
Abstract
Introduction:
Laparoscopic splenectomy (LS) has become the standard treatment for benign hematological disorders and hypersplenism. However, serious complications such as pancreatic fistula and portal venous thrombosis (PVT) sometimes occur. We investigated the clinical significance of splenic vessels and anatomical features in LS.
Methods:
Patient data were collected from 32 patients who underwent LS. The indications for LS were hypersplenism due to liver cirrhosis, idiopathic thrombocytopenic purpura, hereditary spherocytosis, and others. Close contact of pancreatic tail with splenic hilum, spleen volume, and diameters of splenic vessels were evaluated on computed tomography images.
Results:
Close contact of pancreatic tail with splenic hilum was recognized in 15 of the patients. The close contact was significantly associated with operation time (P = .038), spleen volume (P = .021), and spleen volume/body surface area (BSA) ratio (P = .001). In multivariate analysis, spleen volume/BSA ratio was an independent factor for close contact (P = .022). PVT occurred in 3 cirrhosis patients, and the diameter of the splenic vein (SV) was significantly associated with PVT as a result of multivariate analysis (P = .027).
Conclusion:
Close contact of the pancreatic tail with the splenic hilum may cause a longer operation time at LS and be associated with spleen volume/BSA ratio. A larger SV diameter in cirrhosis patients may be related to PVT after LS.
Introduction
Splenectomy has been performed to improve thrombocytopenia in cirrhotic patients before the induction of pegylated-interferon plus ribavirin therapy for hepatic C infection and in patients with cirrhosis undergoing treatment for hepatocellular carcinoma.1,2 In Japan, the first case of laparoscopic splenectomy (LS) was reported in 1992. 3 With advances in laparoscopic techniques, LS has become the standard treatment for benign hematological disorders and hypersplenism.4–6 However, severe complications such as pancreatic fistula and portal venous thrombosis (PVT) still occur in 4.5%–16% and 24%–53% of the cases, respectively, and pitfalls still exist.7–10 We empirically think that manipulation around the splenic hilum is more difficult in cases of close contact of the pancreatic tail with the splenic hilum, and early ligation of the splenic artery (SA) is easier in cases of tortuous SA. Spleen volume and portal hypertension have been reported to be associated with surgical outcomes of LS,9,11,12 and a relationship between PVT and splenic vein (SV) diameter has also been reported.9,10,13 However, there have been only a few reports on SA tortuosity 14 and no reports on close contact of the pancreatic tail with the splenic hilum.
In this study, we focused on the patients who underwent LS in our hospital. We investigated the clinical significance of the splenic vessels and anatomical features in LS.
Patients and Methods
Patients
In this retrospective study, patient data were collected from 32 patients who underwent LS at Oita University Faculty of Medicine between May 2003 and July 2017. Patient characteristics are presented in Table 1. The mean patient age was 42.0 ± 24.8 years, and the sex ratio (female:male) was 18:14. The body surface area (BSA) was calculated using the DuBois formula. 15 The indications for LS were hypersplenism due to liver cirrhosis (LC) in 11 patients, idiopathic thrombocytopenic purpura (ITP) in 10, hereditary spherocytosis (HS) in 7, and others in 4. Of the 32 patients, 10 (28%) were pediatric (<16 years old). The mean height of the pediatric patients was 131.0 ± 4.3 cm and body weight was 29.0 ± 5.4 kg. The pediatric indications for LS were ITP in 4 and HS in 5. This study was approved by the Ethics Committee of Oita University Faculty of Medicine (#1869).
Patient Characteristics
Surgical procedures
Surgical procedures of LS were followed as described previously. 16 Early ligation of the SA was performed at the pre-hilar SA before dissecting the spleen from the surrounding tissues to reduce blood loss, especially in patients with portal hypertension.17,18 After dissection of the ligaments, the splenic pedicle was divided with laparoscopic linear staplers (Endo-GIA™; Medtronic, Dublin, Ireland). The spleen was then placed into a large spectrum retrieval bag (Endo-Catch™, Medtronic) and crushed with the fingers and/or forceps before removal. For hand-assisted laparoscopic splenectomy (HALS), the incision was extended to the glove size, 7 cm. A GelPort® (Applied Medical; Rancho Santa Margarita, CA) was applied to the abdominal wall, and the surgeon's left hand was placed through it. 19 Patients with portal hypertension received heparin for 7 days postoperatively to prevent PVT. 20 PVT was diagnosed with postoperative follow-up computed tomography (CT).
