
Abstract
Purpose:
To review the treatment of lower congenital esophageal stenosis caused by tracheobronchial remnants (TBR) and to introduce a novel technical approach through laparoscopic surgery.
Methods:
Patients with TBR who underwent surgery in our single-center from January 2016 to December 2019 were enrolled. Resection of cartilage with stenotic esophageal segment and end-to-end anastomosis was the traditional surgery. Since 2018, longitudinal incision with partial resection of cartilage loop in the anterior esophageal wall and the transverse suture was conducted endoscopically. We reviewed the treatment, followed-up with these patients, and discussed the new procedure's preponderance.
Main Results:
Thirteen patients underwent surgery and were followed-up for 0.5–45 months (M = 13) after surgery. Twelve patients showed good physical development with a regular diet. One patient, who was 2 weeks after the surgery, was fed by a soft diet and regularly followed-up at our clinic. In 13 cases, five patients underwent traditional laparotomy with pyloroplasty. Two patients who went through anastomotic leakage were cured by drainage and conservative treatments. Anastomotic stricture that occurred in two cases was improved by one-time of dilation. The administration time of parenteral nutrition (PN) was 9.0 ± 1.4 days. The length of hospitalization was 36.6 ± 5.2 days. Eight cases underwent the new surgical approach through laparoscopy or thoracoscopy. Pyloroplasty was avoided since the vagal close to the posterior wall of the esophagus was protected. Gastric motility disorder did not occur as expected. No leakage occurred postoperatively. The anastomotic stricture was found in six cases and improved after one to five times of dilations. The length of hospitalization dropped to 18.6 ± 6.9 days significantly (P < .001).
Conclusions:
Longitudinal incision and transverse anastomosis of the anterior wall of the esophagus with partial resection of cartilage without pyloroplasty through endoscopy is a novel practical surgical approach to treat patients with TBR.
Introduction
Congenital esophageal stenosis (CES), caused by tracheobronchial remnants (TBR), fibromuscular thickening or fibromuscular stenosis, and a membranous web or diaphragm, is a rare malformation with an incidence less than 1/25,000.1,2 The common manifestations in children with CES include vomiting, dysphagia, eating disorder, and growth retardation. For those caused by TBR, the stenosis can hardly be solved by bougienage and balloon dilation like the other two types,3,4 resection of the stricture segment and end-to-end anastomosis, which are commonly used.4–7 With the potential risk of injury of the vagal nerve close to the posterior wall of the esophagus, laparotomy is widely used since pyloroplasty can be conducted meanwhile. With the advanced technology of endoscopy, our department ameliorated the traditional laparotomy procedure to longitudinal incision with partial resection of cartilage in the anterior wall of the esophagus and transverse suture through laparoscopy or thoracoscopy since 2018. We reviewed the treatment of patients with TBR and compared the outcomes and complications of two methods. The purpose of this study was to introduce the effectiveness and preponderance of the novel technical approach.
Materials and Methods
From January 2016 to December 2019, 13 patients were diagnosed with CES according to symptoms and esophagography in our center. During the treatment, balloon dilation was first tried to exclude stenosis caused by fibromuscular thickening or membranous web. In all these patients, the balloon cannot be expanded at the stricture segment. Then, they were diagnosed with tracheal bronchial remnants and underwent surgery at our department. Data including demographics, age at surgery, operational methods, complications, outcomes, development of growth, and diet situation were collected. Patients admitted before 2018, who underwent resection of cartilage with stenotic esophageal segment and end-to-end anastomosis through open surgery, were included in Group A. To avoid pyloric obstruction due to the injury of the vagal nerve, pyloroplasty was done at the same time in patients in Group A. Patients admitted after 2018, who underwent longitudinal incision with partial resection of cartilage in the anterior wall of the esophagus and transverse suture through laparoscopy or thoracoscopy, were included in Group B. In Group B patients, pyloroplasty was no longer needed since the injury of the vagal was prevented. To prevent gastroesophageal reflux, Thal or Toupet fundoplication is completed meanwhile in cases received laparotomy and laparoscopy. Oral feed started after the esophagography showed no anastomotic leakage, and patients were discharged when they got full oral feed. Esophagography was reviewed regularly during follow-up. Retrospective research between two groups was performed.
