
Abstract
Background:
The aim of this study is to evaluate complications and costs in patients treated with laparoscopic and open method for common bile duct (CBD) stones. Secondary aim is to compare the effectiveness, safety, and outcomes of these methods. In addition, it is aimed to review the feasibility of laparoscopic method in rural areas.
Methods:
Seventy-one patients were analyzed retrospectively. Patients were divided into two groups as open and laparoscopic surgical method. These groups were analyzed comparatively in terms of complications and costs. Subgroups were formed from patients who underwent T-tube drainage, primary closure, and biliary anastomosis as choledochotomy management. As a secondary outcome, these three subgroups were investigated in terms of complications and cost.
Results:
The cost was lower in open method compared to laparoscopic method (484$, 707$, P = .002). There was no significant difference in postoperative complications between groups (P = .257). While the mean hospital stay was longer in the open group, the operation time was shorter (P = .002, P = .03). The mean length of hospital stay in the T-tube group was significantly higher than the primary closure (P = .001). The cost in the T-tube group was significantly higher than the primary closure and biliary anastomosis groups.
Conclusion:
Laparoscopic CBD exploration by experienced surgeons in endoscopic retrograde-cholangiopancreatography-limited settings is an effective and safe method in the treatment of choledocholithiasis. This procedure should not be limited to reference centers and should be performed safely in rural areas by well-trained surgeons.
Introduction
The gallstones are one of the commonest problems in modern health care system. The prevalence of gallstones happened to be around 15% and 10%–18% of patients who underwent cholecystectomy for gallbladder stones had also common bile duct (CBD) stones. 1 The method consisting of open common bile duct exploration (OCBDE) and cholecystectomy dominated until the three quarter of the 20th century in the management of cholecysto-choledocholithiasis. Gaining the popularity of endoscopic retrograde-cholangiopancreatography (ERCP) in the 1970s and subsequent development of laparoscopic cholecystectomy (LC), the management of choledocholithiasis has changed. 2 Endoscopic stone extraction/sphincterotomy followed by LC has become the standardized method of treatment for cholelithiasis and choledocholithiasis. With increasing expertise in laparoscopic procedures, many surgeons have been directed to LC and laparoscopic common duct exploration (LCBDE) in the same session as a single-step approach. LCBDE grew rapidly with the advantages of being a single procedure, maintaining sphincter functions, providing shorter hospital stay, being cost-effective, and lacking the complications of ERCP.3,4 Despite all these advantages, it was considered to be time consuming and difficult compared to ERCP and “old habit” of ERCP and LC has not been replaced in most surgical departments.5,6 For this reason, surgeons are at risk of losing their experiences in OCBDE and not being able to transfer them to new generation surgeons.
However, ERCP required heavily trained endoscopists with technical competence and the flouroscopic and endoscopic resources. Having mandatory to have protective room and clothing due to the use of radioactivity hinders to get used widespread. In many hospitals, although the laparoscopy is the main standard of the treatment, ERCP is present only in some centers. A cholecysto-choledocholithiasis patient needs to be transferred to ERCP-performing centers and then undergo LC. It requires a logistic arrangement causing financial, organizational, and psychological burden to the patients and health care system. Since LC is readily available in many centers, it is logical to institute LCBDE to overcome the difficulty of transferring the patients to centers and to teach residents LCBDE where they can perform in rural areas without ERCP facility. However, it was not clearly studied whether to institute such a practice in a surgical clinic without ERCP facility was a safe and feasible option.
The aim of our study is to evaluate the feasibility and efficacy of instituting LCBDE in a surgical clinic when ERCP was not available. We also compared the complications and costs in patients treated with laparoscopic and open method CBD exploration in the CBD stones.
Methods
Between January 2013 and December 2019, 71 patients who were operated for the CBD stone in the general surgery clinic of Gaziosmanpasa University Medical Faculty Hospital were retrospectively analyzed. Permission to use the clinical data of the patients was approved by the Ethics Committee of Gaziosmanpasa University Faculty of Medicine (20-KAEK-116). The patients' data were retrieved retrospectively from hospital database with International Classification of Diseases codes (K83.0, K83.1, K83.8). History, physical examination, laboratory results, radiology reports, surgical notes, and discharge reports of the patients were examined. Patients younger than the age of 18, patients with a history of malignancy, and patients without having the necessary data were excluded from the study.
