
Abstract
The current unprecedented coronavirus 2019 (COVID-19) crisis has accelerated and enhanced e-learning solutions. During the so-called transition phase, efforts were made to reorganize surgical services, reschedule elective surgical procedures, surgical research, academic education, and careers to optimize results. The intention to switch to e-learning medical education is not a new concern. However, the current crisis triggered an alarm to accelerate the transition. Efforts to consider e-learning as a teaching and training method for medical education have proven to be efficient. For image-guided therapies, the challenge requires more effort since surgical skills training is combined with image interpretation training, thus the challenge is to cover quality educational content with a balanced combination of blended courses (online/onsite). Several e-resources are currently available in the surgical scenario; however, further efforts to enhance the current system are required by accelerating the creation of new learning solutions to optimize complex surgical education needs in the current disrupted environment.
Introduction
The current unprecedented coronavirus 2019 (COVID-19)
During the so-called transition phase, 1 efforts were made to reorganize surgical services, reschedule elective surgical procedures, surgical research, academic education, and careers to optimize results. Simultaneously, the protection of patients and health care workers remained the priority according to quality and safety procedures. 2
Furthermore, to enforce social distancing measures, ∼1.2 billion students were out of classrooms during the pandemic. 3 Large-scale efforts to support distant learning are emerging and evolving rapidly, involving all levels of education. Even before the pandemic, the issue of distant access to education and e-learning gathered the interest of the academic world. According to a report of recent global market analysis, the e-learning market size was in excess of $200 billion USD in 2019, and it is expected to grow at an annual rate of >8% between 2020 and 2026. 4 As a result, financial efforts to switch to e-learning, mobile e-learning, rapid e-learning, and virtual classrooms whenever possible and appropriate are currently under discussion.
For >190 years, scientific societies have held conventions and meetings 5 with the intent of making science more accessible to everyone and establish research collaborations and scientific networks. Such events have been considered one of the most effective knowledge transfer and sharing methods in education. Hence, the creation of new blended (on-site/online) educational models may be not only an ideal replacement of on-site scientific gathering but also an ambitious move to take knowledge transfer and sharing to the next level of globalization.
Online survey-based studies performed during the COVID-19 crisis have underscored the intention to switch to online formats (including virtual meetings, webinars, and research collaborations) after the pandemic. 6 Surgical education is reported to be one of the most complex educational models even before the COVID-19 outbreak. Ways in which the enforced situation may fit surgical training remain challenging. Major key questions are raised, and notably whether and how much surgical training can be completed using remote education only, and how much e-learning can enhance surgical skills. Indeed, conventional surgical training includes clinical skills usually acquired on-site during preoperative and postoperative periods, as well as surgical technical skills to be learned in the laboratory and in the operating room and, recently, on virtual simulators (on-site or remote).
The question related to the prevalence of this disrupted educational environment during the full COVID-19 recovery is hard to answer. Epidemiological forecasts, even if they are often imprecise, demonstrate that intermittent social distancing measures may be necessary until 2022. 7 Consequently, surgical educational disruption may not be over yet. In contrast, there are groups of researchers who claim that COVID-19 will hopefully decline soon. And yet, virtual learning in surgical education should prevail as a priority set on the agenda of surgical leaders. 8
The intention to switch to on-line medical education is not new. However, the current crisis triggered an alarm to accelerate the transition. Efforts to consider e-learning as a teaching and training method for medical education have proven to be efficient 9 and have demonstrated that health care professionals may improve their academic performance when a blended learning style is adopted when compared with traditional teaching methods. 10 The advantages of surgical e-learning are summarized in Table 1.
Advantages in Surgical e-Learning
Open issues are present in the switch toward surgical e-learning such as limited student feedback, lack of accelerated course certification, scientific and quality content, trainee self-motivation, and commitment. 11 The main challenges for surgical e-learning are summarized in Table 2.