The SPSS v.23.0 was used for statistical analysis. The normal distribution of the variables was checked by the Shapiro–Wilk test. A comparison between Groups was calculated by the Chi-square test and t-test. A P value of <.05 was considered significant. The study was approved by Ethics Committee of Xin Hua Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (Approval no: XHEC-D-2020-188).
Results
Thirteen patients with TBR were enrolled in the study. Table 1 shows the study population demographics of the cohort.
Study Population Demographics
EA, esophageal atresia; PN, parenteral nutrition; SD, standard deviation; TEF, tracheoesophageal fistula.
Five patients in Group A received resection of the stenotic segment and end-to-end anastomosis of the esophagus and pyloroplasty from laparotomy before 2018. The novel surgical approach, including longitudinal incision with partial resection of cartilage (Fig. 1) and transverse suture (Fig. 2), was performed in 8 cases through endoscopy in Group B. Seven patients with cartilage located at the lower part of the esophagus close to the esophagogastric junction underwent surgery laparoscopically. One patient with cartilage in the lower middle part of the esophagus underwent the surgery thoracoscopically. All the patients underwent partial fundoplication, including 10 Thal and 3 Toupet fundoplication, to prevent reflux symptoms at the same time. Table 2 shows a comparison between two groups. There was no statistical difference in the age and weight at the surgery of these patients between two groups. The operation time and the administration time of parenteral nutrition (PN) after surgery in group A patients were longer than those in group B with no statistical significance. The length of hospitalization in Group B was shortened obviously than that in Group A (P < .001). Compared to two cases of anastomotic leakage cured by drainage and conservative treatments occurred in Group A, no anastomotic leakage was observed in Group B. Anastomotic stricture was found in 8 cases postoperatively (two in Group A and six in Group B) and improved obviously after one to five times (M = 2.67) of dilations. The P-value of these complications was negative between these two groups.
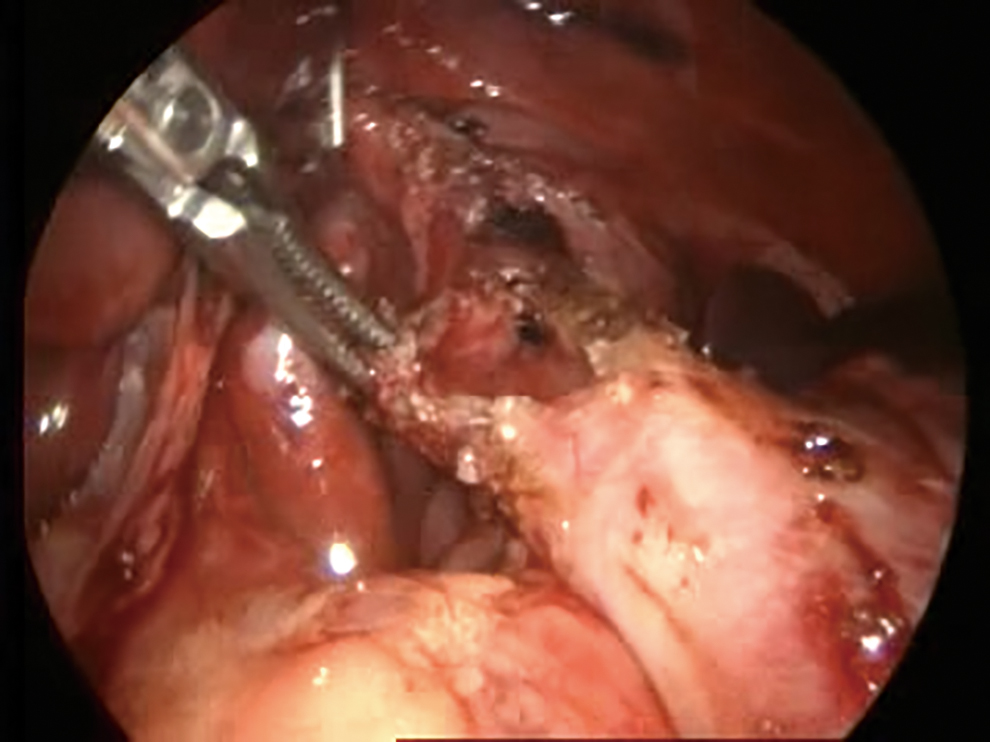
The anterior wall of the esophagus after longitudinal incision with partial resection of cartilage through laparoscopy. Color images are available online.
