
Abstract
Introduction:
Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) has been described to treat hepatocellular carcinoma (HCC) but burdened, in its pioneering phase, by high morbidity and mortality. With the advent of minimally invasive (MI) techniques in liver surgery, surgical complications, including posthepatectomy liver failure (PHLF), have been dramatically reduced. The primary endpoint of this study was to compare the short-term outcomes of MI- versus open-ALPPS for HCC, with specific focus on PHLF.
Methods:
Data of patients submitted to ALPPS for HCC between 2012 and 2020 were identified from the ALPPS Italian Registry. Patients receiving an MI Stage 1 (MI-ALPPS) constituted the study group, whereas the patients who received an open Stage 1 (open-ALPPS) constituted the control group.
Results:
Sixty-six patients were enrolled from 12 Italian centers. Stage 1 of ALPPS was performed in 14 patients using an MI approach (21.2%). MI-ALPPS patients were discharged after Stage 1 at a significantly higher rate compared with open-ALPPS (78.6% versus 9.6%, P < .001). After Stage 2, major morbidity after MI-ALPPS was 8.3% compared with 28.6% reported after open-ALPPS. Mortality was nil after MI-ALPPS. Length of hospital stay was significantly shorter in MI-ALPPS (12 days versus 22 days, P < .001). Univariate logistic regression analysis (Firth method) found that both MI-ALPPS (odds ratio [OR] = 0.05, P = .040) and partial parenchymal transection (OR = 0.04, P = .027) were protective against PHLF.
Conclusion:
This national multicenter study showed that a less invasive approach to ALPPS first stage was associated with a lower overall risk of PHLF.
Introduction
The issue of reducing the risk of posthepatectomy liver failure (PHLF) has been widely addressed—especially when focusing on surgery for hepatocellular carcinoma (HCC)—because PHLF constitutes the most life-threatening complication in hepatic surgery. In HCC indeed, on the one hand, the indication to perform anatomical resections is strongly recommended for oncological reasons 1 and it is associated with the high prevalence of involvement of major portal branches leading to the need of major hepatectomies with significant parenchymal sacrifice and drastic reduction of vascular bed. 2 On the other hand, the impairment of parenchyma in patients with underlying liver disease, limits the functional reserve of these patients making their tolerance to surgery poor and enhancing surgery-related risk in extensive demolitions. 3
In an attempt to broaden the curative chances for patients with HCC by increasing their resectability rate using methods to induce hepatic hypertrophy,4,5 associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) technique has been also explored, confirming the efficacy and reproducibility of this method in the setting of primary tumors arising on liver-related disease.6–8
Along with the diffusion and the precise study of the fields of application,9,10 the laparoscopic technique has gained an ever-increasing interest also in this field of liver surgery,11,12 taking into account the strong level of evidence in the literature supporting the reduction of postoperative complications in laparoscopic compared with open HCC surgery.13,14
The primary endpoint of this study was therefore to compare the short-term outcome of minimally invasive (MI) versus open-ALPPS for HCC performed within the national perspective series of the ALPPS Italian registry, with specific focus on PHLF. Secondary endpoints were the identification of protective and risk factors for PHLF within the whole series of ALPPS for HCC and the analysis of mid-long-term outcomes.
Materials and Methods
Study design
Data of patients submitted to ALPPS for HCC between September 2012 and January 2020 were identified from the ALPPS Italian Registry, described in detail elsewhere. 15 In brief, it is a prospective intention-to-treat Registry open to inclusion of cases from any Italian center performing ALPPS, without any restriction criteria based on the numerosity of performed procedures.
Patients with the following characteristics were included in this study and constituted the study population: histologically proved diagnosis of HCC (mixed hepatocholangiocellular forms were excluded); undergoing at least first stage of the ALPPS procedure (intention-to-treat analysis); and at least 3 months of follow-up.
Patients were stratified in groups according to approach (MI versus open): the patients receiving an MI Stage 1 (MI-ALPPS) constituted the study group, whereas the patients who received an open Stage 1 (open-ALPPS) constituted the control group. MI-ALPPS and open-ALPPS groups were compared and analyzed to address the primary and the secondary endpoints.
