
Abstract
Background and Objectives:
Robotic wedge resection for gastrointestinal stromal tumors (GISTs) located in the stomach offers remarkable advantages, especially for lesions in unfavorable places. Although promising, long-term oncological results associated with this surgical procedure are poorly represented in literature. We present our experience of robotic wedge resection with gastrotomy for challenging gastric GISTs, in terms of both surgical outcomes and long-term oncological results.
Methods:
From April 2014 to February 2020, all consecutive patients affected by unfavorably located gastric GISTs (based on the Privette/Al-Thani classification system) underwent robotic wedge resection. Clinicopathological, surgical, and long-term oncological results were retrospectively analyzed.
Results:
Seventeen patients underwent full-thickness gastric wedge resection with primary robot-sewn closure of the defect. In 64.7% of cases, the lesion was ≥5 cm in diameter. No conversion nor tumor rupture were recorded and complete R0 resection was achieved in all cases. Median hospital stay was 5 days (range 3–18). At a median follow-up of 46 months (range 7–67), the disease-free survival rate and the overall survival rate were 94.1% and 82.3%, respectively.
Conclusions:
Robotic wedge resection with gastrotomy and robotic-sewn suture is a safe and feasible procedure for GISTs located in unfavorable anatomic positions, without compromising oncological outcomes.
Introduction
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumors in the digestive tract with a predominantly gastric localization (60%). 1 Due to the rare possibility of lymphatic metastasis, a complete R0 resection is regarded as the standard treatment.2,3 Based on the location, size, and growth of the tumor (intraluminal or extraluminal), different types of gastric resections have been described, including formal partial or total gastrectomy, wedge resection, or transgastric resection. 4
Both traditional and minimally invasive (MI) approaches can be used. In recent times, retrospective case–control studies and propensity-matched analysis have confirmed the benefits of laparoscopy resections in terms of faster recovery, lower perioperative morbidity, overall superior short-term outcomes, and equivalent oncological results when compared with open surgery.5–8 However, in case of large GISTs (i.e., greater than 5 cm in size), the role of laparoscopy is still debated due to the risk of intraoperative tumor rupture and spillage. 2 Furthermore, when tumors are located in unfavorable sites 9 and organ-sparing surgery is planned, laparoscopy can represent a challenge for surgeons since more advanced skills are required especially for the reconstructive phase. 6
Robotic technology, with its advantages in terms of ergonomics, imaging, movements, and suture accuracy, can overcome some shortfalls of conventional laparoscopy, particularly for large and/or difficultly placed gastric GISTs. Presently, the use of robotic surgery for gastric GISTs is poorly represented in literature, except for small case series10–23 and one matched case–control study. 24 Reported experiences evidence acceptable perioperative and functional outcomes with robotic surgery especially for large or unfavorably located gastric GISTs.15,18–20,23 However, little is known about the long-term oncological safety of this type of approach, irrespective of the type of surgical procedure applied.17–19
The aim of this study is to report our experience of robotic full-thickness wedge resection with gastrotomy of unfavorably located gastric GISTs, in terms of surgical outcomes and long-term oncological results. The work was reported according to the criteria set out in the Preferred Reporting of Case Series in Surgery (PROCESS) checklist. 25
Materials and Methods
From April 2014 to February 2020, all consecutive patients who underwent robotic wedge resection at our tertiary center were included in the study. Indication for robotic approach were lesions located in unfavorable gastric sites, such as the gastroesophageal junction, the small curvature, the posterior wall of the stomach, and the prepyloric area according to the Privette/Al-Thani classification system.17,26 All the surgical procedures were performed by a single surgeon (F.B.) with long-standing experience in laparoscopic and robotic surgery.
Preoperative workup included esophagogastroduodenoscopy, thoracoabdominal computed tomography (CT), endoscopic ultrasonography, and core-needle biopsy when clinically indicated. 3 Preoperative treatment with Imatinib mesylate was recommended following a multidisciplinary team meeting according to guidelines. The exclusion criteria ruled out patients with evidence of distant metastasis.