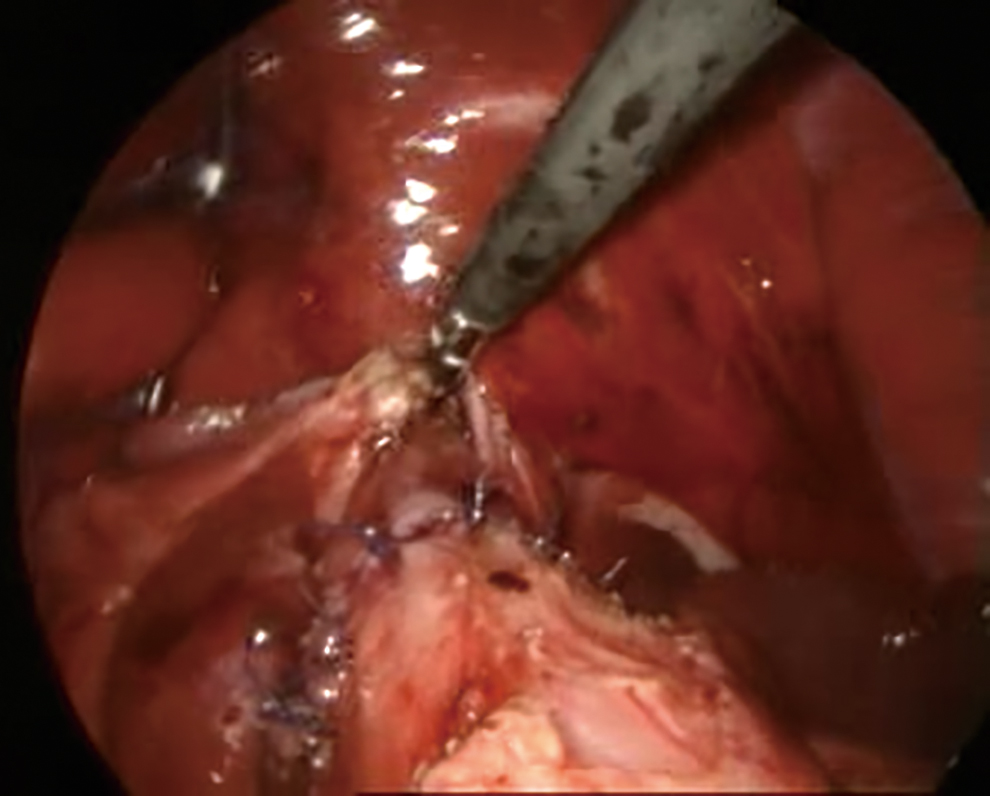
The anterior wall of the esophagus after transverse suture through laparoscopy. Color images are available online.
Comparison Between the Two Types of Surgery
Open surgery: resection of the stenotic segment and end-to-end anastomosis of esophagus and pyloroplasty through laparotomy; Endoscopic Surgery: longitudinal incision with partial resection of cartilage and transverse suture through laparoscopy or thoracoscopy.
Thirteen patients have been followed up for 0.5–45 months (M = 13) after the surgery. Twelve patients are fed by regular diets now, showing good physical and mental development without gastroesophageal reflux symptoms. One case (2 weeks after the surgery) was fed by a soft diet temporarily.
Discussion
According to a literature review, CES is a rare malformation with an incidence of less than 1/25000, and TBR is the most frequent cause. 1 Suzuhigashi et al. 2 and Kawahara et al. 8 reported that CES is frequently associated with esophageal atresia (EA). In this cohort, we found the same status: the incidence of TBR associated with EA was up to 69.2%. Both the trachea and esophagus originates from the foregut in embryonic period,1,9 probably explains the high incidence of TBR associated with EA.
Researches mentioned that the diagnosis of TBR before treatment is often complicated and associated with the delay in diagnosis.10,11 Since esophagography cannot show the cause of the stenosis, endoscopic ultrasonography is recommended by several centers.4,5,12 From our cohort, we found that symptoms such as vomiting, dysphagia, and the eating disorder usually occur in early childhood when they begin to eat solid food. An endoscopic ultrasonic probe can hardly go through the stenotic segment to make a precise diagnosis for infants. In our center, patients diagnosed with CES receive fluoroscopically guided compression balloon dilatation first. Only those who received balloon dilation and showed inextensible stenosis were diagnosed with TBR and enrolled in this study. The diagnosis of TBR was confirmed according to the surgical exploration and pathological examination in all these patients. Stenosis caused by fibromuscular thickening or membranous webbing can be split easily, while the compression balloon cannot be expended at the stenotic segment in patients with TBR due to the existence of cartilage. Thus, it can be seen that compression balloon dilatation is an effective way to make a diagnosis of TBR before the surgery.
