
Abstract
Background:
Malignant or benign biliary obstructions can be successfully managed with minimally invasive percutaneous interventions. Since percutaneous approaches are challenging, extensive training using relevant models is fundamental to improve the proficiency of percutaneous physicians. The aim of this experimental study was to develop an in vivo training model in pigs to simulate bile duct dilatation to be used during percutaneous biliary interventions.
Materials and Methods:
Twenty-eight large white pigs were involved and procedures were performed in an experimental hybrid operating room. Under general anesthesia, animals underwent a preoperative magnetic resonance cholangiography (MRC). Afterward, the common bile duct was isolated and ligated laparoscopically. A postoperative MRC was performed 72 hours after the procedure to evaluate bile duct dilatation. The In vivo models presenting an effective dilatation model were included in the hands-on part of a percutaneous surgery training course. Animals were euthanized at the end of the training session.
Results:
Postoperative MRC confirmed the presence of bile duct dilatation in the survival pigs (n = 25). No intraoperative complications occurred and mean operative time was 15.8 ± 5.27 minutes. During the course, 27 trainees could effectively perform percutaneous transhepatic cholangiography, bile duct drainage, biliary duct dilatation, and stent placement, with a > 90% success rate, thereby validating the experimental model. All animals survived during the training procedures and complications occurred in 28.3% of cases.
Conclusion:
The creation of an in vivo bile duct dilatation animal model is feasible with a low short-term mortality. It provides a realistic and meaningful training model in percutaneous biliary procedures.
Introduction
Hands-on training is a key element of minimally invasive surgery education.1–4 Ex vivo surgical models can be sufficient to train for acquiring basic surgical tasks, while training for more complex ones often requires specific in vivo models, which are sometimes difficult to create and unavailable in most teaching facilities. 5 Percutaneous interventions are becoming frequent procedures in the daily surgical practice, including percutaneous transhepatic cholangiography, biliary duct drainage, stent placement, biliary stone retrieval, and bile duct biopsy. 6 However, percutaneous procedures are challenging with a steep learning curve. 5 The availability of virtual simulators 7 or in vivo models 8 to train for percutaneous interventions is still scarce. The development of a simple and effective animal model of biliary dilatation could provide a relevant teaching tool, which could help shorten the learning curve of these highly specialized procedures. The aim of this work was to establish a large animal bile duct dilatation model to be used during percutaneous surgical training procedures.
Materials and Methods
Survival animal models
This experimental study included 28 pigs (Sus scrofa domesticus, ssp. Large White; 16 males and 12 females, mean weight: 28.39 ± 3.01; range: 25 to 33 kg). This study was approved by the Institutional Review Board of the Institute of Image-Guided Surgery, Strasbourg, France. The ethical protocol for animal use was approved by the French National Ethics Committee (Protocol No. 2017071315487959-2017011216428090). The 3R ethical principles (refinement, replacement, and reduction) were strictly followed. Pigs were fasted 24 hours before surgery with free access to water.
The animals were group housed before the procedure and isolated in individual cages for postoperative care, respecting the circadian light/dark cycle and with constant humidity and temperature.
Premedication by intramuscular injection of zolazepam and tiletamine 10 mg/kg IM (Zoletil ND, Virbac) was administered 30 minutes before surgical procedures. Induction was achieved by intravenous propofol 3 mg/kg and rocuronium 0.8 mg/kg (Esmeron ND, MSD France). Anesthesia was maintained with isoflurane 2% (Isoflurin ND, Axience). After the surgical procedure, a survival period of 72 hours was required to achieve bile duct dilatation in the pigs. At the end of the training, animals were euthanized with an intravenous injection of pentobarbital 40 mg/kg IV (Exagon ND, Axience).
Equipment
Surgical procedures were performed under general anesthesia in the experimental hybrid operating room at the IHU-Strasbourg, Institute of Image-Guided Surgery. Magnetic resonance perioperative images were acquired using a magnetic resonance imaging scanner (Magnetom Aera 1.5T; Siemens Healthcare, Forchheim, Germany). High-definition fluoroscopic projection (CIOS alpha; Siemens Healthcare) and ultrasound images (Acuson 300 m; Siemens Healthcare) were acquired during percutaneous procedure training. The laparoscopic equipment (Karl Storz, Tuttlingen, Germany) was used during the laparoscopic approach.
