
Abstract
Background:
This study aimed to report a European multi-institutional experience about thoracoscopic management of children with congenital lung malformations.
Methods:
The records of 102 patients (49 girls and 53 boys) with median age at surgery of 1 year (range 6 months–1.5 years), who underwent thoracoscopic lobectomy in five European Pediatric Surgery units, were retrospectively collected. Indications for surgery included congenital pulmonary airway malformation (CPAM) (n = 47), intra- and extralobar pulmonary sequestration (n = 34), hybrid lesion (CPAM/intralobar sequestration) (n = 2), severe bronchiectasis (n = 9), congenital lobar emphysema (n = 8), and others (n = 2). The condition was asymptomatic in 77/102 (75.5%), whereas symptoms such as recurrent pneumonia and/or respiratory distress were present in 25/102 (24.5%).
Results:
Surgical procedures included 18 upper, 20 middle, and 64 lower lobe resections. No conversions to open were reported. A 3 mm sealing device and 5 mm stapler were adopted in the last 48/102 patients (47%). The median operative time was 92.2 minutes (range 74–141). The median operative time significantly decreased in patients in whom the vessel division and bronchial sealing were performed using sealing devices (75.5 minutes) compared with suture ligations (118.9 minutes) (P = .001). The median hospital stay was 3.7 days (range 2–6.2). Three/102 patients (2.9%) developed postoperative complications, including air leakage requiring pleural drainage (n = 1) (Clavien IIIb) and respiratory infection (n = 2) (Clavien II). A reoperation was required in one patient with residual pleuropulmonary blastoma (0.9%). All symptomatic patients reported resolution of symptoms postoperatively.
Conclusions:
Thoracoscopic lobectomy is a safe and effective procedure with excellent cosmetic outcome, in expert hands. Based upon our experience, we strongly recommend surgery in patients with congenital lung malformations by the first year of life, to reduce the risk of infection and make the procedure technically easier, despite the small patients' size. Surgeon's experience and use of miniaturized instruments and sealing devices remain key factors for successful outcome.
Introduction
Congenital lung malformations, mainly represented by congenital pulmonary airway malformation (CPAM) and pulmonary sequestration, are the most common prenatally diagnosed intrathoracic masses. 1 Clinically, these lesions may cause acute respiratory distress in the neonatal period, may cause infections throughout childhood, or can remain asymptomatic and undiagnosed until later in life.2,3 The current management of these malformations and the optimal timing of surgery remain controversial, especially in the absence of clinical symptoms. 4 The decision to operate an asymptomatic patient is based on a combination of factors, such as the size of the lesion, the parental concern, the safety of anesthesia, and the surgeon's personal preference. 5 However, most authors agree that complete surgical resection remains the standard treatment, at least for CPAM and intralobar sequestration. 6 In these malformations, despite the lack of symptoms, patients are predisposed to recurrent pulmonary infections and, if untreated, these lesions may undergo malignant transformation.7–9 Research on the follow-up of asymptomatic neonates with cystic lung disease has found that 74.3% become symptomatic by the age of 3 years. 10 For these reasons, cystic lung lesions should be resected electively as it may become problematic in patients with a history of pulmonary infections. 7
In patients who need surgical intervention, anatomic lobectomy is recommended over segmental resection.3,4 Albanese et al. first described a completely thoracoscopic minimally invasive lobectomy in 2003. 11 Subsequent case series have shown that thoracoscopic lobectomy is a feasible and safe technique, also in small infants, demonstrating improved or equivalent complication rates, decreased postoperative pain, shorter hospital stay, better cosmetic outcome, and decreased time of tube thoracostomy when compared with open techniques.12–17 Additionally, long-term morbidity due to a major thoracotomy incision is avoided. 11 However, the current evidence about this technique is still very limited in pediatric literature and is currently being performed in centers with high-volume minimally invasive surgery (MIS) activity and by expert surgeons skilled in thoracoscopic surgery.
The aim of this study was to report a European multi-institutional experience about thoracoscopic management of children with congenital lung malformations.
Materials and Methods
The medical records of 102 patients (49 girls and 53 boys) with median age at surgery of 1 year (range 6 months–1.5 years) and median weight of 9.8 kg (range 8–11.2), who underwent thoracoscopic lobectomy in five European Pediatric Surgery units over a 5-year period (June 2014–June 2019), were retrospectively collected and analyzed. Exclusion criteria were all patients, who were operated on with an open technique in neonatal age.