The patients were divided into two main groups: OCBDE (Group A) and LCBDE (Group B). Age, gender, biochemical parameters (i.e., aspartate aminotransferase [AST], alanine aminotransferase [ALT], total, and direct bilirubin), CBD diameter, stone size in the CBD, American Society of Anesthesiology (ASA) score, preoperative ERCP history, hospital stay length, operation time, morbidity, and mortality data were recorded. In addition, patients in Group A and Group B were compared in terms of total cost. While calculating the cost, the amount invoiced to the social security institution was taken as reference, from the day patients were hospitalized to the day the patients were discharged from the hospital. Complications were classified according to Clavien–Dindo classification. 7 Accordingly, grade I and II complications were defined as minor, and grade III, IV, and V complications were defined as major complications.
In second part of the evaluation, the same patients were divided into 3 subgroups based on the operation on CBD: T-tube drainage, primary closure, and anastomosis. Among these groups, stone size, CBD diameter, duration of operation, length of hospital stay, and cost were investigated. Routinely 14–21 days after T-tube placement, T-tube cholangiography was performed. In patients with normal cholangiography, the T-tube was closed with a clip for 24 hours and removed when no bile leakage was noticed. ERCP procedure was applied for the patients with remaining stones.
Surgical technique
Our endoscopy unit is a tertiary referral center with advanced endoscopic procedures performed by both surgical and gastroenterological endoscopists. Our ERCP unit commenced in 2016. It was not functioning at times since there was no ERCP-performing endoscopist. Our department of surgery performed many laparoscopic major surgeries, including laparoscopic colorectal surgery in this center. LCBDE and OCBDE surgeries were performed by experienced surgeons.
Laparoscopic common duct exploration
Standard four-trocar method which is used for LC was performed. After obtaining critical view of safety in patients with gall bladder, the cystic artery was clipped and cut. Afterward, in all patients, intraoperative cholangiography (IOC) procedure was performed through cystic canal. Stones in the cystic canal, if any, were cleared. After detection of stones with IOC, choledochotomy was performed. The peritoneum on CBD was separated by blunt and sharp dissection. Choledoc was opened vertically by protecting three to nine arteries. The stones were removed from the incision with the help of basket and/or Fogarty catheters. Cholangiography was repeated for checking the presence of remaining stone. When suspected, distal and proximal bile ducts were examined with ureteroscopy. (There is no cholangioscope in our unit.) T-tube was used in the vast majority of patients. The T-tube was placed into the CBD as standard and the incision is closed with 4/0 pds sutures. T-tube cholangiography was performed intraoperatively to confirm choledocal opening and no remaining stones. Primary closure was performed in patients undergoing preoperative ERCP and sphincterotomy. CBD was generally intracorporeal sutured with 4/0 pds material. Biliary anastomosis was performed in patients with a big number of large and recurrent stone history.
In cases with open technique, choledochal exploration and other procedures were applied with conventional techniques by entering the abdomen through standard right subcostal incision. Subhepatic drainage catheter was placed in all patients.
Statistical analysis
SPSS statistical package program (SPSS, Inc., Chicago, IL) was used for data analysis. Shapiro–Wilk test was performed to assess the normality of data. Mann–Whitney U test was used to make comparisons between the parameters in each group that lacked normal distribution. Pearson chi-square and Fisher's exact test were used to compare the qualitative data. For the comparison of more than two groups, which were not normally distributed, Kruskal–Wallis test was performed. The results were evaluated at a 95% confidence interval, P < .05 significance level.