The Italian ALPPS registry was approved by the ethical committees of each center. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki (6th revision, 2008) as reflected in a priori approval by the institution's human research committee. Informed consent was obtained from each patient included in the study.
Variables
The main outcome of this study was Grade B/C PHLF, according to the International Study Group of Liver Surgery (ISGLS) definition. 16 Clinically significant portal hypertension (CSPH) was defined as the presence of esophageal varices and/or platelet count <100 × 103/mL in association with splenomegaly. 17 All surgical complications, defined as any deviation from the ordinary postoperative course occurred before discharge, were recorded and scored using the comprehensive complication index (CCI), ranging from 0 (uneventful course) to 100 (death). 18 Major morbidity was defined as Grade ≥3a, according to Clavien–Dindo classification. 19 Mortality was defined as any death occurring during the interval of both stages or within 90 days after Stage 2.
All patients were routinely discussed during multidisciplinary council and ALPPS was considered in patients with a good performance status (Eastern Cooperative Oncology Group performance score 0/1) and preserved liver function reserve, as indicated by Child–Pugh Grade A, without preoperative signs of ascites or encephalopathy. Standard preoperative evaluation included physical examination, routine laboratory testing, and alpha-fetoprotein (AFP) serum levels. Liver remnant volumes were assessed using cross-sectional imaging by computed tomography and standardized future liver remnant (FLR) was assessed in each patient using the Vauthey formula: −794.41 + 1267.28 × body surface area (m2). 20 FLR/BW (body weight) was calculated as the ratio (%) between FLR volume and patient's BW, assuming a mean physical liver density of 1.00 g/mL. 21 Percentage increase of the FLR volume was calculated as follows: (FLR interstage − FLR baseline)/FLR baseline. The kinetic growth rate (KGR) was calculated as the mean daily volumetric increase, expressed as volume percentage increase/day (%/day) from the date of the portal vein occlusion to the last radiological assessment before the second stage of ALPPS, assuming a linear growth model. 22
In case of insufficient hypertrophy after Stage 1, an additional volumetry was performed until a sufficient FLR volume was achieved. Whenever interstage hepatobiliary scintigraphy (HBS) was performed together with liver volumetry, liver function was also assessed before proceeding to Stage 2. 23
Overall survival (OS) was defined as the time from the first stage of ALPPS to the date of death or the last follow-up, whereas disease-free survival (DFS) was defined as the time from the first stage of ALPPS to the date of recurrence or the last follow-up.
Statistical analysis
Continuous variables were expressed as the median and interquartile range (IQR). Categorical data were expressed as numbers (percentages). For group comparisons of categorical and continuous variables, chi-square test or Mann–Whitney test were used, as appropriate. Univariate logistic regression analyses were performed to predict the risk of developing a clinically significant PHLF. After evaluation of multicollinearity, multivariable logistic regression analysis was carried out on the variables that reached P < .05 at univariate analysis. To allow for the convergence to finite estimates in conditions of separation because of the rarity of some of the potential outcomes, a penalized Firth logistic regression was used. 24
All statistical tests were two-tailed, and differences were considered significant at a value of P ≤ 0.05. Statistical analysis was performed with STATA/SE (Version 15.1; Stata Corp, TX) for Windows.
Results
Baseline characteristics
Sixty-six patients enrolled from 12 Italian centers fulfilled the inclusion criteria and were therefore enrolled in this study. MI-ALPPS was performed in 6 of 12 centers with experience in laparoscopic and/or robotic liver surgery (i.e., completed learning curve in MI liver resections). Background characteristics of the entire cohort are given in Table 1. Half the patients (n = 33) were operated before 201625 and the remaining half thereafter. Median age of the patients at the time of surgery was 64 years (range 24–82). Viral etiology and hepatitis C virus infection were the most common causes of chronic hepatitis/cirrhosis. CSPH was present in 5 patients (7.6%). Portal vein tumoral thrombosis was preoperatively documented in 27 patients (40.9%), whereas ALPPS was considered because of failed portal vein embolization (PVE) in 4 patients (6.1%).