After receipt of Institutional Review Board approval and the signing of a data use agreement, a database of prospectively collected data was created. Patients' characteristics and symptoms in addition to site and diameter of the gastric lesions were recorded. The type of surgical procedure, including the modality of gastric wall reconstruction, total operative time (OT), intraoperative complications, conversion rate, length of hospital stay, reasons for readmission, and postoperative complications, graded according to the Clavien–Dindo classifications, 27 were analyzed. Tumor histopathological characteristics, including growth pattern, presence of ulcerations, mitotic index, and risk grade according to Fletcher's classification were collected. 28
Patients were treated with curative-intent surgery. Adjuvant chemotherapy with Imatinib mesylate was recommended for patients classified as high risk of relapse. 2 All candidates were followed up with routine visits after 1 month, then after 6 months and subsequently every year after surgery. Oncologic outcomes included disease recurrence, defined as a positive result on CT scans, or on ultrasound (US) or positron emission tomography-CT.
Surgical technique
Patient was placed in supine position with 15° reverse Trendelenburg. Trocar layout is shown in Figure 1. The three working arms were equipped with monopolar scissors or a large needle driver in the left flank port (R1), bipolar forceps in the mesogastric port (R2), and Cadiere's fenestrated forceps in the right flank port (R3). Occasionally, an ultrasonic energy device was used in R1.
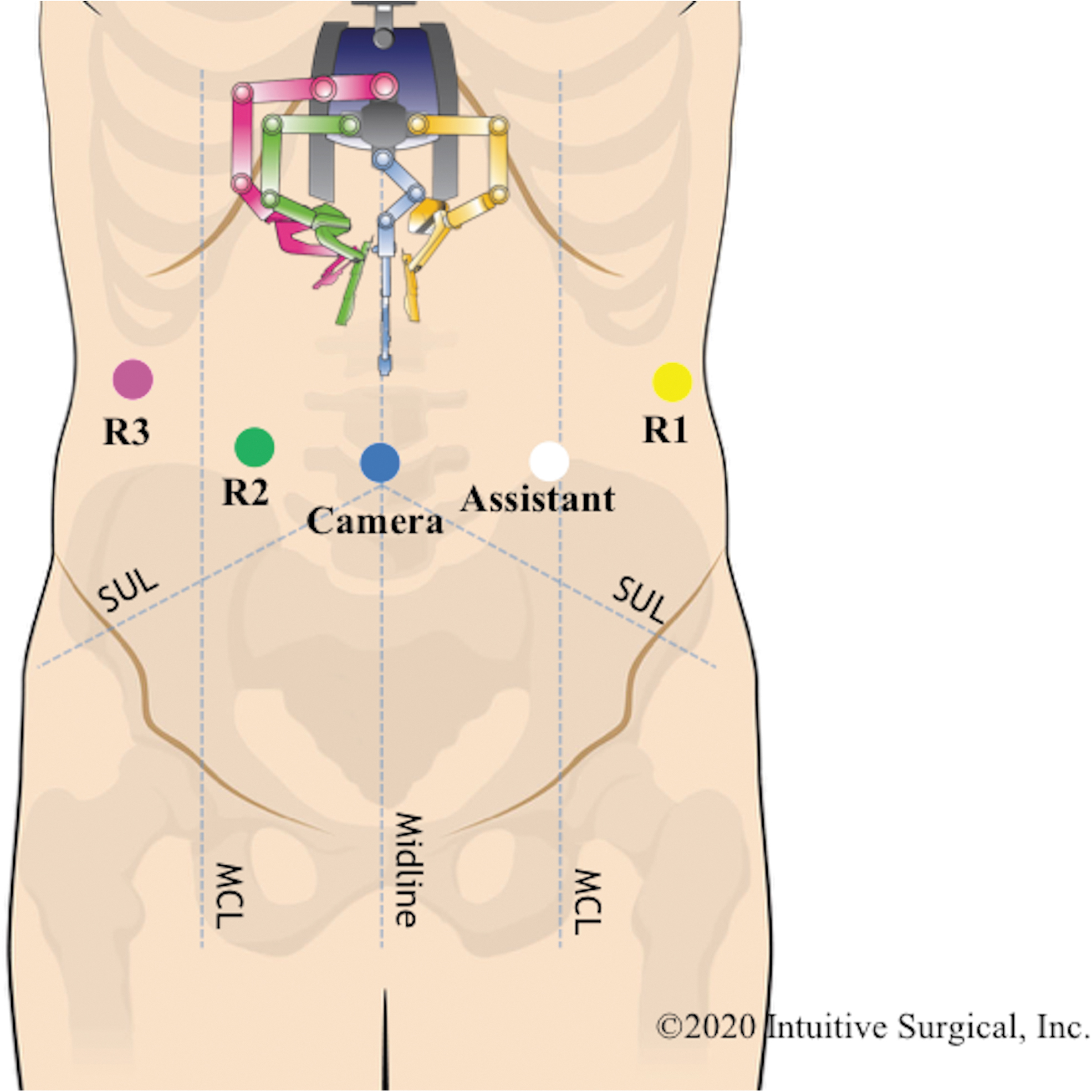
da Vinci® Si™ port layout. A, assistant port; C, camera port; MCL, midclavicular line; R1, robotic arm#1; R2, robotic arm#2; R3, robotic arm#3; SUL, spinoumbilical line.
