
Abstract
Background:
Laparoscopic sleeve gastrectomy (LSG) is currently the most performed bariatric procedure worldwide. We have developed a modification to the usual surgical technique of LSG by adding a Nissen fundoplication.
Objectives:
Provide the technical details of this new bariatric procedure.
Materials and Methods:
The first step of the N-sleeve technique involves dissection and reduction within the abdominal cavity of a possible hiatal hernia and closure of the hiatal orifice. A short 3 cm Nissen valve is created to maintain a gastric fundus as small and functional as possible. After that, the stapling process begins and continues in a standard pattern until the level of the previously created valve. Stapling the stomach around the valve must maintain its natural position and preserve vascularization.
Results:
The following are the five major technical tips: avoid thermic injuries of the gastric wall during short gastric vessel dissection; gently handle the gastric fundus during fundoplication; take the anterior and superior part of the fundus to create the wrap 4 cm from the His angle to avoid a wrong pathway for the food (the food should not go through the wrap); check the good pathway for the food at the end of the operation with the tube by moving it through the esophagogastric junction.
Conclusion:
N-sleeve is a new procedure, technically more challenging than standard LSG, but in our experience, it seems to show similar outcomes in terms of weight loss, effects on comorbidities, and lower rate of leak and gastroesophageal reflux disease.
Introduction
Laparoscopic Sleeve Gastrectomy (LSG) is currently the most worldwide commonly performed bariatric procedure, with the fastest increment rate of the last decade compared to Roux-en-Y gastric bypass (RYGB), the previous standard. 1 Despite its increased acceptance and impressive results on weight loss and comorbidities improvements, there is a growing concern about the relationship between LSG and gastroesophageal reflux disease (GERD).
When patients are suffering from severe GERD before bariatric surgery, the current recommendation is to propose RYGB as a primary operation. However, more than 35% of the patients who underwent RYGB had at least one complication within the 10-year follow-up period. 2 Sandler and others 3 reported on 129,432 RYGB patients, amounting to an overall mortality rate at 1, 5, and 10 years of 2.2%, 4.4%, and 8.1%, respectively. The number of patients hesitating or refusing to accept RYGBP because of long-term complications is important.
The most dreaded complication after LSG is gastric leak, but recent reports showed a decreased incidence to 1%. 4 Himpens et al. 5 reported one of the first experiences with long-term LSG follow-up with limited surgical complications except GERD. Within the 6 years that followed LSG, the same author reported new gastroesophageal reflux complaints in 21% of the patients. Furthermore, three recent studies have emphasized an important rate of Barrett's esophagus after 10 years of sleeve gastrectomy (1.2%–17%).6–8
Considering all of these findings and encouraged by the good results of LSG and concomitant hiatal hernia repair, 9 we have developed a modification to the usual surgical technique of LSG by adding a Nissen fundoplication (N-sleeve). We believe that it can minimize both leaks and heartburn incidence by decreasing the intrathoracic migration of the gastric tube, frequently noticed for regular LSG. Herein, we provide the technical details of this new bariatric procedure.
Materials and Methods
Preoperative management of the patient
The patient was informed about the experimental nature of the study (monocentric prospective evaluation, approved by the local Institutional Review Board) and of this new technique, and he signed an informed consent.
He was evaluated by a Multidisciplinary team, and the evaluation confirmed the surgical indication. A week of protein diet (Bariatric box® Bariawell) was given as part of our routine surgical preparation for all the patients to decrease liver size and to prevent postoperative protein deficiencies.
Results
Surgical technique
All operations were performed under general anesthesia and by laparoscopic approach using the French technique: the surgeon standing between the patient's legs, a first assistant to the left of the patient, and a second assistant to the right with the patient in steep reverse Trendelenburg position with legs abducted. Each procedure required five trocars. Pneumoperitoneum was induced by a primary trocar inserted through the umbilicus with the open technique (Hasson technique). The placement of the trocars did not differ from the standard LSG. A 5 mm epigastric trocar was used for liver retraction. A 5 mm trocar was positioned in at the right paramedian area and a 10 mm on the left midclavicular line. An additional 5 mm trocar was positioned on the left anterior axillary line as represented in (Figs. 1 and 2).