Measurements of imaging parameters
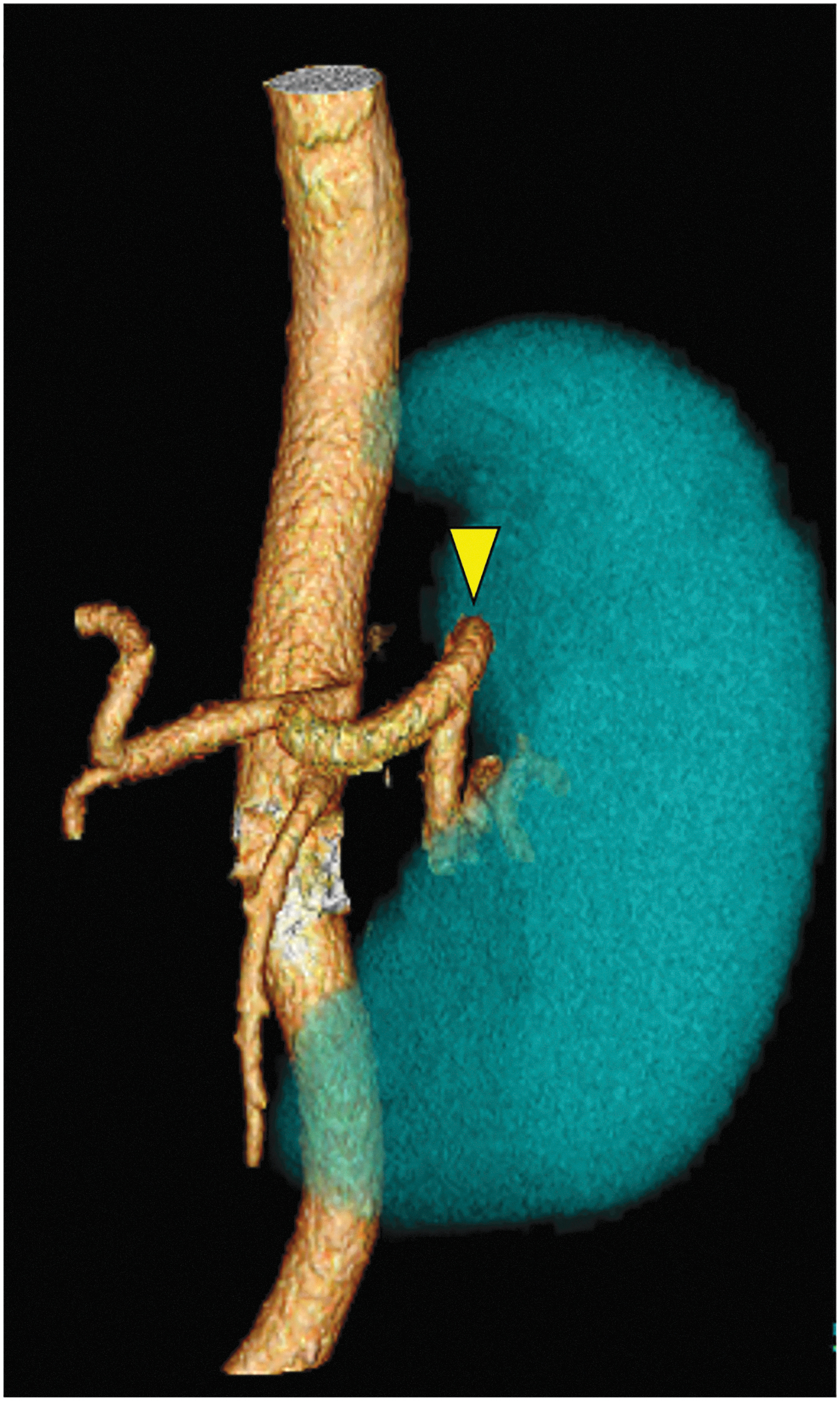
We used a 16-detector row CT scanner (Toshiba, Tokyo, Japan) with a slice thickness of 1.0–2.5 mm. Close contact of the pancreatic tail with the splenic hilum was defined as the pancreatic tail being close to and bending at the splenic hilum with more than 20 mm thickness (Fig. 1). A volume analyzer, Synapse Vincent version 4.4 (Fujifilm Medical Company, Tokyo, Japan) was used to measure spleen volume and length of the SA. This instrument allowed automatic rendering of high-precision, three-dimensional (3D) images from CT images (Fig. 2). The total length of the SA (x) and the straight distance of the SA (y) from the celiac trunk to the point of branching at the hilum were measured on the 3D images (Fig. 3), and the tortuosity index of the SA was calculated as x/y, as previously described. 14 The diameters of the splenic vessels were measured at three locations: central, intermediate, and peripheral, and the averages were used. 10 Evaluation of the CT images was performed by at least 2 physicians.