Challenges in Surgical e-Learning
Educational Methods
Several e-resources are currently available in the surgical scenario. A recent review summarizes currently active operating room simulation and e-learning platforms, which can be accessed either through web-based or through mobile phone applications, thereby promoting remote surgical learning. 12
The IRCAD/IHU, the Strasbourg experience
The expertise of the Research Institute Against Digestive Cancer (IRCAD, France) was further leveraged and shared in the 2000s when WebSurg, its online university dedicated to minimally invasive surgery, was created. WebSurg aims to publish academic content in several surgical specialties. Currently, >4000 educational videos are available on a multilingual platform. As a result, the largest community of surgeons is brought together, currently gathering 417,121 registered members. The platform also offers free-of-charge live webinars and live conference streaming.
For image-guided therapies, the challenge needs to double efforts since surgical skills training is combined with image interpretation, thus the challenge is to cover quality educational content with a balanced combination of blended courses (online/onsite). To overcome this difficulty, IRCAD/IHU (Image-Guided Surgery Center) dedicates blended programs for training in minimally invasive surgery procedures (including image-guided education).
Image-guided surgical e-learning
Image-guided surgery techniques cover a wide range of minimally invasive procedures, including percutaneous (needle-based), laparoscopic, robot-assisted, and flexible endoscopy approaches.
Image-guided needle-based procedures have minimally invasive advantages and comparable outcomes with open surgery approaches. Consequently, they are gaining in popularity for diagnostic and therapeutic fields, including good clinical standards in different specialties and diseases (e.g., liver ablation).
To date, liver ablation is considered to be the first-choice treatment for unresectable liver tumors and it is also accepted as an alternative to surgical resection in single and small (<2 cm) hepatocellular carcinoma (HCC). 13 Planning and guidance of image-guided needle-based procedures are becoming a fundamental part of the daily workflows of the health care professionals involved, and such skills are more frequently required. In addition, image-guided needle-based procedures have steep learning curves, and growing evidence shows that it should be forbidden to perform them without the necessary set of skills. Studies have shown that skills assessment in interventional procedures is appropriately completed with the use of virtual simulators. 14 Consequently, several driving forces are associated with the breakthrough of virtual simulation and e-learning in image guidance techniques, as reported in Table 3.
Driving Forces Associated with the Breakthrough of Virtual Simulation and e-Learning in Image Guidance Techniques
Image-guided simulation trainers for percutaneous and endoscopic procedures
Currently, there is no standard training tool nor skills assessment platform for the ultrasound and computed tomography (CT) image-guided needle-based procedures in the liver. As a result, the development of a comprehensive percutaneous simulator, allowing for the on-site and remote simulation of needle-based procedures, is a priority.
Education and training in percutaneous procedures require perceptual, visuospatial, and psychomotor skills, 15 as well as hand–hand and hand–eye coordination, planning of realistic workflows, oncological planning, procedural advanced imaging interpretation, and basic guidance system knowledge. The assessment of fundamental percutaneous skills, low-cost simulation, performance analytics, and later data acquisition to train artificial intelligence systems to assess learners' skills even remotely is one milestone at the Institute of Image-Guided Surgery (IHU), Strasbourg, France. The expertise of the IHU with e-learning solutions has been running along since 2017, with the conception of the EVE-evolving education platform, * which was created to promote medical innovation and deliver personalized hybrid (online/on-site) training programs while establishing research networks. So far, three university curricula are available for blended surgical endoscopy, imaging, and percutaneous techniques surgical training.
To deliver cognitive and practical knowledge, the e-learning model was complemented with remote simulation platforms, which may enhance the content. To maximize the chances of success of remote simulation learning, the simulators were designed to be low cost, plug, and play technology in the form of serious games.
This new teaching strategy has the ambition to provide a totally different learning environment, which hides in a surreal and engaging package, a very realistic and thorough simulation of endoscopic gestures extrapolated and tuned from authentic clinical scenarios. A gaming environment and a playful universe can easily overcome the boredom perceived by users when training on current clinical simulators, increasing the learning process and amount of time spent in training through competition and satisfaction.