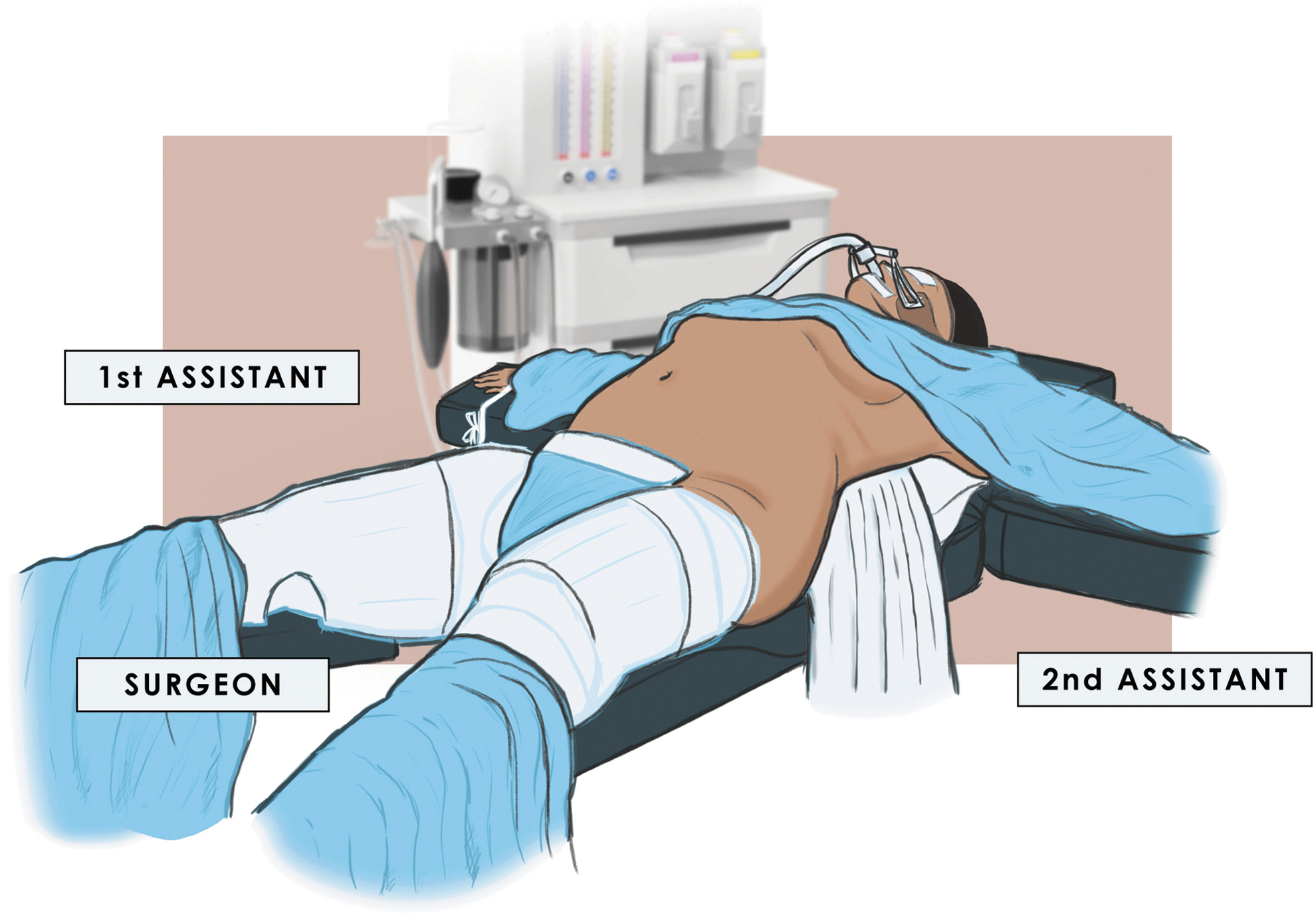
Patient positioning.