After the exploration of the abdominal cavity to exclude the presence of metastatic disease, the dV® Si™ was docked over the patient's head, and in certain cases, the left lobe of the liver was retracted toward the abdominal wall using the liver lift method. 29
An intraoperative US or endoscopy was performed to localize the lesion. 30 If surgical criteria of oncological resectability were guaranteed and if feasible, a wedge resection was planned. When necessary, stay sutures were placed on either side of the lesion to lift it away from the stomach, to avoid direct manipulation of the lesion and to facilitate subsequent reconstruction.
A gastrotomy was accomplished and a full-thickness resection of the gastric wall was carried out with at least 1–2 cm of macroscopic free margins. In case of pericardial GISTs, a complete mobilization of the esophagogastric junction was always performed and a 54Ch Maloney bougie dilator was inserted to avoid cardia outlet stenosis.
The specimen was then bagged intracorporeally. Gastric defects were closed with robot-sewn absorbable sutures. If need be, after the robot was undocked, a drain was positioned close to the suture and a nasogastric tube was left in place for 24–48 hours. According to tumor size, the specimen was then removed through a Pfannenstiel incision or just by enlarging the 12-mm assistant port. The closure of the port incisions ended the surgery. Figures 2 and 3 show patient cases #3 and #6, respectively, before and after surgery.
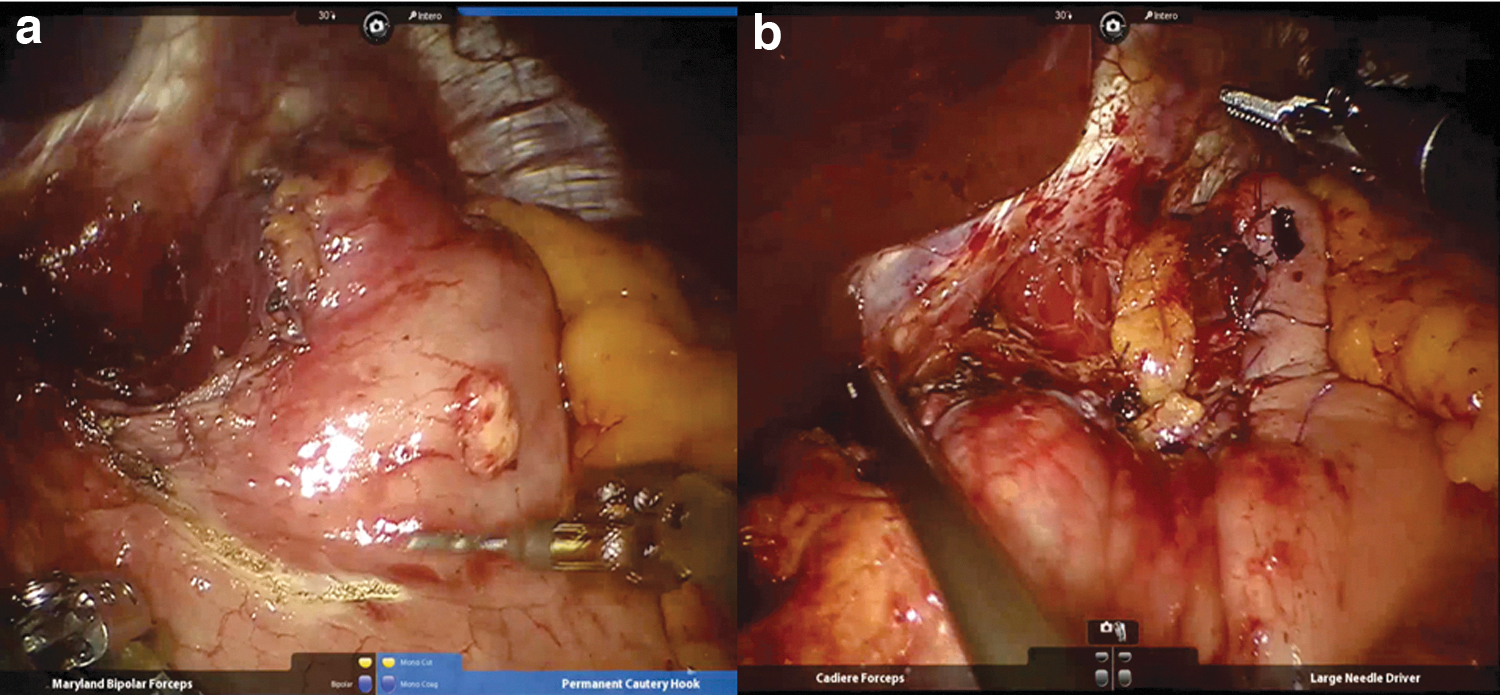
Patient #3: Robotic wedge resection of subcardial gastrointestinal stromal tumor, before
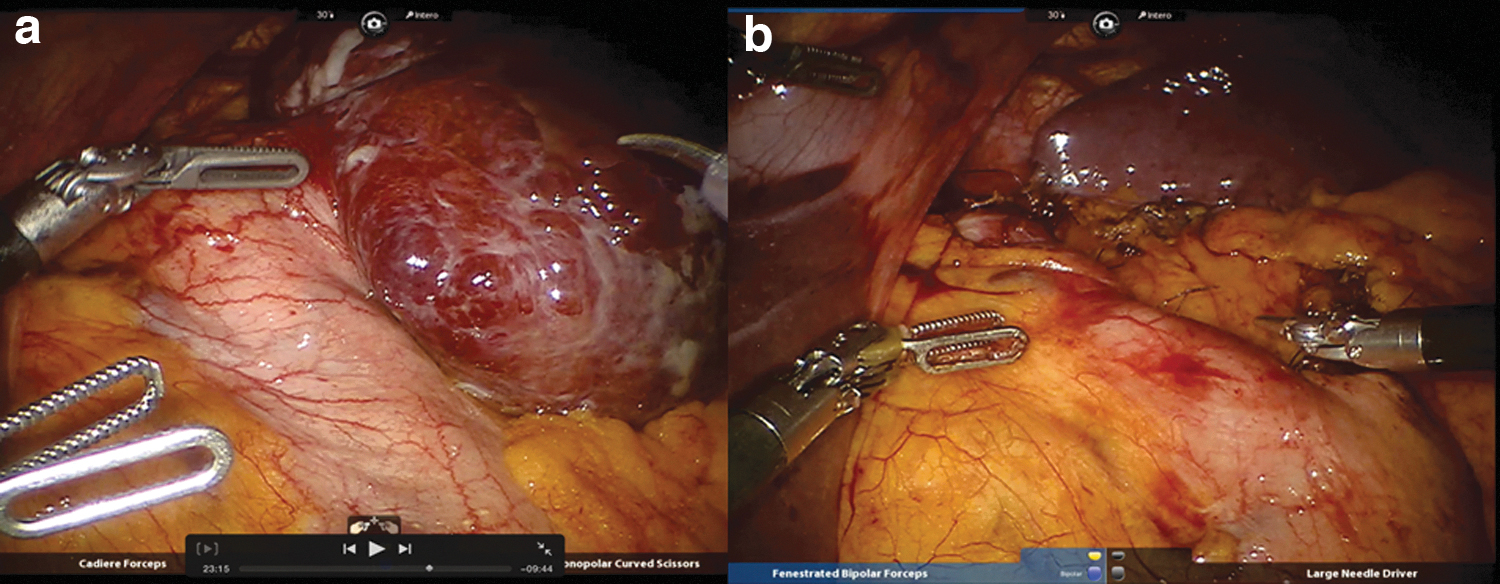
Patient #6: Robotic wedge resection of large gastrointestinal stromal tumor located on the anterior wall of the body of the stomach, before
Results
Seventeen patients (9 females and 8 males) underwent full-thickness gastric wedge resection with primary robot-sewn closure of the defect. In two cases of GISTs located in the posterior wall of the body, an anterior gastrotomy was performed to obtain a safe wedge resection of the posterior wall. Both anterior and posterior gastric breaches were closed with two hemirunning of absorbable suture.