Indications for surgery included CPAM (n = 47), intra- and extralobar pulmonary sequestration (n = 34), hybrid lesion (CPAM/intralobar sequestration) (n = 2), severe bronchiectasis (n = 9), congenital lobar emphysema (n = 8), and others (malignancy and neuroglial heterotopia) (n = 2). Prenatal diagnosis was obtained in 79/102 patients (77.4%). The condition was asymptomatic in 77/102 (75.5%), whereas symptoms such as recurrent pneumonia and/or respiratory distress were present in 25/102 (24.5%). Pathology was right sided in 59/102 (57.8%) and left sided in 43/102 (42.2%).
Preoperative work-up included ultrasound, chest X-ray, computed tomography (CT), and/or magnetic resonance imaging (MRI) in all patients (Fig. 1). Follow-up included clinical controls every 3 months for the first year after surgery, thereafter every 6 months for the second year, and thereafter annually. A control chest X-ray was repeated at 1 month and 1 year postoperatively.
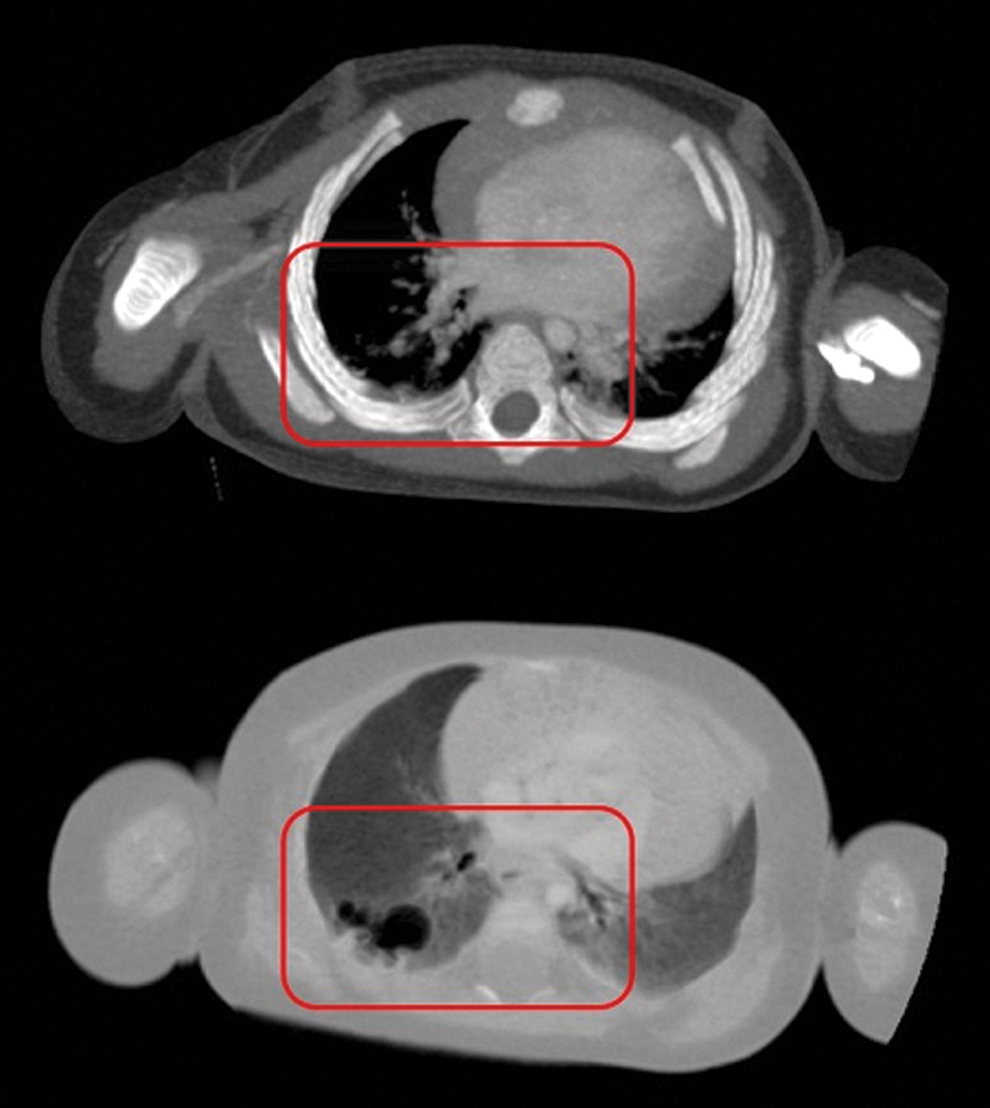
A CT scan demonstrating a CPAM in the right lower lobe. CPAM, congenital pulmonary airway malformation; CT, computed tomography.