Several medical centers have suggested resection of the stenotic esophageal segment and end-to-end anastomosis.6,7,13–15 Although the entire resection of the cartilage can relieve the stenosis, the tension from the proximal and distal esophagus may increase the risk of anastomotic leakage and secondary infections, leading to longer hospitalization. Usually, a cartilage loop exists around the trachea in front of the esophagus to support it and prevent tracheomalacia. The ectopia of the cartilage loop around the esophagus would limit the extensibility and flexibility of muscularis mucosa, leading to stenosis and difficulty in swallowing. It means that partial resection of the cartilage loop is an effective way to relieve the limitation caused by cartilage for esophageal expansion. The transverse suture of the proximal and the distal esophagus can reconstruct the continuance of esophageal muscularis, which was separated by the cartilage ring, and enable peristalsis to be extended to the lower esophagus entirely so that the peristalsis function of the esophagus can be improved. The cicatricial stenosis at the suture postoperation can also be expanded by balloon dilation easily. Therefore, we ameliorated the procedure to longitudinal incision with partial resection of cartilage in the anterior wall of the esophagus and transverse suture through laparoscopy or thoracoscopy after 2018. With the novel approach, the protection of the posterior wall of the esophagus can avoid the injury of the vagal and make it possible not to do the pyloroplasty.
According to the data, we found that the length of hospitalization was shortened in group B patients than those in group A, presenting the therapeutic outcome of the new approach. In our feeding strategy, PN lasted before the esophagography was completed at about 7 days after the surgery. It explained the negative statistical result in the administration time of PN between two groups. However, with a similar time of the PN usage, the hospitalization length was still decreased remarkably, signified the quicker rehabilitation of the esophageal function.
Compared to two cases of anastomotic leakage in Group A, no leakage occurred postoperatively in Group B patients, showing the lower risk of anastomotic leakage after the new approach. The tension of the anastomosis, ischemia, and infection is the primary risk factor of anastomotic leakage. The integrity of the posterior wall of the esophagus can alleviate the anastomotic tension caused by segmental resection effectively. In addition to the relief of the anastomotic tension, tissue ischemia can be protected by the novel approach, which plays a vital role in the precaution of anastomotic leakage.
Despite the limited number of cases with TBR, we can find that the average operation time of the novel procedure with endoscopic surgery was shortened in numerical data (193 ± 32 vs. 156 ± 30, P = .056), also indicated the preponderance of less traumatic and high efficiency of the new procedure.
In this research, anastomotic stricture was found in 8 cases postoperatively, including two cases in group A and six in group B. The new procedure seems to lead to more dilation demands after the surgery (40% vs. 75%, P > .999), but there was no significant difference between two groups in this study. Moreover, we found that the extent of the stricture was slighter after the surgery and can be dilated easily, mostly no more than two times (range 1–5, M = 2.67), whether endoscopic surgery will increase the risk of anastomotic stricture compared to open surgery needs more cases to explore.
In addition to anastomotic leakage and stricture, injury of the vagal nerve is another potential risk of the end-to-end anastomosis. The truncation of the esophagus may damage the vagal, leading to pyloric obstruction and gastrointestinal motility disorders. Setty and Harrison 16 emphasized that pyloroplasty should be considered during a segmental resection of the esophagus. Hence, all the patients in Group A underwent pyloroplasty. Although pyloroplasty was omitted in Group B patients, no pyloric obstruction or delayed gastric emptying was observed in this study. In other words, the pyloroplasty is no longer needed in the novel approach, and the difficulty of the surgery can be simplified.
Besides, we recommend the endoscopic procedure to ameliorate the incision of the surgery. With the help of endoscopy, surgeons can better expose the abdominal or thoracic cavity within the minimal incision. Saka et al. 14 reported two cases of thoracoscopic resection of CES and highlighted the advantage of better cosmetic outcome and prompt recovery. Precisely, the choice of laparoscopy and thoracoscopy is depended on the location of the stenosis. If the cartilage locates at a higher level, the distance between the diaphragm and the stenotic segment is more than one intercostal space, thoracoscopy is recommended. If the stenosis is close to the cardioesophageal junction, laparoscopy is more appropriate.
