasper using the right hand to fix the anterior wall of the stomach to be close to the pylorus at 3 o'clock, turns the grasper over and pulls the grasper forward and downward appropriately, exposes the avascular space on the mesangial side toward the pyloric canal; the operator places the pyloric electrocoagulation chisel (power set at 13–15 Watts) with the left hand at 9 o'clock, and the seropyloric muscular layer from the duodenum end of the pylorus to the stomach end was divided by electrocoagulation cutting, the head end of the pyloric electrocoagulation chisel was inserted into the pyloric serosa and the shallow muscular layer was cut by electrocoagulation, and the pyloric electrocoagulation chisel was rotated slightly downward along the space to widen the gap between the muscles. (Figs. 2 and 3), a grasper was used to separate the pyloric muscular layer completely to bulge the mucous membrane. 50–100 mL of air was injected through the stomach tube, after the stomach was full, whether the air could pass the pylorus smoothly and whether there was air leakage was noted, if there was no abnormality upon examination, the pylorus was covered with omentum majus, the navel incision was closed and medical tissue glue was used to bind the skin.
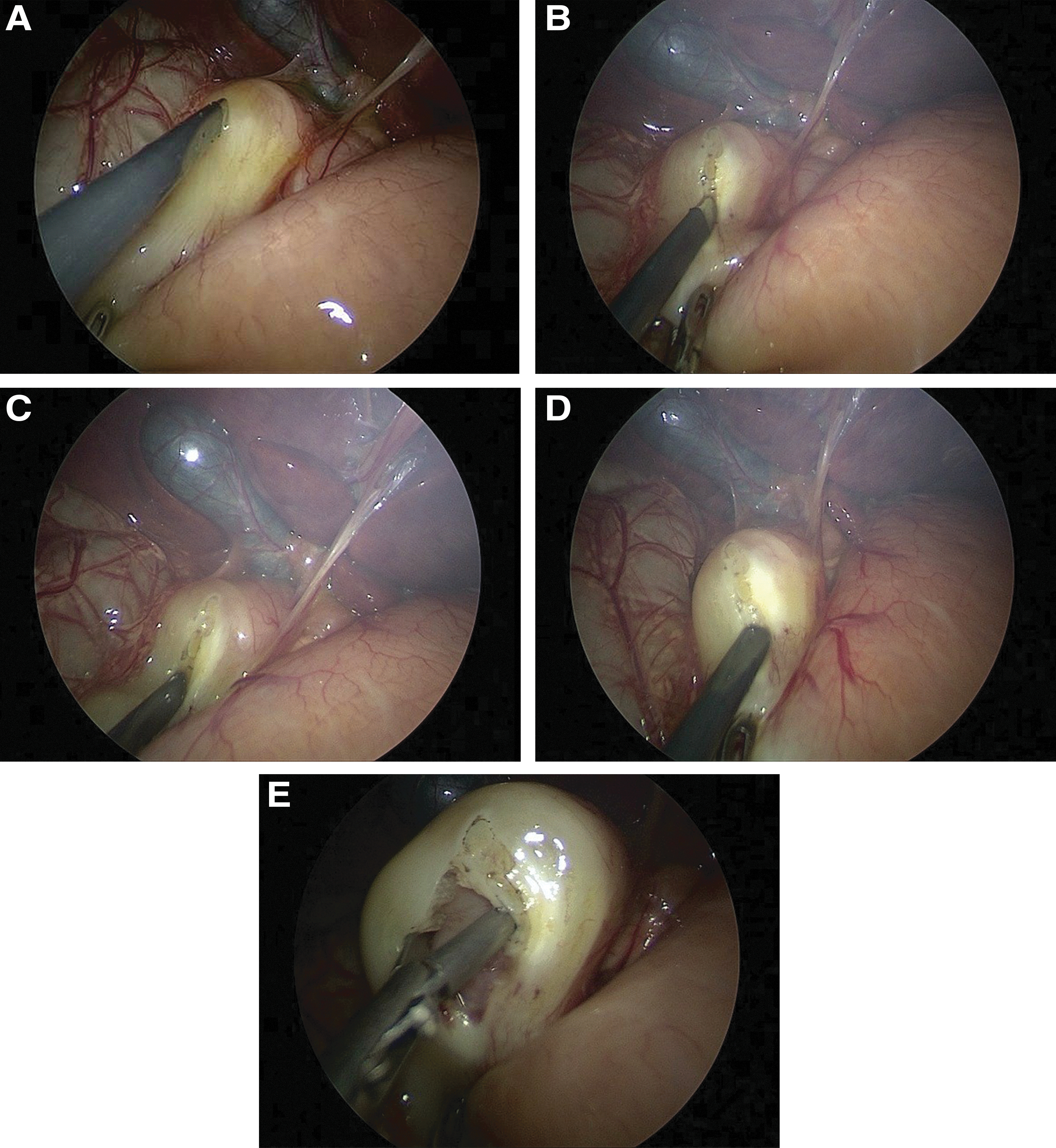

This figure shows the position of the umbilical operating grasper. In the 3 o'clock direction, the grasper is used by the right hand to fix the anterior wall of the stomach close to the pylorus. At the 9 o'clock position, the pyloric muscular layer is cut and expanded by the left hand.
The following observation indicators were recorded: the operative time, postoperative length of stay, and operative complications.
Results
Among the 25 patients, 6 were female (40.0%). The median age was 49.5 ± 8.5 days (range 34–66 days). The median weight was 3.7 ± 0.5 kg (range 2.5–4.5 kg). The thickness of pyloric muscular was 4.9 ± 0.5 mm (4–6 mm) and the length of pyloric tube was 21.2 ± 4.7 mm (15–27 mm).
Single-site umbilical laparoscopic procedures were completed in 25 patients without conversion to laparotomy, with a mean operative time of 21.9 ± 5.5 minutes, the longest operative time was 38 minutes and the shortest operative time was 15 minutes. The mean postoperative length of stay was 2.5 ± 0.9 days, the longest postoperative length of stay was 5 days and the shortest was 2 days. Four children had persistent vomiting after feeding, which was considered to be due to pyloric mucosal edema. Therefore, the feeding dose was reduced, and the symptoms were relieved on the first and second postoperative days. There were no pyloric mucosal perforations, recurrent obstruction, surgical site infections, or incisional hernias. All patients had follow-up evaluations for at least 3 months, had good growth and development, and the parents were satisfied with the postoperative scars.