The mean age was 70.2 ± 11.2 years old. Fourteen out of 17 patients were symptomatic. By location, patients were classified based on the Privette/Al-Thani classification system17,26 as follows: type 1 (fundus/greater curve, n = 0), type 2 (antrum/prepyloric, n = 4), type 3 (lesser curve/perigastroesophageal junction, n = 7), and type 4 (posterior wall, n = 6). The mean tumor size was 60 ± 27.5 mm, and in 64.7% of cases the lesion was ≥5 cm in diameter (Table 1).
Clinical Characteristics and Surgical Outcomes
ASA, American Society of Anesthesiology; LOS, length of stay; OT, operative time; PO, postoperative.
Neoadjuvant treatment with Imatinib was administered to 1 patient (case #9). Associated procedures were a distal splenopancreatectomy due to tumor infiltration of the pancreatic tale in one case and a reduction of sliding hiatal hernia with hiatoplasty in another. Intraoperative complications included an iatrogenic transverse colon perforation that was repaired. No tumor pseudocapsule ruptures occurred and no patients required conversion to laparoscopy or open approach.
Estimated blood loss was 50 mL (range 50–100) and median total OT was 200 minutes (range, 105–313). One patient developed a Grade A pancreatic fistula that was treated with antibiotic therapy (Clavien–Dindo 2). No major complications (Clavien–Dindo ≥3), no leakages of the suture nor intra-abdominal infections were recorded. All patients started a solid diet on postoperative day 1 or 2 and the median hospital stay was 5 days (range 3–18). Complete R0 resection was achieved in all cases. Mortality rate at 60 days was nil.
The histological features of each tumor are summarized in Table 2. For 5 patients (29%) in the high-risk group, imatinib (400 mg, orally once daily for 1 year) was recommended as adjuvant therapy. At a median follow-up of 46 months (range, 7–67), the disease-free survival rate and the overall survival rate were 94.1% and 82.3%, respectively. Of note, one disease-related death occurred, in a patient who developed liver recurrence 10 months after the surgery and died of progression disease. Two other patients died with no evidence of GIST-related recurrence.
Histological Evaluation and Oncological Outcomes
Case #2 refused adjuvant treatment.
Case #4 presented Platelet-Derived Growth Factor Receptor Alpha (PDGFRA) mutation that contraindicated adjuvant therapy with Imatinib. 2
From the clinical point of view, there was no evidence of clinical stenosis of the esophagogastric junction or pyloric region nor symptomatic gastroesophageal reflux disease.
Discussion
Our preliminary experience shows that a robotic full-thickness wedge resection with robot-sewn reconstruction is technically feasible for the treatment of unfavorably located gastric GISTs. This type of procedure warranted negative resection margins in all cases and provided acceptable postoperative and long-term functional outcomes. In addition, in our experience, a gastric transection through gastrotomy did not increase the rate of recurrence due to tumor spillage owing to luminal exposure during wedge resection.
Laparoscopic wedge resection has proven to be feasible and oncologically safe for the treatment of gastric GISTs, minimizing morbidity and enhancing recovery. 31 However, if a tumor is located in unfavorable sites, this approach is sometimes challenging and more advanced laparoscopic skills are required. In addition, although the latest guidelines do not state an absolute contraindication regarding the use of laparoscopy for the treatment of large GISTs, 3 the technique can be demanding and requires sound expertise in MI surgery to avoid tumor rupture with its consequent high risk of relapse. 2
Robotic technology can provide some advantages especially in these specific cases, thanks to its well-known technical advantages. 32 To date, although promising, experience with robotic resection for large or unfavorably placed gastric GISTs remains limited (Table 3). Tumor location and size vary between different published series and wedge resection with or without a stapler has been the most commonly implemented technique for the gastric transection.
Summary of Published Case Series of Robotic Resection of Gastric Gastrointestinal Stromal Tumors (n ≥ 3)
Values are expressed as median.