It should be noted that the fundoplication should be completed at the same time with laparoscopy. Trappey and Hirose 4 and Saka et al. 14 pointed out that gastroesophageal reflux is a significant complication of segmental esophagectomy, fundoplication is recommended as added protection. From our experience, anatomy and traction of the lower esophagus may expand the esophageal hiatus and lead to gastroesophageal reflux when doing resection of cartilage and suture through laparoscopy. Thus, repair of esophageal hiatus and Thal or Toupet fundoplication are an effective way to prevent reflux symptoms. On the contrary, surgery through thoracoscopy suggests a higher location of the cartilage ring (Figs. 3 and 4). For these patients, sufficient releases of the proximal esophagus can relieve the tension of anastomosis and avoid the damage of the esophageal hiatus, so that the fundoplication can be omitted.
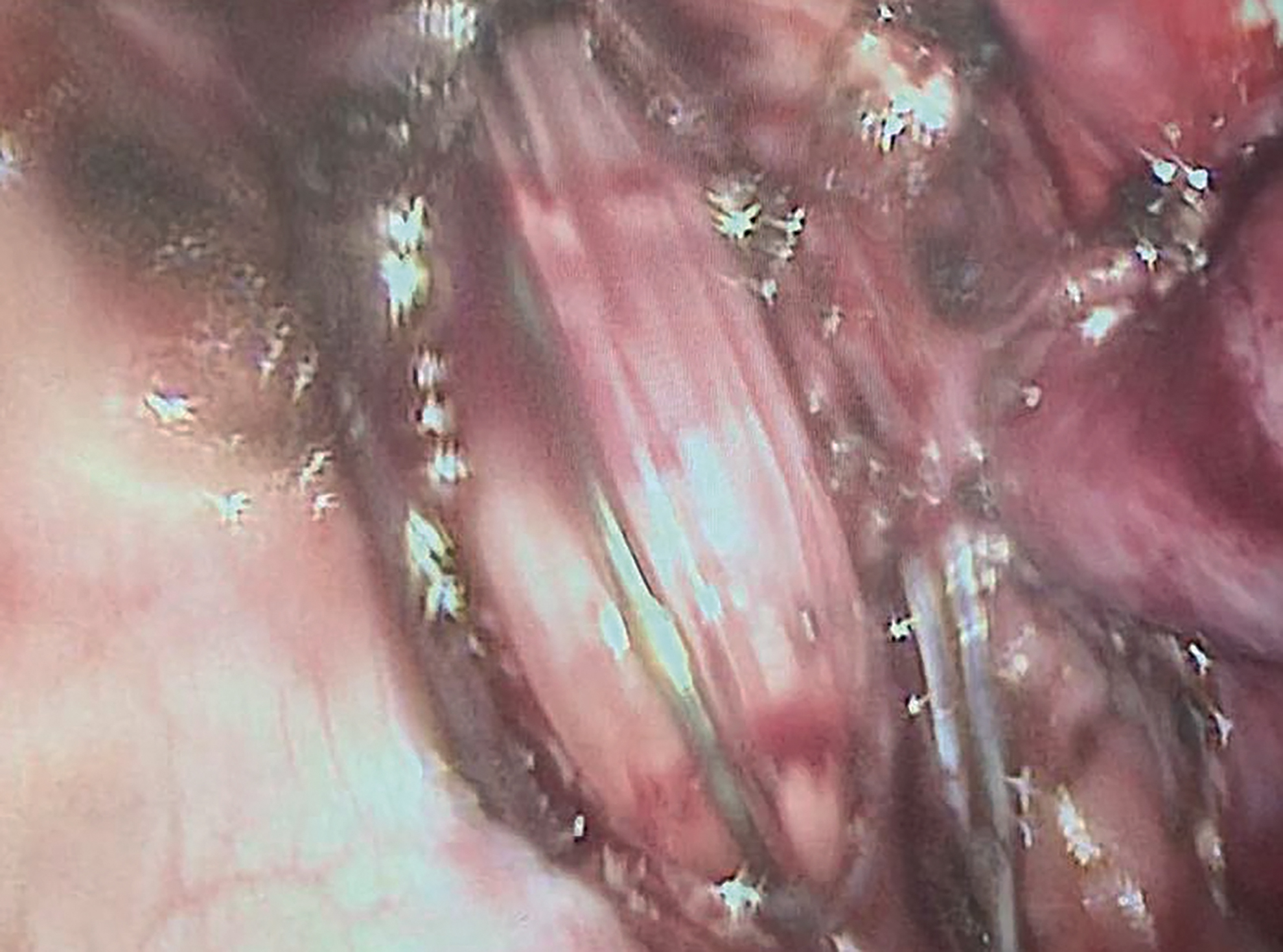
Identify the location of the cartilage by balloon. Color images are available online.