Discussion
With the constant improvement in medical technology, patients have an increasingly high demand for incision cosmesis, 12 thus the use of single-site umbilical laparoscopic operations has been a welcome addition. In 2010, Muensterer et al. first reported a single-site umbilical laparoscopic pyloromyotomy. 6 Subsequently, and with improved techniques, complications were reduced using the cross method. 13 In 2011, to reduce single-site laparoscopic complications, Bertozzi et al. reported a pyloromyotomy by delivering the pylorus using a single incision at the umbilicus with laparoscopy. 7 In 2012, to reduce the difficulty of single-site laparoscopic procedures, Kozlov et al. reported a laparoscopic pyloromyotomy with a single navel incision. 8 In 2014, Li et al. reported the experience with single-site umbilical laparoscopic treatment of children aged <21 days using a pyloric incision knife. 9 In 2015, Vahdad et al. reported the experience of conducting laparoscopic pyloromyotomy using a TriPort multichannel converter. 10 Different reports have their own advantages as well as limitations. In some surgical procedures the incisions are small, but the manipulations are difficult, whereas in other procedures the manipulations are easier although with a longer incision. At present, there is no consensus on which method is safest, most effective, and results in the most aesthetically acceptable incision. Based on the three-hole laparoscope and single-site laparoscope carried out in an earlier stage,14,15 to overcome the difficulty of single-site umbilical laparoscopic pyloromyotomy we adopted an innovative approach using a left-handed main operation and used an independently designed pyloric electrocoagulation chisel method. The pyloric electrocoagulation chisel is flat and blunt on the head end, can perform electrocoagulation cutting of the serosal layer of the pylorus, then chisel the muscular layer of the pylorus, which cannot damage the pyloric mucous membrane. Then, a horizontal rotation of the handle of the pyloric electrocoagulation chisel is performed and separation of the muscular layer of pylorus is expanded to be convenient for the pyloric separation grasper to enter and separate the pyloric muscular layer.