To further develop the remote learning strategy, microlearning was added to the curriculum of the image-guided ablation therapies courses; microlearning can be defined as an educational approach that offers bite-sized small learning units with just the necessary amount of information to help learners achieve a goal. This growing e-learning modality has been used in several fields including business, language learning, and management. Since the advent of image-guided therapies, knowledge acquisition may be challenging. The conception idea is to offer a new progressive web-app tool, which can group learning materials in the form of bite-sized information cards to be accessed by surgeons precisely when they need it. This would allow for just-in-time learning, avoiding mental fatigue, and reinforcing concepts before surgeons lose their motivation, and this is one of the educational goals of the IHU (Strasbourg, France). Although trainees can quickly hold important concepts in self-paced learning, the training content is personalized and easily handled, simplifying the learning acquisition.
Ablation therapies virtual bootcamps
During the emergency phase of the COVID-19 pandemic (April and May 2020), the average number of surgical videos viewed on the WebSurg platform was 1161 views per month versus 161 views per month in the same period in 2019 (+621%). During the same time period, a worldwide web-based survey was carried out among WebSurg members for 2 weeks addressing the question of which education means would be the most desirable during the lockdown. More specifically, the question was the following: “How would you like to meet your training and educational needs during this challenging period until all COVID-19 restrictions are lifted again?” In a total of 4459 responders, 1731 (38.82%) replied virtual conference/online courses with the experts, 614 (13.76%) preferred webinars with faculty experts, and 1038 (23.27%) were in favor of a dedicated website. Overall, 75% of the participants expressed the importance of using e-learning surgical methods until restrictions are lifted. The results of the survey are summarized in Table 4.
An Online Survey Regarding Surgical e-Learning
Source: WebSurg.com
COVID-19, coronavirus 2019.
In light of these results, we sought to create an image-guided surgery blended course with the intent to provide new trainees with an interactive learning pathway. The aim is to initiate and mentor participants on this topic through e-learning meetings ahead of on-site hands-on courses during the COVID-19 pandemic.
Virtual bootcamps in ablation therapies are included in an e-learning pathway dedicated to complement the educational content of image-guided therapies on-site programs at the IHU. Radiofrequency ablation has emerged as a first-line curative treatment approach for patients with small HCC lesions.
The diagnosis, identification, and treatment of such small tumors may be challenging. The evaluation of the treatment success or curative intent includes several factors that may affect the oncological success, including the following: (1) precision during insertion of ablation electrodes, (2) technical limitations of conventional CT or ultrasound-guided techniques, (3) single or multiple-needle approaches using three-dimensional treatment planning and stereotactic needle placement, (4) different thermal techniques used (radiofrequency, microwave, and cryoablation), and (5) visualization of tumor size. The previously mentioned challenges in ablation therapies are not clear for daily clinical practice. Theoretical courses may complement the understanding of such complex approaches.
Conclusions
e-Learning may impact surgical education in a different way, according to established educational objectives. Although undergraduate education at medical schools is mainly theoretical, residency and fellowship programs are primarily based on hands-on/technical skills. Yet, e-learning solutions, as for the IRCAD/IHU experience, can bring benefits to every surgical learner, despite their different learning desired outcomes. A true balance for optimizing hybrid courses that may impact surgical education should be found, as summarized in Figure 1.