Study design
The study was divided into 2 phases. First, in 3 pigs, a trial phase to assess the feasibility and safety of the in vivo model creation was required. A validation phase in 25 pigs was then completed during a percutaneous surgery training course, which included 27 trainees working under the supervision of experts.
Statistical analysis
Statistical SPSS software was used to analyze the data. Data were expressed on average, standard deviation, and range. The confidence interval was 95% (95% CI) and statistical significance was accepted for P < .05.
Procedures
Laparoscopic bile duct ligation
In 28 pigs, the pneumoperitoneum was induced (12 mmHg). Four laparoscopic trocars were introduced. The common hepatic and bile ducts were exposed through the dissection of the hepatoduodenal ligament (Fig. 1). A vessel ligature (Devon™ Vessel Loops, Covidien, Ireland) was applied proximally in 21 pigs and distally (Polysorb™, Covidien, Ireland) to the cystic duct in 7 pigs. A 2.5 mL intravenous injection of Indocyanine Green was required in 2 pigs to identify the bile ducts with a near-infrared laparoscope.

Common bile duct ligation using a laparoscopic approach.
After the surgical procedures, the pigs underwent a 72-hour survival period. During postoperative and survival periods, surveillance and assessment of pain were required, buprenorphine 0.03 mg/kg IM (Buprecare ND 0.3 mg/mL, Axience) was used on demand. Antibiotic prophylaxis was administered (Amoxicillin, 14.7 mg/kg). A resonance magnetic cholangiography scan was acquired 72 hours after surgery to assess the bile duct dilatation. If the bile duct presented a larger diameter as opposed to the one observed during the previous resonance magnetic cholangiography, the dilatation was considered successful.
Percutaneous biliary interventions
Several percutaneous biliary procedures were performed to validate the training model (Fig. 2).

Percutaneous biliary procedures performed in the in vivo animal models.
Percutaneous transhepatic cholangiography, and internal/external biliary drainage
In 22 pigs, a 21-gauge needle (Chiba Needle 21G; Cook Medical, Inc.) was used under fluoroscopic guidance to reach a bile duct. Iodate contrast medium (VISIPAQUE 270; GE Healthcare, Buckinghamshire, United Kingdom) was injected to perform a transhepatic cholangiography. A 0.018-inch guidewire (Guide-Wire; Cook Medical, Inc.) was then advanced through the needle, and later on, the 21-gauge needle was exchanged for a coaxial introducer set (Neff Introducer Set; Cook Medical, Inc.), which was deployed into the bile ducts. A hydrophilic guidewire (Roadrunner 0.035′′; Cook Medical, Inc.) was introduced and used to insert a biliary drainage catheter (10.2F; Cook Medical, Inc.).
Percutaneous transhepatic cholangioplasty and biliary stenting
In 22 pigs, after a percutaneous transhepatic cholangiography was performed to visualize the biliary tree, a hydrophilic guidewire (Roadrunner 0.035′′; Cook Medical, Inc.) was navigated around the simulated stricture, which was dilated using a balloon catheter (ATB Advance® Balloon Catheter; Cook Medical, Inc.), before stent placement (Zilver 635® Biliary Self-Expanding Stent; Cook Medical, Inc.).
Percutaneous cholecystostomy
In 22 pigs, the gallbladder was punctured using an access 22-gauge needle (Chiba Needle 21G; Cook Medical, Inc.) under ultrasound guidance (Acuson x300 m; Siemens Healthcare), using the Seldinger technique. The appropriate needle position was confirmed with bile aspiration and contrast injection under fluoroscopy guidance. A guidewire was inserted into the gallbladder lumen, followed by serial dilatation, and finally, a multipurpose drain catheter was inserted (10.2F; Cook Medical, Inc.).
Results
Laparoscopic procedures for the in vivo model preparation
Twenty-eight animals underwent laparoscopic bile duct ligation. The data of the surgical procedures are presented in Table 1. Mean operative time was 15.8 ± 5.27 minutes (range: 10 to 25 minutes, 95% CI: 13.76 to 17.84), and was slightly prolonged in 2 pigs presenting with severe perihepatic adhesions, which required laparoscopic adhesiolysis. All animals underwent programmed procedures and recovered from general anesthesia successfully.