Results
Seventy-one patients (38 female and 33 male) were included to the study. The mean age of the patients was 65.38 ± 14.25. The means of AST, ALT, total bilirubin, and direct bilirubin were 123.67 ± 164.80 U/L, 98.10 ± 92.45 U/L, 2.84 ± 3.36 mg/dL, and 2.17 ± 3.02 mg/dL, respectively. The mean CBD diameter was 12.14 ± 4.7 mm and the mean CBD stone size was 11.90 ± 7.99 mm. The mean duration of surgery and hospital stay was 137.24 ± 48.97 minutes and 8.65 ± 3.46 days, respectively. There were 39 patients undergoing OCBDE (Group A) and 32 patients undergoing LCBDE (Group B).
AST was significantly higher in Group A (Table 1). While the rate of preoperative ERCP was 71.2% in laparoscopic method, it was 30.8% in open method and this difference was significant (P = .001) (Table 1). Other demographic, biochemical, and clinical parameters were similar (P > .05) (Table 1). It was observed that most of the patients with high comorbidity (ASA III and IV) were operated with OCBDE (n = 20 and 14).
Comparison of Demographic, Biochemical, and Clinical Data According to Surgical Methods
Chi-square test.
Fisher exact test.
Mann–Whitney U test.
Statistically significant P < .05 with Mann–Whitney U test.
ALT, alanine aminotransferase; ASA, American Society of Anesthesiology; AST, aspartate aminotransferase; CBD, common bile duct; ERCP, endoscopic retrograde-cholangiopancreatography; Max, maximum; Min, minimum.
Both the duration of surgery and hospital stay were significantly different between groups (P = .030, P = .002). Length of hospital stay in Group A (9.72 ± 3.70) was significantly higher than Group B (7.34 ± 2.65). The duration of surgery in Group B (149.28 ± 39.70) was significantly higher than Group A (127.36 ± 53.93) (Table 2).
Comparison of Choledochotomy Management, Complications, Mortality, and Cost According to Surgical Methods
Mann–Whitney U test.
Chi-square test.
Fisher exact test.
Statistically significant P < .05 with Mann–Whitney U test.
Max, maximum; Min, minimum.
In Group A, bile duct stones were successfully removed in all 39 patients. In Group B, bile duct stones were removed in 30 of 32 patients. Ductal clearance rates are 100% and 93.7%, respectively. Overall ductal clearance rate was 97.1%.
The cost in Group B was significantly higher than Group A (P = .002) (Table 2 and Fig. 1). Other parameters, including complications and mortality rates, were not statistically different between the groups (P > .05) (Table 2).

Comparison of costs between
In 3 patients who had undergone LCBDE, the procedure was converted to open technique. The reasons were bleeding, multiple impact stones that could not be removed, and severe adhesion with cholecysto-duodenal fistula. Major intraoperative complication was observed in 1 patient for each group. The complications were duodenum perforation (patient died due to sepsis) in Group A and uncontrolled bleeding caused by portal vein injury in Group B. In Group B, 2 patients had remaining stones and were removed by postoperative ERCP.
Postoperative complications were more common in Group A (41% and 28.1%), but it was not statistically significant. Minor complications were in the majority. Wound infections were treated with local interventions and antibiotherapy. Patients with major complications, including bile leakage and intra-abdominal abscess, were treated with percutaneous drainage methods and intravenous antibiotherapy. In both groups, 2 patients had surgical site infection after T-tube drainage and 1 patient had T-tube dislocation. No anastomotic leakage was observed. No patient underwent a second operation.
In Group A, 2 patients who were operated because of severe cholangitis had died because of bile leakage, sepsis, multiple organ failure, and Clavien–Dindo V. These 2 patients had high comorbidity (ASA IV) and they were in older ages (74 and 82).
Secondly, we compared T-tube drainage, primary closure, and biliary anastomosis subgroups after choledochotomy, independent of laparoscopic and open method. CBD stone diameter, CBD diameter, duration of surgery, and preoperative ERCP rates were not significantly different among these groups (Table 3). Length of hospital stay and costs were significantly different between groups. According to the post hoc tests, the length of hospital stay and costs were statistically higher in T-tube group than the primary closure group (P = .001, P = .036) (Table 3). Length of hospital stay and costs were higher in T-tube group compared to the anastomosis group, but it was not statistically different (Table 3). There was no significant difference in terms of the length of hospital stay and costs between the primary closure and anastomosis groups (Table 3). Both OCBDE and LCBDE costs were higher in T-tube group than primary closure and anastomosis groups (Fig. 2).