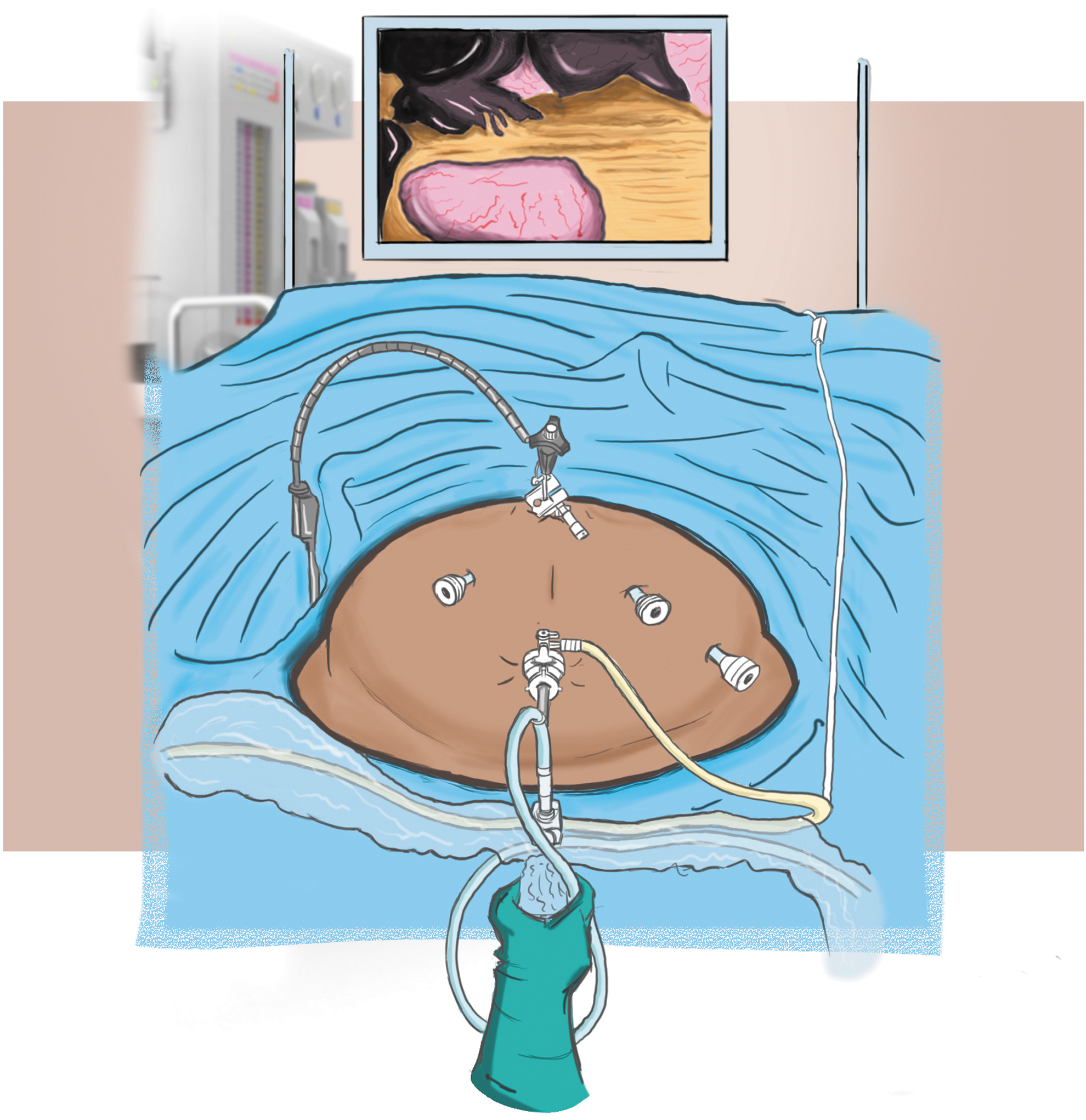
Trocar positioning.