Baseline Features of Overall Study Population and by Comparing Open and Minimally Invasive Approach
AFP, alpha-fetoprotein; ALPPS, associating liver partition and portal vein ligation for staged hepatectomy; ASA, American Society of Anesthesiologists; BMI, body mass index; BW, body weight; COPD, chronic obstructive pulmonary disease; CSPH, clinically significant portal hypertension; DMT2, diabetes mellitus type 2; FLR, future liver remnant; HBV, hepatitis B virus; HCV, hepatitis C virus; IQR, interquartile range; MELD, model for end-stage liver disease; MI, minimally invasive; NAFLD, nonalcoholic fatty liver disease; PVE, portal vein embolization; PVTT, portal vein tumoral thrombosis; sTLV, standardized total liver volume.
Stage 1 of ALPPS was performed in 14 patients (21.2%) using an MI approach (MI-ALPPS: 13 laparoscopic, 1 robotic), whereas 52 patients by open approach (open-ALPPS). Baseline characteristics of open-ALPPS versus MI-ALPPS are given in Table 1.
Perioperative outcomes (Stage 1)
Surgical details and operative outcomes are summarized in Table 2. With regard to the surgical technique, partial parenchymal transection (PPT) was performed more frequently in the MI group (78.6% versus 7.7%, P < .001) as well as PVE, which was carried out only in MI-ALPPS. Pringle maneuver was required in 71.4% of all MI cases compared with the open approach in which clamping of hepatic hilum was performed in 17.3% of cases (P < .001). Operative time did not differ between the two groups (P = .677) as well as postoperative complications or Grade B/C PHLF. Conversion rate from MI to open approach during Stage 1 was nil. When Grade A was also included, incidence of PHLF in open-ALPPS was nearly double compared with MI-ALPPS (28.8% versus 14.3%, P = .289). Using an MI approach, a significantly higher rate of patients (78.6% versus 9.6%, P < .001) was discharged home after the first stage in a median of 5 days (IQR = 4–9).
Perioperative Outcomes of Stage 1 of Overall Study Population and by Comparing Open and Minimally Invasive Approach
ALPPS, associating liver partition and portal vein ligation for staged hepatectomy; BW, body weight; CCI, comprehensive complication index; CT, computed tomography; FLR, future liver remnant; IQR, interquartile range; KGR, kinetic growth rate; MI, minimally invasive; PHLF, posthepatectomy liver failure according to Grade B/C ISGLS (International Study Group of Liver Surgery) criteria; PVE, portal vein embolization; PVL, portal vein ligation; PVO, portal vein occlusion; RBC, red blood counts; sTLV, standardized total liver volume.
Perioperative outcomes (Stage 2)
After a median of 7 days (IQR = 6–14), FLR increased by 39.3% (IQR = 22.9–65.5). FLR volume increase was higher after MI-ALPPS compared with open-ALPPS (62% versus 34%, P = .069) but at a slower rate (3.7%/day versus 5.1%/day, P = .140) (Table 1). Similarly, FLR increase was significantly higher (P = .037) after PTT (61.6%, IQR = 42.7–77.2) compared with total parenchymal transection (34.1%, IQR = 22.6%–61.6%) along with a similar rate of regeneration (3.9% versus 4.7%, P = .486).
Before completion of Stage 2, FLR/sTLV (standardized total liver volume) and FLR/BW were comparable between the two groups (MI versus open, P = .453 and P = .442, respectively) also when considering only patients with liver cirrhosis (38.2% versus 39.6% and 0.85 versus 0.80, P = .587 and 0.549, respectively).
Five patients did not complete the second stage of ALPPS. Reasons for dropout were insufficient liver hypertrophy (n = 1), progression of disease (n = 2), and intraoperative complications occurred during Stage 2 (n = 2). The remaining 61 patients underwent completion surgery in a median of 9 days (IQR = 7–17) after the first stage: second stage was performed in median 20 days after Stage 1 in MI-ALPPS group compared with 8 days in the open-ALPPS group (P < .001) (Table 3). Among MI-ALPPS, completion of hepatectomy was approached using MI techniques in 7 patients (6 laparoscopic, 1 robotic). Two (laparoscopic) procedures were converted owing to bleeding (n = 1) and oncological concerns (n = 1). Right extended hepatectomies were carried out more frequently in MI-ALPPS group compared with open-ALPPS group (75% versus 32.7%), whereas operative time was in median significantly longer after MI approach (305 minutes versus 190 minutes, P = .004). Median CCI points were significantly increased after open surgery (20.9 versus 0, P = .001). Major morbidity after MI-ALPPS was 8.3% compared with 28.6% reported after open-ALPPS, whereas mortality was nil after MI-ALPPS without reaching statistical significance (P = .164). Length of hospital stay was significantly shorter in MI-ALPPS (12 days versus 22 days, P < .001).