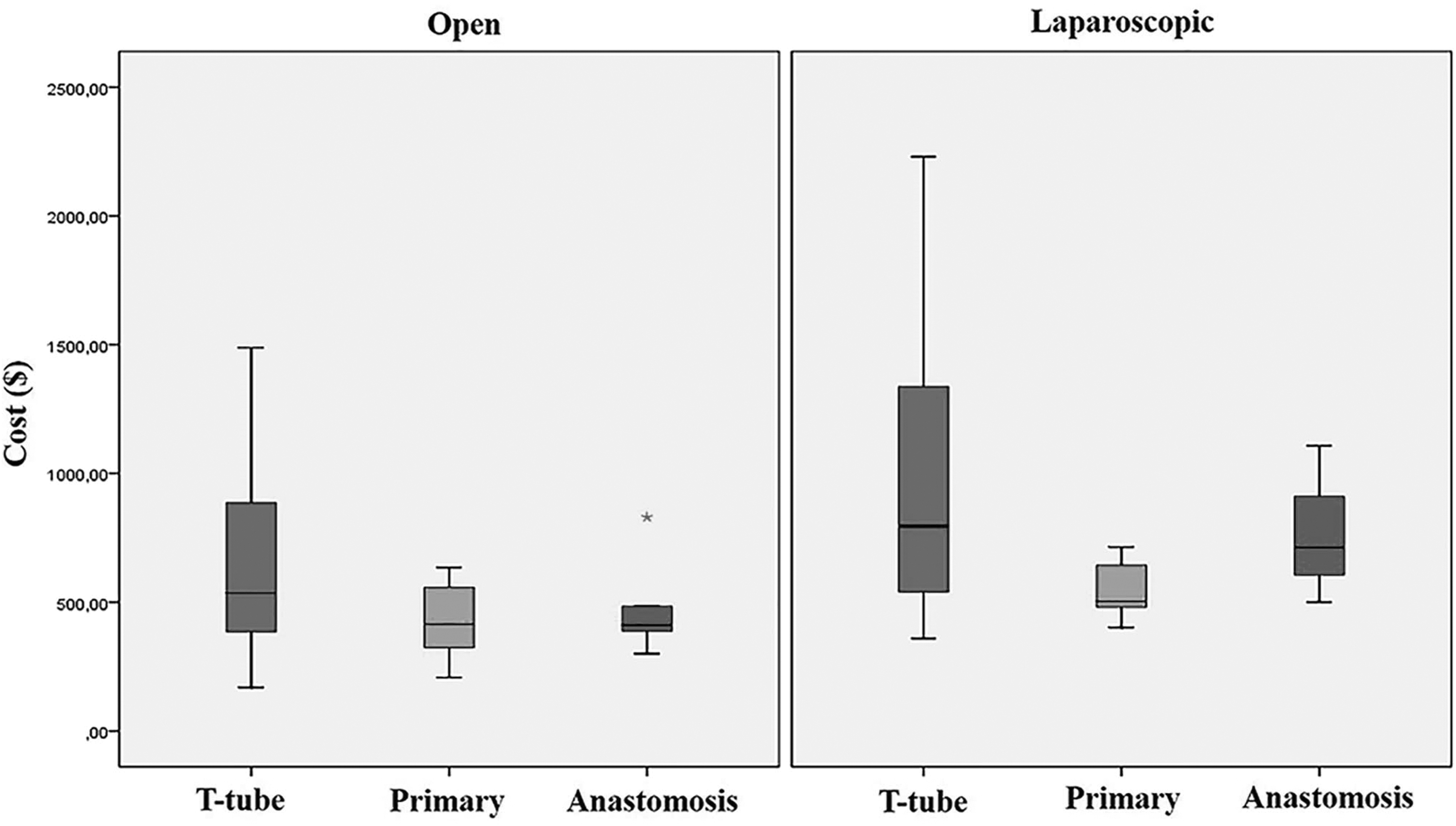
Comparison of costs between T-tube, primer, and anastomosis groups according to surgical methods. Asteriks: outliers.