All patients' demographics are reported in Table 1.
Patients' Demographics in Our Series
CPAM, congenital pulmonary airway malformation; CT, computed tomography; MRI, magnetic resonance imaging; US, ultrasound.
Primary outcome parameters included surgical success rate, defined as complete removal of the malformation and resolution of clinical symptoms in symptomatic patients. Secondary outcome parameters included length of surgery, intraoperative complications, conversions, postoperative complications, and reoperations. Postoperative complications were classified according to the Clavien–Dindo grading system. 18
The study received the appropriate Institute Review Board approval at each participating center.
Operative technique
The patients were placed in a lateral decubitus position with the operative side turned up and the surgeon and assistant stood at the child's anterior chest wall facing a single monitor placed in front of the operating surgeon. Three ports were adopted: the first 5-mm trocar was inserted, with an open technique, in the mid axillary line through the fifth or sixth intercostal space, and was adopted as camera port for the 5-mm, 30° telescope. A selective single lung ventilation was achieved in only 20 patients by means of contralateral mainstem bronchus intubation. All other procedures were performed using tracheal ventilation. The pneumothorax was induced with a CO2 flow of 1 L/min and a pressure between 4 and 8 mmHg. Two additional working ports were placed in the anterior axillary line above and below the camera port: one 5-mm port was dedicated to the 5-mm Ligasure (Valleylab, Boulder, CO) and/or the 5-mm stapler (JustRight Surgical, Boulder, CO), and one of 3-mm was dedicated to the 3-mm laparoscopic instruments and/or the 3-mm JustRight Vessel Sealing System (JustRight Surgical). The location of the fissure should indicate the placement of the other ports. The surgical technique varied depending on the affected lobe and type of malformation. In CPAM patients, the lobar vessels were dissected and sealed using the 3-mm JustRight Vessel Sealing System or the 5-mm Ligasure. Occasionally, endoscopic clips and suture ligations were also used. In cases with incomplete fissure, dissection was performed along this plane and then the fissure was completed using the 5-mm stapler or the 5-mm Ligasure before dissecting the pulmonary arterial supply. The bronchus to the affected lobe was dissected and closed intracorporeally using the 5-mm stapler or alternatively suture ligations or 5-mm endoscopic clips. In larger patients, a 12-mm endoscopic stapler was adopted to seal the bronchus; in this last case, a 12-mm trocar was placed instead of the 5-mm trocar.
In lower lobectomies, the lobar dissection began with mobilization of the inferior pulmonary ligament and division of any pleuropulmonary adhesions (Fig. 2). During this maneuver, care was taken to identify a potential systemic vessel arising from the aorta in cases of bronchopulmonary sequestration. In such case, the systemic vascular supply was identified, ligated with the Ligasure or endoscopic clips, and divided. Once the lung was free, attention was turned to the hilum. The branches of pulmonary artery to the affected lobe were sealed and divided first, then the pulmonary vein, and lastly the bronchus (Fig. 3). Middle lobectomies proceeded first with completion of the fissures to allow identification of the branches of both the pulmonary vein and artery, followed by isolation and division of segmental branches. For upper lobe resections, dissection started with isolation and division of the superior pulmonary artery at the segmental level. Once the lobectomy was completed, the specimen was then brought out through a slightly enlarged trocar site, either whole or piecemeal (Fig. 4). A chest tube was left in place through a trocar site in all cases and port incisions were finally closed using absorbable suture.