Perioperative Outcomes of Stage 2 of Overall Study Population and by Comparing Open and Minimally Invasive Approach
ALPPS, associating liver partition and portal vein ligation for staged hepatectomy; CCI, comprehensive complication index; IQR, interquartile range; MI, minimally invasive; PHLF, posthepatectomy liver failure according to Grade B/C ISGLS (International Study Group of Liver Surgery) criteria; RBC, red blood counts.
With regard to histology, underlying liver fibrosis/cirrhosis according to METAVIR score differed significantly between the two groups (P = .009): cirrhosis was present in 68.9% of patients in open-ALPPS group compared with 25% in MI-ALPPS group. Size and number of nodules were comparable between the two groups as well as Edmonson grade and presence of microvascular invasion (Table 3).
Risk factor analysis
Univariate logistic regression analysis (Firth method), examining the effect of patient and surgical factors on the development of PHLF, found a significantly protective effect from both MI-ALPPS (odds ratio [OR] = 0.05, 95% confidence interval [CI] = 0.002–0.87, P = .040) and PPT (OR = 0.04, 95% CI = 0.002–0.69, P = .027). Multivariate analysis did not show any independent predictors of PHLF (Table 4).
Univariate and Multivariate Penalized Firth Logistic Regression for Factors Potentially Associated with Posthepatectomy Liver Failure
BW, body weight; CI, confidence interval; FLR, future liver remnant; HBS, hepatobiliary scintigraphy; KGR, kinetic growth rate; MI, minimally invasive; OR, odds ratio; PPT, partial parenchymal transection; sTLV, standardized total liver volume.
Survival
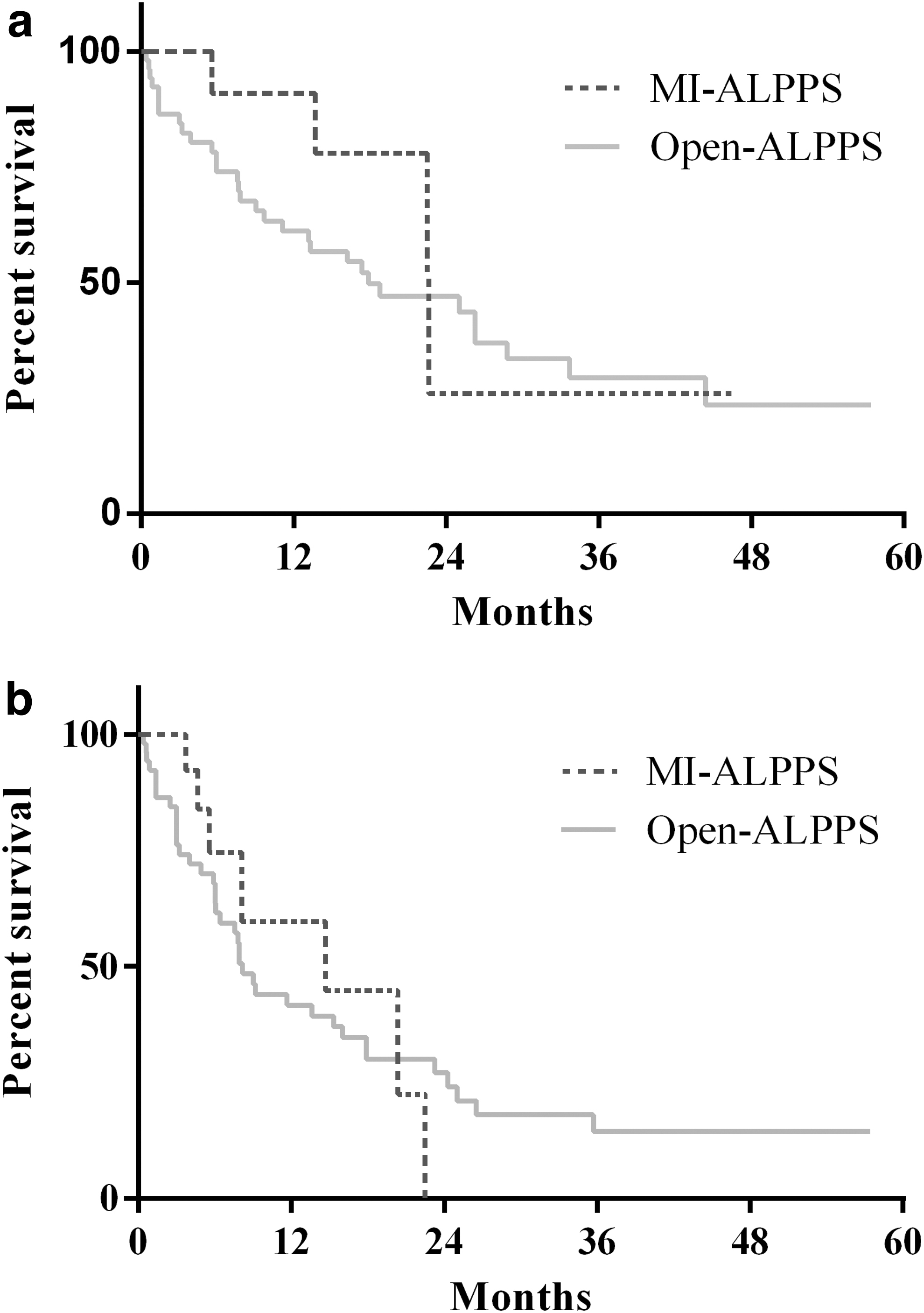
Median follow-up was 413 days (IQR = 148–686). Median OS did not significantly differ between MI-ALPPS and open-ALPPS (22.6 months versus 17.9 months, P = .278) (Fig. 1a). Thirty-one patients of 61 (46.7%) had recurrence of disease: liver-only (n = 10), extrahepatic (n = 10), and both intra- and extrahepatic (n = 11). Median DFS after MI-ALPPS was 14.7 months compared with that of open-ALPPS, which was 8.2 months (P = .714) (Fig. 1b).
Discussion