Comparison of Choledochotomy Management, Complications, Mortality, and Cost Between Subgroups
Kruskal–Wallis test.
Fisher exact test.
CBD, common bile duct; ERCP, endoscopic retrograde-cholangiopancreatography; LCBDE, laparoscopic common duct exploration; Max, maximum; Min, minimum.
Preoperative ERCP was performed in 35 patients. The causes for ERCP failure were multiple/large (>2 cm) stones (n = 18), impacted stone (n = 10), unable to cannulate ampulla (n = 4), giant duodenal diverticula (n = 1), perforation of CBD, and impaction of basket catheter (n = 2). The reasons for not performing ERCP to other patients were mainly the lack of ERCP facility, the patients' desire for single operation, and also logistic and technical reasons. The diagnosis of CBD stones was based on preoperative physical examination, laboratory test, hepatobiliary ultrasonography, and magnetic resonance cholangiopancreatography. Sixty-seven of the patients had CBD stone with gall bladder stone and four of the patients had gall bladder operation and CBD stone.
In Group A, choledochoduodenostomy (n = 2), Roux-en-Y hepaticojejunostomy (n = 3) and in Group B choledochoduodenostomy (n = 2), and choledochojejunostomy (n = 1) were performed as biliary anastomosis methods.
Discussion
Management in patients with choledocholithiasis is still controversial. 8 In our study, the patients with choledocholithiasis who underwent surgical treatment in a university hospital were examined. The complication rate and the length of hospital stay with laparoscopic CBDE were significantly higher compared to the patients operated with the open approach. Beside, the operation time and cost were also higher in the laparoscopic group. Although there were no remaining stone in open technique, 2 patients in laparoscopic technique had remaining stone (ductal clearance 93.75%).
The first treatment option in CBD stones was ERCP and subsequent cholecystectomy. On the contrary, LBCDE when performed by an experienced surgeon, is as effective and safe as other methods of choledocholithiasis treatment.9,10 Many rural hospitals do not have the equipment and experienced staff for endoscopic treatment of choledocholithiasis. Thus, it requires the patient to be transferred to the appropriate centers, resulting delay in the treatment of the patient, increased cost, and logistical problems. The presence of well-trained surgeons in LCBDE in a rural hospital where LC can be performed technically is enough to make the treatment of choledocholithiasis possible in most cases. Our hospital is a reference center and training hospital in a university, which serves a population of ∼600,000 people. However, ERCP was interrupted from time to time due to either the lack of technical equipment or the lack of physicians who would perform the procedure or both. During that time period, LCBDE was performed by experienced surgeons. In addition, LCBDE was applied in patients who had failed ERCP performed in other hospitals or elsewhere. The results of LCBDE in our study are consistent with previous studies. These studies found the morbidity rate of LCBDE as 3.7%–33%, mortality rate as 0.3%–0.8% and ductal clearance rate as 85%–97.3%.11–14
In our study, it was revealed that LCBDE had higher costs than OCBDE. Cost-effectiveness research has not been studied explicitly in literature. In a prospective randomized study conducted in 2017, LCBDE, ERCP, and OCBDE costs had been compared. In this study, while costs were similar in open and laparoscopic methods, it was shown that ERCP cost was high. 15 Cost analysis differs depending on the countries' health systems, insurance, and payment policies. 16 In our study, we found higher costs in the laparoscopic group compared to the open group, as well as in the T-tube group compared to the primary closure and anastomosis groups. This might be because of the higher cost of laparoscopic equipment in our country. Another reason could be that we have done a total cost analysis which was invoiced to the social security institution. This included everything from patient admission to the discharge or death. It also included ERCP, if performed. Because a single ERCP-performing endoscopist with limited experience has performed the procedure most of the time, ERCP-failure might have more common in our unit than fully developed ERCP units. Since the patients were not randomized, there could be some biases in patient selection, procedure selection, and so on. Therefore, a healthier comparison could be made by randomization of the two arms of patients. However, our study might be considered to be useful to reflect the “de facto” situation in our settings. The reason why the cost in T-tube group was high could be explained by the longer length of hospital stay and higher complication rates.