Characteristics of Surgical Procedures Used with the Intention of Creating Bile Duct Dilatation in Pigs and Percutaneous Procedures Performed in Animal Models
Bile ducts dilation success.
Percutaneous biliary procedures success.
Complications after laparoscopic approach
There were no intraoperative complications. According to the postoperative morbidity rate (10.7%), 2 pigs developed an early postoperative hernia of the omentum through the 10 mm trocar incision site, which required immediate surgical repair under sedation. After the hernia adverse event was presented, abdominal wall closure techniques were improved. No other complications were reported. There were no differences between the type of surgery performed (distal ligation vs. proximal ligation) and postoperative complications (P = .40). Mortality was reported in 3 pigs after surgery. One died during the magnetic resonance scan performed on postoperative day 3, probably related to the sedation. During the autopsy, no significant findings were reported. Two animals died within 2 days of survival, due to gastric hemorrhage and perforation related to major gastric ulcers. As a result, a standard gastroscopy under sedation was added to the protocol in eight of the surviving pigs. Six animals, with ligation of the distal bile duct, presented with gastric ulcerations. For this reason, intravenous therapy with proton pump inhibitors (PPI) (Omeprazole 80 mg), per oral ursodesoxycholic acid and sucralfate was adapted as well in all animals. No differences were found between the type of procedure (distal vs. proximal ligation) and postoperative mortality (P = .11).
Bile duct dilatation assessment
After 72 hours of survival, a magnetic resonance cholangiography was performed in the operated animals. In all cases, clinically significant bile duct dilatations were observed (Fig. 3).
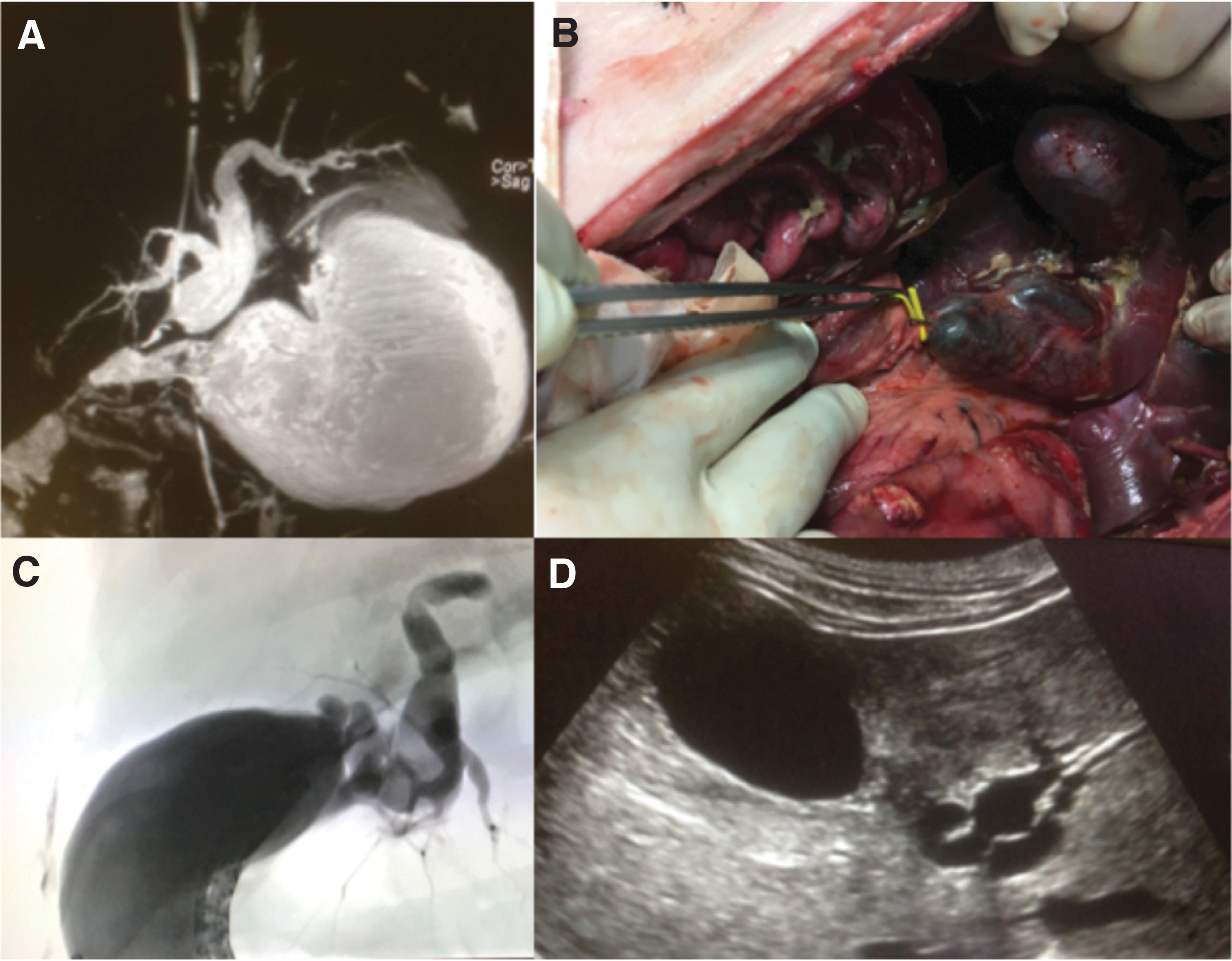
View of the dilated biliary tree using
In vivo model validation
Feasibility pilot study
To validate the model, 4 percutaneous biliary procedures were performed in 3 pigs. At this stage, 2 senior surgeons and interventional radiologists successfully performed 2 percutaneous cholecystostomies and 2 percutaneous transhepatic bile drain placements (Table 1). No complications were reported.
Training validation
Percutaneous biliary procedures (49) were performed in 25 animals during the training course in percutaneous image-guided surgery procedures, in which 27 trainees worked under the supervision of experts (in some cases, more than one operation was performed in the same animal). The percutaneous procedures performed were percutaneous cholecystostomy, percutaneous transhepatic biliary drainage (external and internal–external), percutaneous transhepatic cholangioplasty, and percutaneous biliary stent placement (Table 1).