Typical feature of close contact of the pancreatic tail with the splenic hilum (arrow) on enhanced computed tomography.
Three-dimensional computed tomography image of the SA and spleen. The arrowhead indicates a tortuous SA at the suprapancreatic area. The tortuosity index of the SA was 3.2, and the spleen volume was 862 mL in this case. SA, splenic artery.
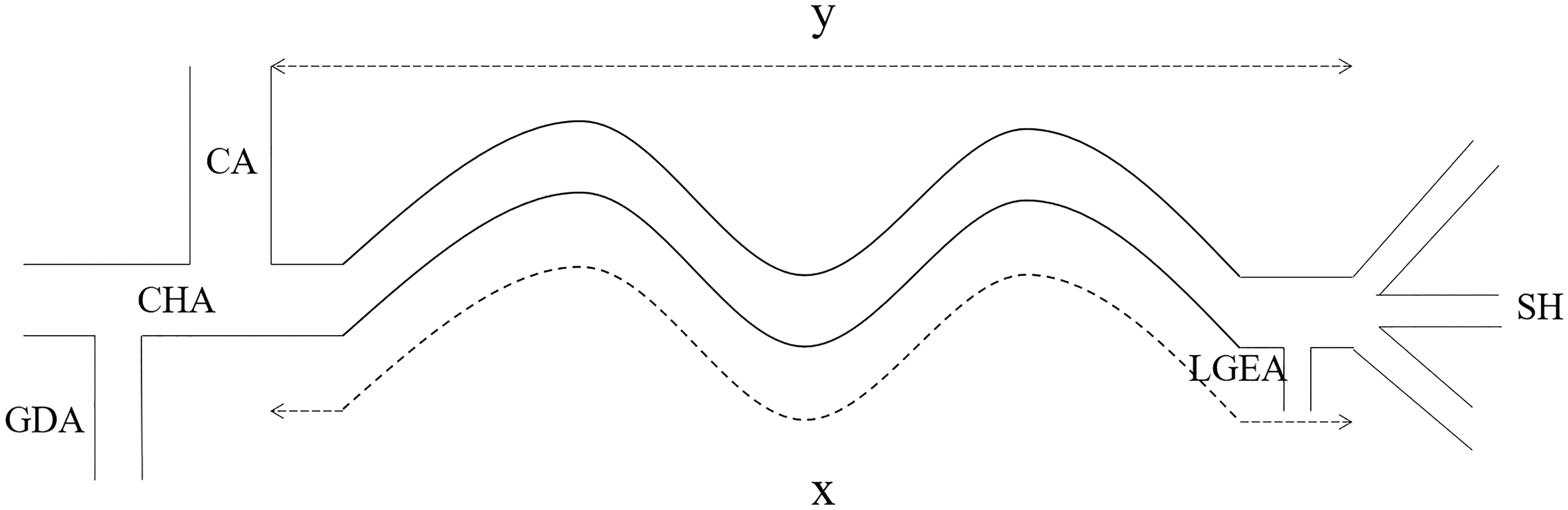
Tortuosity index of the splenic artery (x/y). CA, celiac trunk; CHA, common hepatic artery; GDA, gastroduodenal artery; LGEA, left gastroepiploic artery; SA, splenic artery; SH, splenic hilum; x, total length of the SA; y, straight distance of the SA.