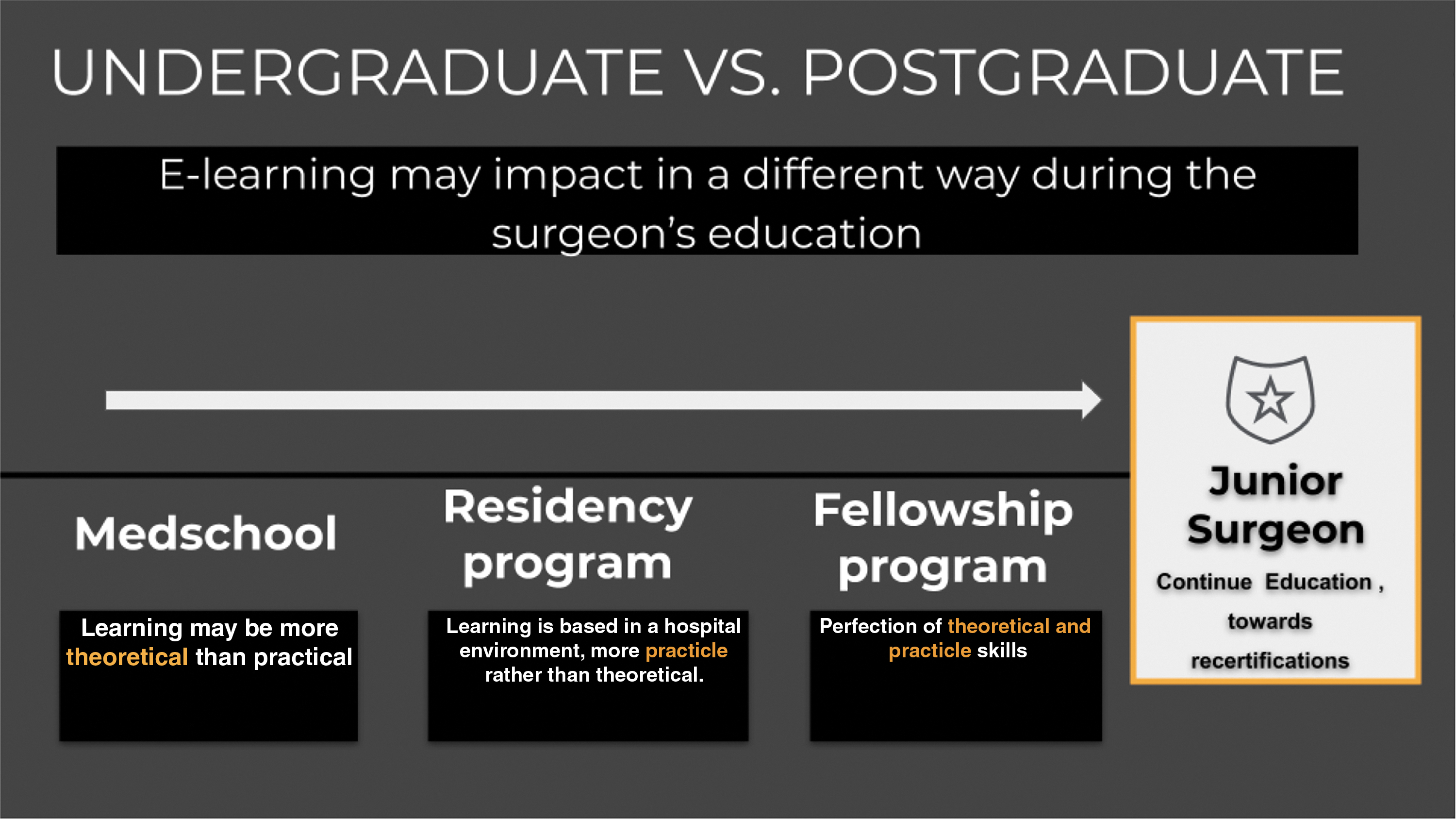
E-learning may impact surgical education in a different way.
e-Learning for surgical education may be considered a robust educational method for experienced surgeons, as well as students and residents. Further efforts to enhance the current system are required by accelerating the creation of new learning solutions to optimize complex surgical education needs in the current disruptive environment.
Footnotes
Acknowledgments
The authors are grateful to the WebSurg team: Thomas Parent, Margaux Diebold, Guy Temporal, and Christopher Burel.
Disclosure Statement
A.G.V., J.M.V., F.D.M., M.P., L.C., B.D., and S.P. declare no competing financial interests exist. J.M. is president of IRCAD, France, which is partially funded by Karl Storz and Medtronic; B.G. is the CEO of the IHU, Strasbourg France; and M.E.G. is a Medtronic and Siemens Healthineers Advisor.
Funding Information
This study benefited from state aid managed by the French National Research Agency (ANR) under the “investissements d'avenir” program with the reference ANR-10-IAHU-02.