This study, developed from data collected by the Italian ALPPS registry, showed that a less invasive approach to ALPPS first stage was associated with a lower overall risk of PHLF. The lower impact of Stage 1 had a favorable impact on Stage 2 where a lower rate of complications (including ascites) and mortality was recorded in MI-group. Of interest, most patients with MI approach could be discharged home in the interstage, allowing full recovery before completion of surgery.
The need to specifically address the issue of comparison between MI and open-ALPPS in HCC arises from the observation of an increased susceptibility of patients with underlying liver disease to surgical stress.13,14 The topic becomes even more interesting in ALPPS because the impact of a two-stage surgery stratified per approach has never been analyzed before and the hypothesis of a different effect on outcome induced by different technical approaches deserves specific attention. After the first consensus meeting on ALPPS held in Hamburg in 2015 and published later in 2016, 25 several modifications of the ALPPS original technique have been introduced to reduce the high mortality/morbidity rates reported. Among them, the combination of PPT with PVE, also called mini-ALPPS, was proposed with the intent of minimizing the impact of the first stage, allowing fast and full recovery before the second stage.26,27 In addition, ALPPS first stage may be performed by laparoscopy 28 or robotically, 29 thus reducing adhesions in the second stage and conferring all the advantages of a previous MI surgery. Because PPT should not reach the anterior aspect of the inferior vena cava, such a procedure is burdened by a lower technical complexity and consequently associated with an increased feasibility using an MI approach. 30 In this setting, despite Stage 2 still representing the most aggressive procedure, it may benefit from a more favorable situation induced by the synergy of MI approach and PPT during Stage 1. This was consistent with our data reporting a significant number of patients with an MI approach discharged home in the interstage after a median of 5 days. After full recovery, Stage 2 was carried out in median 12 days later compared with open-ALPPS, but resectability was not affected and more importantly, morbidity and mortality rates were reduced regardless of how second stage was approached.