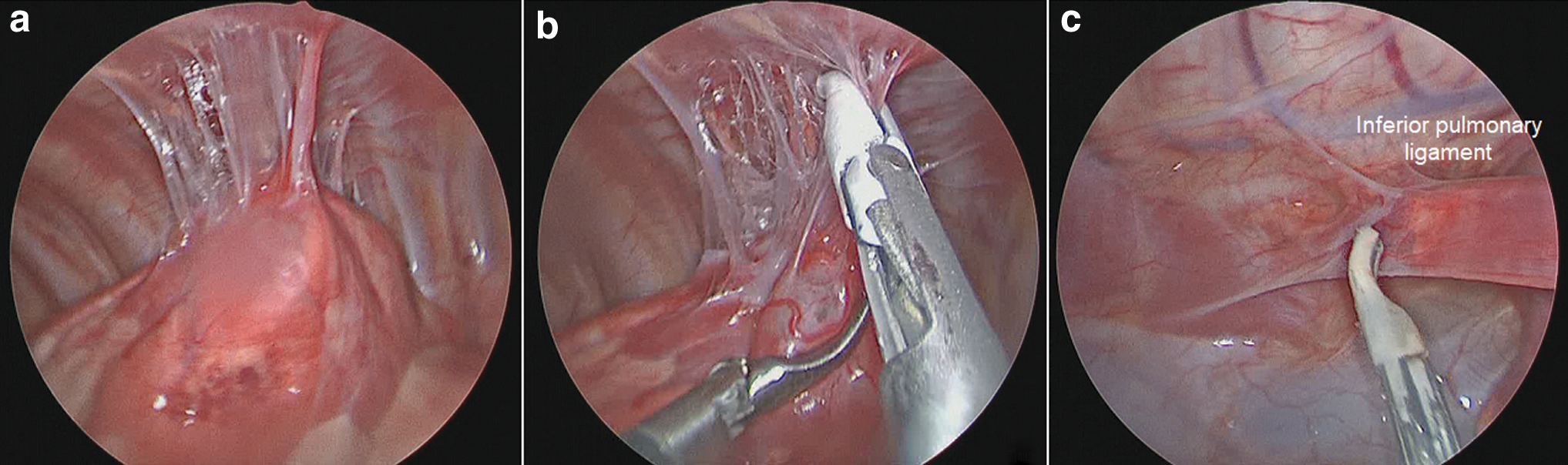
Right lower lobectomy technique—division of pleuropulmonary adhesions
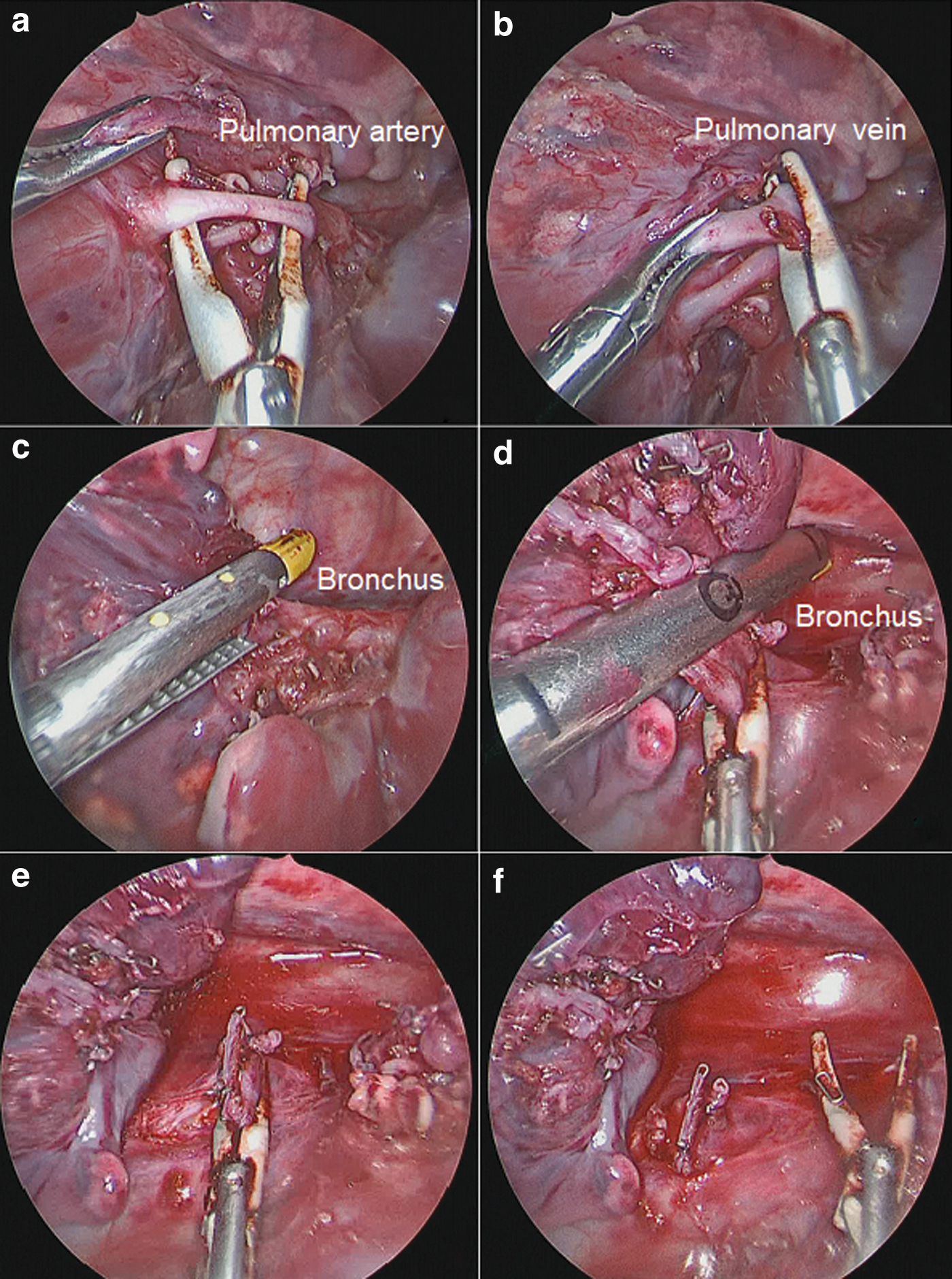
Right lower lobectomy technique—sealing and division of the branches of pulmonary artery and pulmonary vein using the 3-mm vessel sealing device
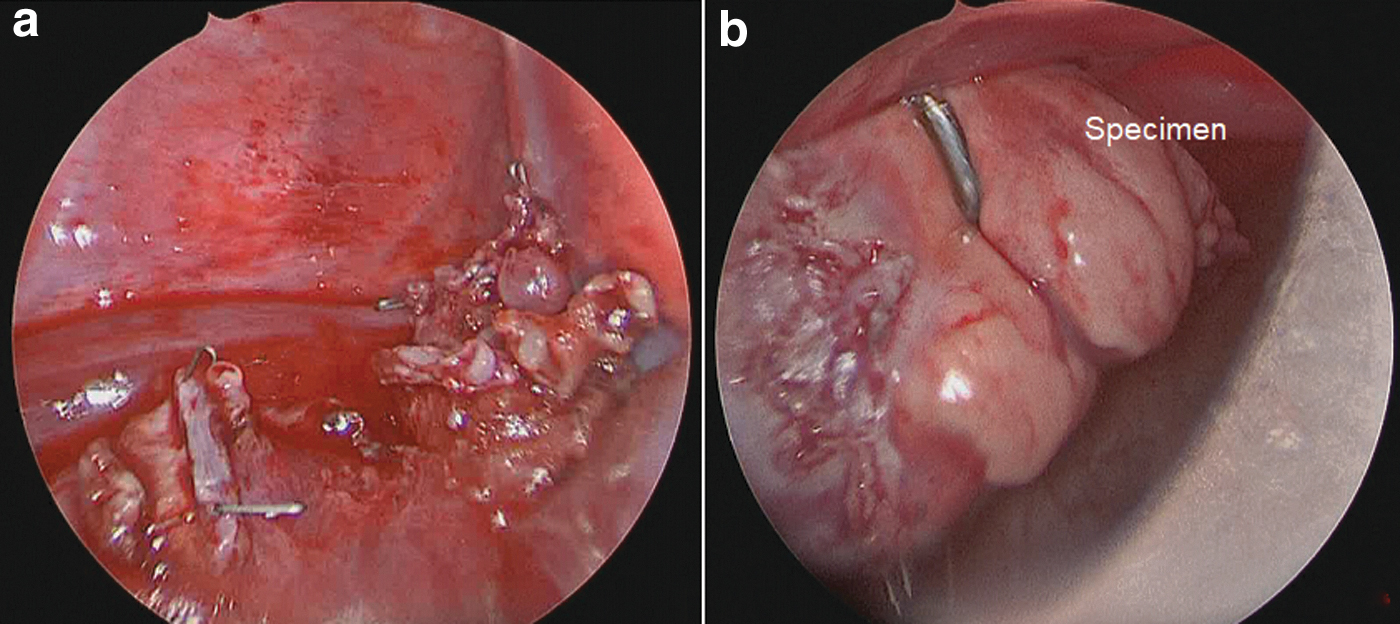
Right lower lobectomy technique—final check after completion of lobectomy
Results
All procedures were completed thoracoscopically using three ports (3-mm and 5-mm) and included 18 upper lobe resections, 20 middle lobe resections, and 64 lower lobe resections. Most cases (71/102, 69.6%) were performed in two centers; however, no difference regarding time of surgery, complications, or length of hospital stay were found between all centers. No conversions to open surgery were reported in all centers. These findings were most probably related to the fact that all surgical procedures were performed by a senior surgeon skilled in thoracoscopy in each participating center. Each senior surgeon had >15 years of experience in MIS with a median number of 450 MIS procedures per year. Additionally, most surgeons safely performed the first procedures under the guidance of an experienced surgeon, thus allowing to shorten the learning curve and to reduce the complications.