Statistical analysis
Numerical data are expressed as mean ± standard deviation. Differences between the variables were compared using Fisher's exact or Mann–Whitney U test. The association between SA tortuosity and variables was evaluated using Spearman's rank correlation. Stepwise multiple regression analyses were performed to investigate independent factors for close contact of the pancreatic tail with the splenic hilum, tortuosity of the SA, and postoperative PVT among significant patient characteristics and imaging parameters in the univariate analyses (P < .05). The relationship between tortuosity of the SA and early ligation and that between PVT and SV diameter were analyzed using receiver operating characteristic (ROC) curves and the area under the ROC curve (AUC). The cutoff value was decided using Youden's index. A P value <.05 was considered to be statistically significant. All statistical analyses were performed with JMP software version 14.2 for Windows (SAS Institute, Cary, NC).
Results
Surgical outcomes
There were no open conversions, but 4 patients underwent HALS due to severe adhesions (Table 2). Early ligation of the SA was performed in 16 of the patients (50%), whose diseases were LC in 11 patients, HS in 3, ITP in 1, and others in 1. The mean operation time was 180.6 ± 85.0 minutes, and mean blood loss was 126.3 ± 234.0 mL. Postoperative complications occurred in 6 patients (19%): PVT in 3 patients, pancreatic fistula in 1, sepsis in 1, and intra-abdominal bleeding in 1.
Surgical Outcomes
The 16 patients who underwent early ligation had a mean operation time of 189.1 ± 21.5 minutes and blood loss of 51.4 ± 60.6 mL, whereas those who did not have a mean operation time of 172.1 ± 21.5 minutes and blood loss of 191.9 ± 56.7 mL. The differences were not significant (P = .580, .102, respectively).
Measurements of splenic vessels and anatomical features
Fifteen of the patients (47%) had findings of close contact of the pancreatic tail with the splenic hilum (Table 3). The mean spleen volume was 456.9 ± 393.3 mL, and the spleen volume/BSA ratio was 311.0 ± 227.1 mL/m2, respectively. The mean total length of the SA (x) was 116.5 ± 6.4 mm, and the straight distance of the SA (y) was 60.2 ± 15.8 mm. The mean tortuosity index of the SA (x/y) was 2.0 ± 0.6. The mean diameters of the SA and SV were 5.3 ± 1.7 mm and 8.6 ± 2.7 mm, respectively.
Measurements of Splenic Vessels and Anatomical Features
Relationship between close contact of the pancreatic tail with the splenic hilum and patient data
In univariate analyses, close contact of the pancreatic tail with the splenic hilum was significantly associated with spleen volume and spleen volume/BSA ratio (P = .021, .001, respectively, Table 4). Operation time was significant longer in the close contact group than that in the nonclose contact group, but there was no significant difference in blood loss between the two groups. In addition, pancreatic fistula occurred postoperatively in 1 patient in the close contact group. Multivariate analysis showed that spleen volume/BSA ratio was an independent factor for close contact of the pancreatic tail with the splenic hilum among the patient characteristics and imaging parameters (P = .022).
Relationship Between Close Contact of Pancreatic Tail with Splenic Hilum and Patient Data
BSA, body surface area; CI, confidence interval; HALS, hand-assisted laparoscopic splenectomy.
Relationship between tortuosity of the SA and patient data
In univariate analyses, age, body mass index, disease, spleen volume, spleen volume/BSA ratio, diameter of the SA, and diameter of the SV were significant factors for tortuosity of the SA (Table 5). In multivariate analysis, diameter of the SA was an independent factor for tortuosity of the SA (P = .013).
Relationship Tortuosity of Splenic Artery and Patient Data
BSA, body surface area; CI, confidence interval.
The mean tortuosity index of the SA was significantly higher in the 16 patients with early ligation of the SA than that in the 16 patients without early ligation (2.2 ± 0.1 versus 1.7 ± 0.1, P = .017). The ROC curve for early ligation showed that the AUC was 0.750 (P = .012), and the cutoff value for tortuosity index of the SA was 1.9.
Relationship between PVT and patient data
Postoperative PVT was observed in 3 patients, all of whom had LC (Table 6). Univariate analyses showed that postoperative PVT was significantly associated with disease, spleen volume, spleen volume/BSA ratio, diameter of the SA and SV, HALS, and blood loss. Multivariate analysis found diameter of the SV to be the only parameter significantly associated with PVT among the patient characteristics and imaging parameters. The mean diameter of the SV in the 3 patients with postoperative PVT was 13.1 ± 1.4 mm. The ROC curve for PVT showed an AUC of 0.931 (P = .045), and the cutoff value for SV diameter was 10.5 mm.