After removing the bile duct stone, T-tube, primary closure and anastomosis methods can be used for drainage. We used T-tube in 64.7% of patients, primary closure in 23.9%, and biliary anastomosis in 11.2%. Traditionally, as the most commonly used method, T-tube aims to create a controlled bile fistula by reducing biliary tract pressure. However, this method has many complications such as bile leakage, peritonitis, T-tube dislocation or obstruction, sepsis. In addition, the fact that the patient stays with the drainage catheter for a long time reduces patient comfort, increases the risk of complications and costs.17,18 In recent years, primary closure method with lower complications and higher success rates have been used. However, this technique requires advanced laparoscopic experience. 19 Although the trend shifts toward the primary closure method, this is still controversial. Many studies have confirmed that primary closure without T-tube after removing the CBD stone is safer and associated with a lower complication rate.20,21 In a prospective randomized study of 80 patients, the T-tube was used in the first half and the primary closure was used in the second half. Postoperative hospital stay (5.2 ± 2.2 versus 8.3 ± 3.6 days) and time to return to work (12.6 ± 5.1 versus 20.4 ± 13.2 days) were found to be lower in the primary closure group. In addition, hospital expenses (8.638 ± 2.946 versus 12.531 ± 4.352 yuan) were stated to be significantly lower in the primary closure group compared to the T-tube group. 22 In our study, the length of hospital stay was found to be significantly higher in patients who were treated with T-tube. The operation time was longer in primary closure than the other two methods. The complication rate of T-tube was found to be high, which is compatible with the literature.
This study has some limitations. First of all, the study had a retrospective design and was conducted in a single center. Second, cost analysis was performed upon Turkey's health care system, so it cannot be generalized. Third, we also took into account the total cost, including the services such as ERCP. However, a better comparison with ERCP with subsequent LC and LCBDE could provide more accurate data about the cost. Also, the pricing of services and materials differs in international health systems.
It was discussed that, LCBDE is increasingly used by surgeons, thus it should take a part in their training.23–25 The variables checked in our study such as cost, morbidity, and length of stay were all higher in LCBDE compared to OCBDE in patients with CBD stones. But, our study still has a clinical impact in providing a management option where ERCP cannot be performed due to the limited resources. Our study is not a sole comparison between ERCP/LC approach and LCBDE, since ERCP was also performed in some cases of LCBDE. It should be emphasized that we prefer to use ERCP/LC approach in our clinic. In highly selected cases, we offer LCBDE to the cholecystolithiasis patients with nonimpacted small CBD stones as it is one-step procedure. Our study showed that the LCBDE in limited-resourced places can be performed safely and effectively with the caution of acceptable increase in morbidity, length of hospital stay, and cost. Therefore, the residents should be trained to perform LCBDE in the surgical departments where they have their trainings. CBDE is an important component of surgical armamentarium and it should be performed laparoscopically when necessary. This study is expected to contribute to the understanding that when the conditions necessitate (i.e., ERCP cannot be performed and the patient transfer is rather difficult), the surgeons who had training has an option to perform LCBDE in selected cases.
In conclusion, the use of LCBDE by well-trained surgeons in regions with limited equipment for ERCP is a safe and feasible method, although the cost, morbidity, and length of stay are increased.
Ethical Standards
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Declaration of Helsinki 1964 and later versions. Informed consent to be included in the study, or the equivalent, was obtained from all patients.
Footnotes
Authors' Contributions
M.Y. and I.O. planned the study, M.Y., U.O. and A.K. collected the data, M.Y., F.D. and E.D. drafted the article and, I.O. did the revision of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.