An incomplete fissure was found intraoperatively in 35/102 cases (34.3%). No intraoperative complications occurred. The decision as to whether single lung or tracheal ventilation was used was mainly depending upon the anesthesiologist's experience and confidence with each technique. A selective single lung ventilation was adopted in only 20/102 patients (19.6%) from a single center. This variable did not affect in any way the operative time and complication rate within the single center and reported no difference between all surgical units.
Pulmonary vessels sealing, lung parenchyma division, and bronchial sealing were performed using the 3-mm JustRight Vessel Sealing System and the 5-mm JustRight stapler in the last 48/102 patients (47%), who were operated since 2018.
The median operative time was 92.2 minutes (range 74–141). The median operative time significantly decreased in patients in whom the vessel division and bronchial sealing were performed using sealing devices (75.5 minutes) compared with suture ligations (118.9 minutes) (P = .001). The median analgesic requirement (paracetamol 15 mg/kg every 8 hours) was 20.4 hours (range 9–28). The median chest tube duration was 1.3 days (range 1–4). The median hospital stay was 3.7 days (range 2–6.2).
The median follow-up length was 21.6 months (range 9–24). The overall success rate was 99.1%. One patient (0.9%) with pleuropulmonary residual blastoma required a reoperation to perform complementary resection. The postoperative complications rate was 2.9% and included air leakage requiring pleural drainage (n = 1) (Clavien IIIb) and respiratory infection (n = 2) (Clavien II).
After surgery, all symptomatic patients reported complete resolution of symptoms. Control chest X-rays were normal at 1 month and 1 year postoperatively in all patients (Fig. 5). The cosmetic outcome was excellent in all patients (Fig. 6).
Postoperative chest X-ray at 1 year following a left lower lobectomy.

Cosmetic outcome at 6 months postoperatively
Pathologic examination confirmed evidence of CPAM, pulmonary sequestration, congenital lobar emphysema, or “hybrid” lesion.
All outcome parameters are reported in Table 2.
Outcome Parameters in Our Series
Discussion
Elective thoracoscopic lobectomy has been reported as a safe, effective, and well-established approach for surgical treatment of pediatric patients with congenital lung malformations. Several advantages of this technique have been clearly demonstrated.2,12 First, it avoids complications and morbidity associated with standard posterolateral thoracotomy. 11 In fact, the small incisions performed in the thoracoscopic approach allow to avoid the risk of musculoskeletal deformities, including asymmetric chest wall, scoliosis, and winged scapula that have been reported following posterolateral thoracotomy.12,19 Additionally, it has all advantages of MIS, including excellent cosmetic outcome, decreased postoperative pain, short hospitalization, and rapid return to full daily activities. 12
Despite this general consensus, the diffusion of this technique and surgeons' comfort with this approach remain relatively low. 13 It is currently being performed in centers with high-volume MIS activity and by expert surgeons skilled in thoracoscopic surgery. The ability to first correctly identify vital structures supplying both affected lobe and areas to be preserved and then safely secure the large pulmonary vessels and lack of an adequate lung case volume make this operation one of the most technically demanding procedures for pediatric surgeons. 13 For this reason, the current evidence about the long-term outcome of this technique is still very limited in the pediatric literature.13,20,21 So, we decided to organize a multicenter study to collect the experience of the main European centers with strong experience in this procedure and our study is one of the largest case series among those published until now. Based upon this multicenter experience, we would like to underline some key points in the management of these patients.