Values expressed as mean.
AW, anterior wall; D, days; DG, distal gastrectomy; GC, great curvature; LC, lesser curvature; M, months; NA, not available; OT, operative time; PW, posterior wall; TG, total gastrectomy; WR, wedge resection.
In our series, all 17 patients were affected by unfavorably located gastric GISTs and in 64.7% of cases the lesion was also ≥5 cm. A R0 robotic wedge resection through gastrotomy was performed in all of the cases without any intraoperative tumor rupture. The choice of the robotic system can help to avoid any direct tumor manipulation, thanks to the steady traction provided by the third robotic arm that grasps the surrounding tissues or holds the threads sutured to the normal serosa around the tumor.
A gastric transection under direct visualization was performed with monopolar forceps or ultrasonic shears thus sparing as much of the stomach as possible, particularly in the case of GISTs with main intragastric growth or those located close to the cardia. The integrity of the gastrointestinal tract was restored with a robot-sewn suture, taking advantage of the wristed articulation of the robotic needle drivers, which simulate the same movements performed in a conventional open operation. 18 Indeed, especially in the area around the esophagogastric junction or in the prepyloric area, a robot-sewn reconstruction after a wedge resection helped to prevent postoperative gastric tract stenosis, which is one of the main complications that should be avoided. We reported 10 cases of GISTs (mean size 60.2 ± 27.8 mm) placed near the cardia and in the prepyloric area without any postoperative stenosis at the 46-month mean follow-up (range 7–67 months). In addition, in case of GISTs near the cardia, the magnified 3D robotic vision facilitated the identification and the sparing of the vagus nerve, thus preventing delayed gastric emptying.
The full-thickness incisions resulting from the gastrotomy may potentially lead to an intraoperative contamination of the abdominal cavity and thereby increase the risk of postoperative intra-abdominal infections. 33 In our study, except for 1 patient (5.9%) who developed pancreatic fistula, no other complications occurred. Our postoperative outcomes are consistent with those reported by other experiences of robotic wedge resection through gastrotomy, in terms of both postoperative complications and length of stay (Table 3).
It is known that the risk of recurrence increases by almost 100% in case of GIST rupture. 34 Furthermore, according to the available literature, the everting/eversion technique can—by opening the gastric lumen—involve the potential risk of peritoneal dissemination, particularly in patients with GIST with ulcerations. 35 However, a study on almost 200 patients showed that laparoscopic wedge resection with gastrotomy for gastric GISTs does not increase the risk of dissemination even in case of ulcerated GIST compared with laparoscopic wedge resection without luminal exposure. 35 During the median follow-up period of 36 months, no patients who underwent a wedge resection with gastrotomy had recurrence. Therefore, the authors concluded that gastrotomy might not increase the rate of recurrence due to tumor spillage by luminal exposure during a MI wedge resection. In light of these promising outcomes, other experiences reporting the same technique have been described with acceptable oncological results.15,17–20,22
In the current series, a gastrotomy was carried out in all cases and we tried to minimize the risk of peritoneal metastasis due to gastric exposure making a comprehensive suction during the gastrotomy and promptly inserting the specimen into an endobag. At a median follow-up of 46 months, the disease-free survival rate was 94.1% with one case of hepatic recurrence in a high-risk patient (case #9). However, a more consistent series of patients with a longer follow-up period is expected to define the exact impact of full-thickness wedge resection with luminal exposure on long-term survival of gastric GISTs.
Our study had some drawbacks. It was a retrospective analysis in a tertiary referral center and it was limited to a quite small series of patients, of whom only 23.5% were at high risk. An additional shortcoming of this study was the lack of a cost analysis that is a crucial issue in our health care system. However, to the best of our knowledge, this is the largest monocentric study with the longest follow-up in literature that specifically focuses on the perioperative, oncological, and functional impact of robotic wedge resection through gastrotomy and intracorporeal robotic gastric wall suture for difficultly placed gastric GISTs.
Conclusion
Robotic full-thickness wedge resection with gastrotomy and robot-sewn reconstruction is a safe and effective treatment for unfavorably located gastric GISTs, with promising long-term functional and oncologic outcomes.
Footnotes
Acknowledgment
The authors thank Mrs. Anna Maria Racca for her significant contribution to revising the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.