In our early stage, the operative time of three-hole laparoscopic pyloromyotomy was 30.5 ± 10.5 mm, the postoperative length of stay was 3.5 ± 0.5 mm, 14 but in this group of patients, the operative time was 21.9 ± 5.5 minutes, the shortest operative time was 15 minutes, the postoperative length of stay was 2.5 ± 0.9 days, the shortest was 2 days. We did not experience recurrent obstruction, pyloric mucosal perforation, or other severe complications. In addition, there were no occurrences of heat transfer or incision-related complications. We arranged for at least 3 months of follow-up care, and the parents were satisfied with the cosmetic effect of the incisions on the abdominal wall.
At present, the pyloric incision knife is the most widely used tool in transumbilical single-site laparoscopic pyloromyotomy. Our pyloric electrocoagulation chisel has overcome the shortcomings of the pyloric incision knife at the transumbilical single site. Because both the pyloric knife and the lens enter from the umbilical region, and the lens and the pyloric knife have a parallel relationship, 16 it is difficult to have direct vision of the knife head, thus challenging the operator to accurately position the distance between the knife head and the pyloric canal wall. As a result, there is increased operative time and uncertainty during the operation. In addition, the head of the pyloric knife is sharp, which is easy to cause mucosal perforations and incomplete incision of the pyloric circular muscle. 6 Because the pyloric knife has no hemostasis effect, increased bleeding will make it easy to obscure the operative field and a suction apparatus will need to be used repeatedly to aspirate blood. The repeated exchange of operative instruments will also increase the operative time. The pyloric electrocoagulation chisel cuts the pyloric serosal layer by electrocoagulation, which avoids bleeding and maintains clarity of the operative field. Only a very shallow serosal layer is cut by electrocoagulation, whereas for the remaining muscular layer, because the head end of the pyloric electrocoagulation chisel is blunt and flat, the muscular layer could be chiseled with great force without worrying about perforation. Using the width of the head end to rotate the muscular layer, the pyloric separation grasper can enter the muscular layer and separate the pyloric muscular layer.
At the time of a traditional three-hole laparoscopic pyloromyotomy,1,14,17,18 the left hand is used to fix the duodenum end of the pylorus, whereas the right hand is used for the main operation; however, because a single-site umbilical method is limited by vision and space, the procedure is relatively difficult. Therefore, Muensterer et al. suggested the concept of a cross, 13 but a cross always has a “chopsticks effect,” which increases the difficulty for beginners and requires a long learning curve.8,19 During the actual operation, we discovered that the stomach end of the pylorus was freer than the duodenum end, was more convenient to be fixed and dragged to require vision by the grasper, and was easy for our operating grasper and lens to reach an ideal operable status. Therefore, we changed to use right hand to drag and fix the stomach end with the grasper, and use the left hand for the main operation. This has changed the operating habit of the conventional three-hole method, however, compared with the “chopsticks effect,” as long as we can change the habit of the right and left hands slightly, it could be carried out. Therefore, it is easily accepted by beginners.
Although our findings have been satisfactory, our study had a retrospective design, was conducted in a single center, and involved only 25 patients. Therefore, our findings need to be verified by randomized controlled trials and more cases in the future. In addition, the satisfaction of the patients' parents regarding the incision scars has not been quantified.
To summarize, according to our preliminary experience with single-site umbilical laparoscopic pyloromyotomies using a technique with a pyloric electrocoagulation chisel combined with left-handed main operation facilitated improved completion of the operation, yielded good postoperative recovery, was safe and effective, and the parents were satisfied with the incision scars.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.