Relationship Between Portal Venous Thrombosis and Patient Data
BSA, body surface area; CI, confidence interval; HALS, hand-assisted laparoscopic splenectomy.
Discussion
Recently, LS has become the standard for the treatment of benign hematological disorders and hypersplenism.4–6 However, a survey by the Japan Society for Endoscopic Surgery (JSES) reported a 7.7% incidence of postoperative complications 21 that included serious complications such as pancreatic fistula and PVT. Therefore, we investigated the relationship between the complications and splenic anatomical features in LS. Some new findings were revealed in this study. Close contact of the pancreatic tail with the splenic hilum may cause a longer operation time and be associated with the spleen volume/BSA ratio. Further, SA tortuosity may be associated with SA diameter, and a larger SV diameter in cirrhosis patients may be related to postoperative PVT.
To date, the clinical impact of close contact of the pancreatic tail with the splenic hilum on surgical outcomes has been unclear. The positional relationship between the pancreatic tail and the splenic hilum is very important during dissection of the splenic hilum. The pancreatic tail is reported to be almost always located at the splenic hilum or caudal to it, 22 but there have been no reports about close contact of the pancreatic tail with the splenic hilum. In patients with close contact of the pancreatic tail, manipulation at the splenic hilum is thought to be more difficult because of the increased frequency of pancreatic tail injury. Once the pancreas is injured by manipulation at the splenic hilum, one of the fatal complications, pancreatic fistula, will occur. Postoperative pancreatic fistula in LS has been reported to be related to the length of the spleen and splenic volume.7–9,11 In this study, operation time was significantly longer in the close contact group. Pancreatic fistula occurred only in 1 patient in the close contact group, indicating that close contact of the pancreatic tail with the splenic hilum may be associated with the development of postoperative pancreatic fistula in LS. In addition, the spleen volume/BSA ratio was an independent factor for close contact of the pancreatic tail with the splenic hilum. LS is usually applied both to children and to adults, and the intra-abdominal cavities of the patients vary. Because BSA is an objective index of physique, the spleen volume/BSA ratio may indicate the ratio of space occupied by the spleen in the intra-abdominal cavity. Therefore, the spleen volume/BSA ratio was significantly associated with close contact of the pancreatic tail but spleen volume was not in this study.
Postoperative PVT still frequently occurs after LS.9,10,13 It can lead to liver failure and worsen portal hypertension, and thus its prevention and prediction are important. A relationship between PVT and SV diameter has been reported. Kinjo et al. reported that an SV diameter of ≥9 or ≥13 mm was associated with PVT in LC patients after LS. 10 Danno et al. also reported that an SV diameter of ≥8 mm was associated with PVT in patients without LC. 13 Kuroki et al. indicated that 10 mm was an accurate cutoff value of SV diameter for the prediction of PVT after LS. 23 In the present study, PVT occurred in 3 patients with LC (9%), and the cutoff value of SV was 10.5 mm. Therefore, in patients with an SV diameter ≥10 mm, careful postoperative management for PVT is thought to be very important.
When the SA is severely tortuous in the suprapancreatic area, it may be easier to perform early ligation of the SA. A case-control study reported that early ligation of the SA decreased intraoperative bleeding in LS, 18 but there has been no strong evidence for this technique to reduce the blood loss until now. In a previous report, tortuosity of the SA was attributed to congenital, age-dependent and pathological changes and not to atherosclerosis. 24 The present study showed that the diameter of the SA was only significantly associated with tortuosity of the SA. This result suggested that tortuosity was attributable to pathological change due to enlargement of the SA. It was reported that SA diameter and SA flow volume are closely correlated. 25 Therefore, tortuosity of the SA may be a consequence of splenic hyperkinetic state.
There were some limitations in this study. First, this study was retrospective with a small number of patients. A larger prospective series of patients undergoing LS will be needed to confirm our results. Second, the patients in this study included both adults and children without distinguishing between them. Third, due to the long duration of the study, some of the LS surgical techniques had slightly changed over time.
Conclusion
Close contact of the pancreatic tail with the splenic hilum may cause a longer operation time and be associated with the spleen volume/BSA ratio. A larger SV diameter in cirrhosis patients may be related to postoperative PVT. In addition, SA tortuosity may be related to the diameter of the SA and splenic hyperkinetic state.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.