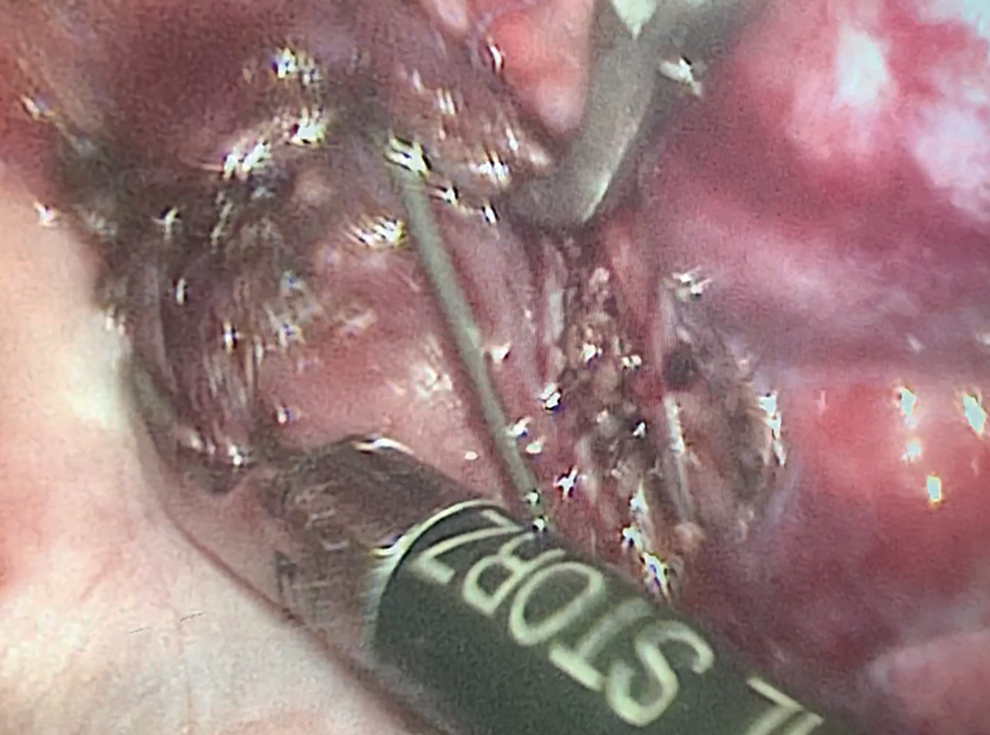
The anterior wall of the esophagus after longitudinal incision and partial resection of the cartilage through thoracoscopy. Color images are available online.
All the others showed good physical and mental development with a regular diet at the average of 13-month follow-up, besides 1 of 13 patients, who was 1 week after the surgery was fed by a soft diet and followed-up regularly at our clinics. Symptoms of gastroesophageal reflux have not been observed during the follow-up, demonstrated the satisfactory effect of the new operation.
In conclusion, longitudinal incision and transverse anastomosis of the anterior wall of the esophagus with partial resection of cartilage endoscopically without pyloroplasty is a novel surgical approach, which is safe and effective for patients with TBR. Compression balloon dilation is conducive to exclude the diagnosis of CES caused by fibromuscular thickening or a membranous web.
Footnotes
Acknowledgment
The abstract of this article has been submitted to the IPEG 2020 program and presented in the 2020 IPEG online meeting.
The authors thank all the staff of the pediatric surgical department of Xinhua Hospital affiliated to Shanghai Jiao Tong University School of Medicine.
Disclosure Statement
No competing financial interests exist.
Funding Information
Shanghai Jiao Tong University Medical-engineering Cross Fund Program (YG2017MS76). Shanghai Science and Technology Commission Program “Biomedical Science and Technology Support Projects” (19441905500). Shanghai Translation Medicine Collaborative Innovation Center Program (TM201910).