Because of longer interstage interval, a lower KGR was recorded in the MI group, taking also into account that PPT was performed in the majority of MI cases. Indeed, the caudal approach of laparoscopy can theoretically induce the surgeon to perform a transection deeper in the caudal and more superficial in the cranial segments, thus reducing the depth of the liver partition. Nevertheless, our study as well as systematic reviews and meta-analyses31,32 have shown that FLR increase is comparable between total and partial ALPPS and this has been explained by the inflammatory response associated with the hepatocyte damage owing to parenchymal transection that seems to lead to a similar regeneratory stimulus. 33
In the present series, PPT and MI first stage were both protective against the risk of developing PHLF after the second stage. The issue of hepatic decompensation in HCC patients and how MI techniques may reduce the risk of PHLF 34 especially in patients with cirrhosis and/or CSPH, is still open. 35 With regard to cirrhosis, F4 METAVIR score was found after surgery in a significantly higher percentage of patients submitted to open-ALPPS, suggesting that MI approach was less frequently considered in cirrhotic livers. However, cirrhosis was not significantly associated with PHLF at univariate analysis. Moreover, there were no significant differences in terms of preoperative (Stage 2) liver volumes between MI and open group when analyzing cirrhotic patients only. Thus, the most consistent hypothesis is that MI and open groups might have faced Stage 2 with a different functional reserve even when showing clinical and biochemical markers of liver function within limits of normality. Although liver function in HCC patients has been traditionally measured using biochemical scores,36,37 indocyanine green clearance test, 38 or liver stiffness, 39 more recently, HBS has been demonstrated to well predict PHLF before major hepatectomy 23 especially in ALPPS interstage. 40 Because drop of liver function may occur after ALPPS first stage as shown by HBS, 41 it is reasonable to think that both PPT and MI approach may have helped to preserve liver function in the interstage, despite recent controversial results found in more heterogeneous populations. 42 This was confirmed in our study where an increased number of PHLF Grade A was observed after open-ALPPS compared with MI approach. With regard to HBS, all the patients who were assessed with such a scintigraphic technique in the interstage did not develop PHLF. This could represent an important bias of this study but it confirms how functional assessment is of extreme importance in ALPPS especially in HCC patients and should therefore be standardly implemented. 25
Given the relatively limited number—within this series—of ALPPS totally performed by MI approach (1 and 2 stage), it is presently not possible to carry out a specific analysis comparing first stage only and full MI-ALPPS. However, it is possible to speculate that the advantages of a totally MI approach should be at least equal to those documented in comparative series of laparoscopic versus open major hepatectomies. 28
The main limitations of this study are its retrospective nature and the small sample numerosity that may have rendered the analysis particularly susceptible to bias or prevented significances in baseline characteristics between the two groups as well as significance at multivariate analysis. Second, the intrinsic nature of ALPPS Italian Registry—built to provide a reliable representation of the national picture, with no cutoff numerosity for joining, no superimposed techniques, and including high percentage of total centers performing ALPPS in the country—may have included varied characteristics and heterogeneities among centers (e.g., allocation criteria for MI approach, protocols of perioperative management, and use of Pringle maneuver) leading to disparities between MI- and open-ALPPS groups. In particular the policy of inclusion to MI technique may have been influenced by single institutions policy and expertise.
In conclusion, MI first stage of ALPPS together with PPT can be considered a safe option for candidates to ALPPS, because the favorable scenario provided by a less invasive Stage 1 allows to decrease not only morbidity and mortality rates but also incidence of PHLF especially in patients with limited hepatic functional reserve as HCC patients generally are. These findings were confirmed irrespectively from the approach chosen for Stage 2, for which MI feasibility still has to be analyzed in details. 43
Footnotes
Acknowledgments
The authors thank all the colleagues who participated in this study despite the difficulties encountered during COVID-19 outbreak.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no specific funding for this work.