The greater curve of the stomach was dissected from the short gastric vessels and the gastrocolic ligament placed downward as far as 6 cm from the pylorus to preserve the distal antrum, by means of an impedance coagulator Ultracision® (Ethicon Endo-surgery; Johnson-Johnson, Inc., 2010). A careful dissection was performed at the level of the gastric fundus, keeping an appropriate distance from the gastric wall, thus avoiding any possible thermal injury to this important part that would be used later for performing the fundoplication. Total exposition and dissection of the right crus and the gastroesophageal junction are required; and when present, posterior gastric vessels should be divided as well as the attachments to the pancreas so that the stomach can be easily turned on its axis “like the page of a book.” The hepatogastric ligament was opened at the Pars Flaccida, preserving an accessory hepatic artery. Then a complete dissection of the left crus was obtained.
The first step of the N-sleeve technique involves dissection and reduction within the abdominal cavity of a possible hiatal hernia, with the hernia sac and gastroesophageal fat pad being dissected. Lower esophagus was mobilized for at least 5 cm of extension and all the anterior and posterior esophageal space was clearly dissected, keeping the care not to damage the vagus nerve.
The hiatal orifice was closed by approaching the right and left diaphragmatic crus with 1–3 2.0 nonabsorbable interrupted sutures of Ethibond® (Johnson-Johnson, Inc.) calibrated on a 37F tube (Midsleeve®; Medical Innovation Development, Dardilly, France) introduced into the stomach by the anesthetist. A short 3 cm Nissen valve was created using 3.0 Ethibond suture (Johnson-Johnson, Inc.). This valve was created to maintain a gastric fundus as small and functional as possible (Fig. 3). First, 2 fixation points were passed between the left part of the valve, the superficial esophageal layer and then the right side of the valve. The last point was passed between the two sides of the valve (Fig. 4).

Open cadaveric stomach showing the aspect and size of the valve.
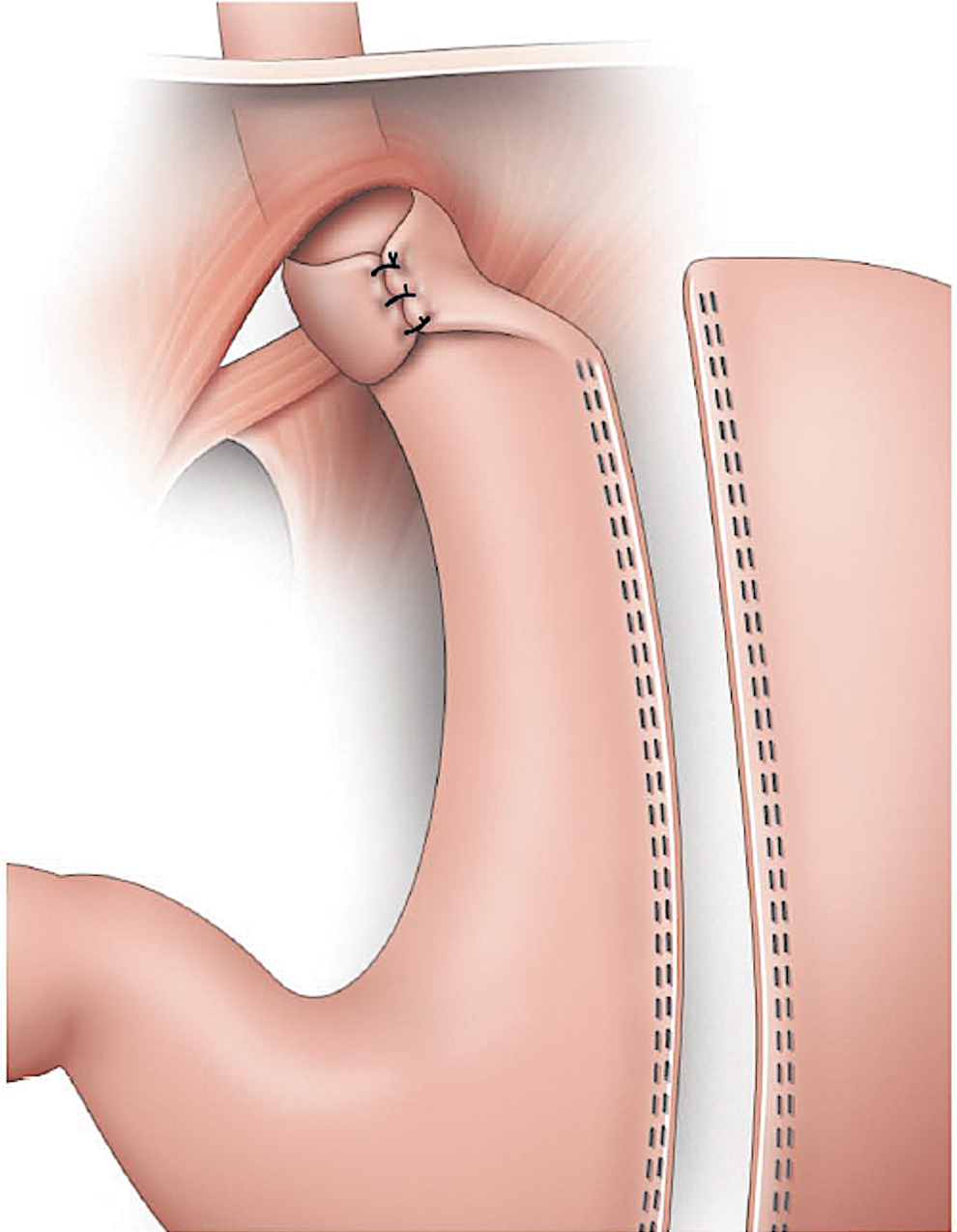
The small Nissen valve before sleeving the stomach.
During the following step, 50 cc of saline solution were inserted in the distal balloon of the Midsleeve (MID Company) positioned at antrum level to define accurately the beginning of the staple line and thus avoid stricture of incisura angularis. A laparoscopic 60 mm Echelon linear stapler with green cartridges® (Ethicon Endosurgery) reinforced by Bioseamguard® (WL Gore) was introduced into the peritoneal cavity and applied alongside the Midsleeve (MID Company) tube, positioned close to the lesser curvature. The instrument was fired and reloaded; and the procedure was repeated for an average of six total firings. While firing the stapler