First, it is fundamental to obtain an accurate preoperative imaging study of these lesions. CT should represent the first-line postnatal investigation for all babies with prenatal diagnosis of suspected CPAM. 22 The main difficulty lies in identifying any aberrant vessels supplying the lesion. To date, the accuracy of MRI in showing the latter is not established. 23 So, we always preferred to perform CT to confirm the diagnosis of CPAM or detect aberrant vessels and confirm the presence of a pulmonary sequestration or, in rare cases, demonstrate the association of a macrocystic lesion with an aberrant vessel (hybrid lesion) (Fig. 7). Our common protocol is to follow a period of observation in the asymptomatic prenatally diagnosed cases, and then to repeat a thorax CT scan at 3–6 months of age and, if malformation is confirmed, to plan the surgery by the first year of age or before if symptoms appear.
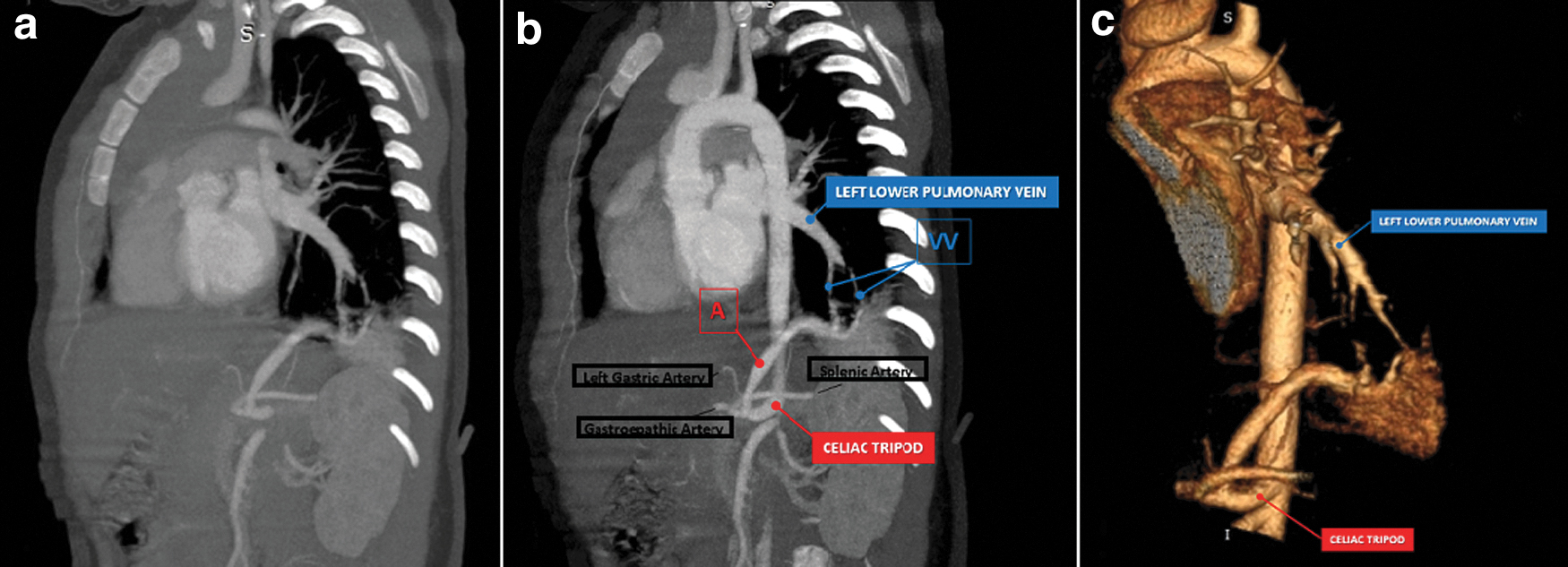
A CT scan demonstrating an hybrid lesion (CPAM + intra-lobar sequestration) in the left lower lobe
The second point of debate is the optimal timing of surgery; we agree with most authors that elective surgery should be accomplished by the first year of age of the child.11,12,17 In this way, we can perform an elective surgery, avoid the long-term risks (infection, pneumothorax, and malignant transformation) associated with untreated malformations and promote compensatory growth of the remaining parenchyma. In fact, it has been demonstrated that pulmonary parenchymal growth is particularly important during the first 3 years of life. 22 In addition, early intervention in patients with no episodes of pulmonary infection is easier and safer with lower complication and conversion rates compared with patients who have already suffered a clinical chest infection. 13 Additionally, as reported by Rothenberg et al., many of the patients, who were clinically asymptomatic, had likely subclinical infections before surgery. 12 He found in the older patients, who were apparently asymptomatic, varying degrees of inflammation, including enlarged, adherent lymph nodes adjacent to the vessels, adhesions, and even completely fused fissures that made surgery more difficult and dangerous. 12 For all these reasons, it is preferable to remove these lesions as earlier as possible and before they become symptomatic to avoid a more complicated surgery.
Third, this multi-institutional study confirmed that surgeon's experience remains the main prerequisite to safely accomplish this procedure and ensure the best possible outcome for the patient. In all cases, the surgeon should be familiar with the anatomy of the pulmonary arteries, veins, and bronchi, including the various aberrant arteries/veins known to exist in each lobe, and also have confidence in treating incomplete fissures between lobes. Another important suggestion is to perform the first procedures under the guidance of an expert tutor, who is able to interpret difficult or unusual anatomy improving the learning curve. In our series, most cases (71/102, 69.6%) were performed in two centers; however, no difference regarding time of surgery, complications, and length of hospital stay was found between all centers. No conversions to open surgery were reported in all centers. These findings were most probably related to the fact that all surgical procedures were performed by a senior surgeon skilled in thoracoscopy in each participating center. Additionally, most surgeons safely performed the first procedures under the guidance of an experienced surgeon, thus allowing to shorten the learning curve and to reduce the complications.
The fourth and last key point is the use of recently introduced miniaturized instruments, represented by the 3-mm vessel sealing device and the 5-mm stapler (JustRight Surgical).24–26 The 3-mm sealing device now available can seal vessels up to 5-mm in diameter and its curved Maryland-style jaw design allows it to work well as a dissector, especially in the small chest cavity of infants. Its use is adapt for most pulmonary vessels in children under 10 kg and for segmental branches in larger children. As described by Rothenberg, the key to using vessel-sealing technology effectively is to make proximal and distal seals on the vessel ∼3–5 mm apart. 24 Using scissors, a partial cut is made to determine that the seals are secure and that there is no bleeding once the lumen is entered. Once the vessel is partially divided and no bleeding is seen, the vessel can be completely divided. 23 One of the most difficult aspects of these procedures is when the fissure is incomplete and the pulmonary vessels are not readily visible.5,27 We found that the 3-mm sealing device was very useful to dissect and divide the parenchyma of an incomplete fissure, limiting bleeding and air leak. The fissure was approached layer by layer until the pulmonary artery was visualized.
For bronchus management, you can adopt 5-mm endoscopic clips in smaller children or 12-mm endostapler in larger patients. The new 5-mm stapler, with a staple line length of 25 mm and a staple leg length of 2 mm, allowed to eliminate the use of clips and larger staplers in the small patients. 24 Moreover, the reduced dimensions of these instruments occupy less space, allowing for better visualization of the surgical field. 26
The usefulness to adopt the new sealing and stapling technologies in such procedures was confirmed by our results; in fact, the median operative time significantly decreased in patients in whom the vessel division and bronchial sealing were performed using sealing devices (75.5 minutes) compared with suture ligations (118.9 minutes) (P = .001).
Our results confirmed that thoracoscopic lobectomy is a safe and effective procedure with excellent cosmetic outcome if performed by expert hands. Considering the technical challenges of this procedure related to anatomical anomalies such as incomplete fissure and low number case, we believe that these patients should be treated in referral centers in each country to reduce the incidence of complications. The use of miniaturized instruments such as the 3-mm vessel-sealing device and the 5-mm stapler allowed to perform a quicker and a safer procedure. Based upon our experience, we strongly recommend surgery in patients with congenital lung malformations by the first year of life, to reduce the risk of infection and make the procedure technically easier, despite the small patients' size. Surgeon's experience and use of miniaturized instruments and sealing devices remain key factors for successful outcome.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No fundings was received for this study.