at the level of the new created valve, particular attention must be paid to maintain its natural position and its vascularization preserved. Adequate vascularization of the valve coming from the left gastric artery can be proved by performing an indocyanine green test (Figs. 5–7).
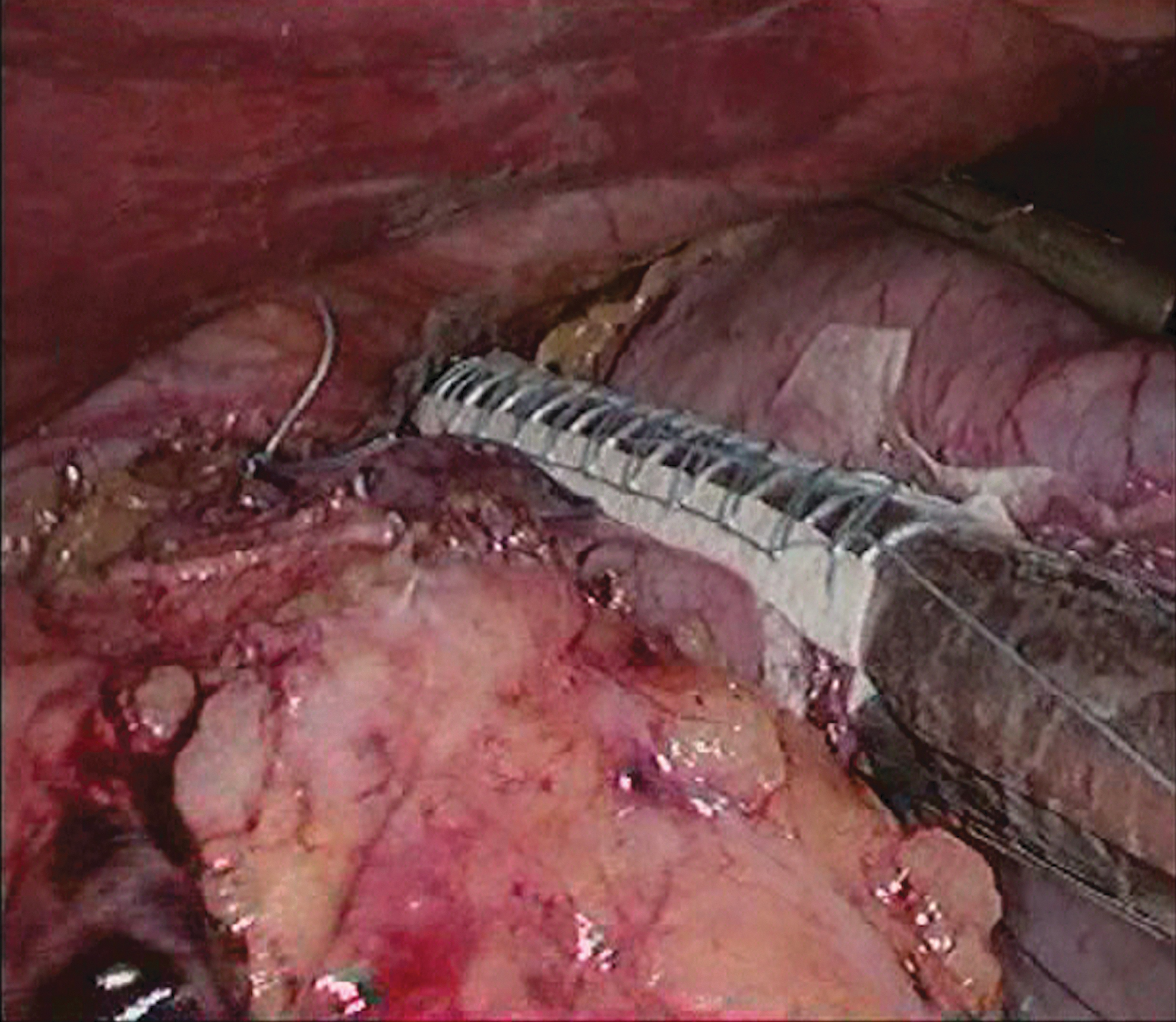
The last firings to create the N-sleeve, taking care to avoid stapling a double stomach fold and preserving vascularization. N-sleeve, Nissen sleeve.

The sleeve finished.
Once the sleeve is finished, Indocyanine green is used to check the vascularization.
At the end of the procedure, we tried to recreate the gastrocolic ligament between the staple line of the sleeved stomach and the cutting edge of the previous gastrocolic ligament by using the BioGlue® (Cryolife).
All the patients received perioperative deep vein thrombosis prophylaxis, using low-molecular-weight heparin and intermittent pneumatic leg compression during the operation and recovery.
Postoperative management involves early oral feeding with liquids and semiliquid diet in the first postoperative day. On the second day, an upper GI series is performed as represented in Figure 8, to confirm a correct barium swallow. With good oral tolerance, the patient can be discharged on the same day. Follow-up is made at 1st, 3rd, and 6th month after surgery, with a control gastroscopy performed at 1 year.

Barium swallow at 2nd postoperative day.
Discussion
The association between obesity and GERD is very well-known. Compared to the general population, obese patients have a threefold increase in its prevalence.6,9–11 A recent study quoted the prevalence of reflux symptoms in the morbidly obese to be over 50%, with >70% demonstrating evidence of reflux disease on PH monitoring. 12 The pathophysiology of GERD in obese patients is notably multifactorial and it includes an altered gastroesophageal gradient pressure due to intragastric and intra-abdominal adiposity compression, in addition to the frequent concomitant presence of hiatal hernia. The current literature shows different results concerning the effect on GERD after LSG, with a significant proportion of patients who improved GERD symptoms and severity of esophagitis.13–15 Angrisani et al. reported a resolution of GERD symptoms in 65% of patients with body mass index <50 at 5 years follow-up, probably explained due to weight loss and visceral adiposity reduction, 16 while others show a substantial number of patients with worsening or persisting GERD, or even de novo GERD after surgery.17–19 This should be linked to the alteration created over the angle of His, which is normally blunted during the surgery; and to lower esophageal sphincter (LES) dysfunction, due to the division of the sling fibers at the fundus, with a resulting LES pressure decrease. In addition, after LSG, the stomach can become conical with the formation of a “neofundus” that serves as a reservoir for food storage leading to gastric stasis and increased acid production. Finally, the resection of the gastric fundus removes an important portion of the stomach responsible for ghrelin production, which can result in slowed gastric emptying and worsening GERD symptoms. 11 N-sleeve was often incriminated for the nonresected fundus, but by the creation of the valve, nonresected fundus is only air filled with no alimentary content, with the purpose to prevent the migration. Even more relevant is the increased prevalence of hiatal hernia associated to patients after SG, variable between 6% and 27%.11,20,21,22 The study by Genco and colleagues showed a lower rate of all classes of esophagitis and Barrett's in patients with concomitant hiatal hernia repair. 7
The International Consensus on LSG in 2012, in which only selected surgeons with an extensive experience on this procedure took part and essentially “focused” on the GERD issue, concluded that hiatal hernia should only be fixed when found. 23 Soricelli et al. 9 concluded that sleeve gastrectomy with hiatal hernia repair is feasible and safe, providing “good” management of GERD in obese patients with reflux symptoms. This subject remains controversial, and we believe that the verdict is still out. Recently, several modifications to the standard LSG have been proposed to control postoperative GERD. Patients with severe GERD preoperatively were treated by Moon et al. with SG and anterior fundoplication, reporting a statistically significant decrease in GERD scores at 3–4 months follow-up. 24 Da Silva et al. performed an alternative technique of sleeve gastroplasty combined with Nissen fundoplication25,26—the laparoscopic sleeve-Collis-Nissen gastroplasty—with 1-year follow-up showing a significant decrease in the prevalence of esophagitis and the use of proton pump inhibitors.
The esophagogastric junction represents an anatomical area of weakness for any digestive suture. The fundic wall is thinner,27,28 and its vascularization is more precarious than in the rest of the stomach. This area under the cardia is more sensitive to any technical failure or to any increase in intragastric pressure. 29 Experience showed us that almost all leaks after LSG originate from this location, namely just below the GE junction. 30 There are substantial differences in the technique of both sleeve gastrectomy and hiatal dissection, and the subsequent alterations in the sling fibers at the angle of His. Moreover, sizing of the sleeve varies, and narrow sleeves have greater intraluminal pressure, which may exacerbate GERD and increase the risk of leakage. Even the concomitant repair of hiatal hernia is challenging, since a loose approximation of the hiatus can predispose to a slip of the now relatively free gastric sleeve. The N-sleeve valve could avoid this potential complication of migration.
Besides GERD control, N-sleeve also adds a possible benefit by lowering the leak rate. The rationale is to cover the angle of His with the antireflux valve and to displace the staple line, thus achieving a better-vascularized area. Our initial results for 25 patients showed no gastric staple line leak and no ischemia of the gastric fundoplication.31,32
Contrary to standard LSG, for the N-sleeve, five extremely important technical details must be observed:
Avoid thermic injuries of the gastric wall during short gastric vessel dissection; Gently handle the gastric fundus during fundoplication; Take the anterior and superior part of the fundus to create the wrap (4 cm from the his angle) (Fig. 9) to avoid a wrong pathway for the food (the food should not go through the wrap) Check at the end of the operation with the tube the good pathway for the food by moving it through the esophagogastric junction. Do not forget that stapling the fundus twice, like a sandwich may cause worst injuries. This can happen when the stomach is not correctly pulled inside the staple before stapling, which could create a blind pouch.

Creating the correct N-sleeve wrap.
In conclusion, the N-sleeve is a new proposal, technically more challenging than standard LSG, but in our experience, it seems to show similar outcomes in terms of weight loss, effects on comorbidities, and lower rate of leak and GERD. As a result, it could really represent an important option for the choice of bariatric procedures.
Footnotes
Disclosure Statement
Marcelo Loureiro, Martha Silvestri, Audrey de Jong, Marius Nedelcu, Mariano Palermo and Almino Ramos have no conflicts of interest or financial ties to disclose. David Nocca received honorarium for speaking engagements from Ethicon Endo-Surgery and Gore and Associates, and created patents for MID.
Funding Information
There was no funding involved to accomplish any of the steps of this study.