Total intraoperative complications were n = 15 (28.3%, 95% CI: 0.16 to 0.40), observed in 12 pigs. Bleeding of the abdominal wall n = 3 (5.6%, 95% CI: −0.01 to 0.11), contrast leakage at catheter insertion sites n = 4 (7.5%, 95% CI: 0.00 to 0.14), and involuntary puncture of the portal vein n = 8 (15.1%, 95% CI: 0.05 to 0.25) were reported. No mortality case was reported during percutaneous procedures. The animals were euthanized at the end of the training session.
Discussion
Benign and malignant hepatobiliary diseases are common pathologies in surgical practice. In 2018, it was estimated that 42,220 persons in the United States would be diagnosed with liver cancer and intrahepatic bile duct cancer and an additional 12,190 persons would be diagnosed with gallbladder cancer or another biliary tract cancer. 9 The percutaneous approach is widely used for diagnostic, therapeutic, or palliative purposes in relation to malignant and benign pathologies. 6 Percutaneous transhepatic cholangiography is a safe and effective technique to evaluate biliary abnormalities. 10 It is also a therapeutic option included in the recommendations for acute cholangitis. 11
Percutaneous interventions might be part of the surgical training, and highly specialized skills must be developed. 12 As a result, the development of virtual and in vivo models is fundamental. Different in vivo models to simulate bile duct dilatation were developed, using endoscopic duodenal papilla clipping, 13 peroral cholangioscopy, 14 or laparoscopic double-balloon occlusion device placement. 15 However, complexity exists and a high level of surgical skills is required to create it. The model presented offers advantages, is feasible, safe, realistic, and meaningful, although it requires laparoscopic skills to create it. Its effectiveness in the development of intrahepatic and extrahepatic biliary dilatation was successfully assessed with resonance magnetic cholangiography. On the other hand, the in vivo model allows to perform multiple percutaneous biliary procedures in the same animal, subsequently reducing the number of animals required and respecting the ethical principle of reduction in animal experimentation. The limitations of the model lies in the potential development of gastric ulcers, resulting in the absence of intragastric bile after ligation, which normally buffers the gastric acidity. However, the administration of proton pump inhibitors and endoscopic assessment prevented complications. Finally, the feedback and the level of expertise of the students were heterogeneous, and these variables were not analyzed. This could well impact both the success rate and the rate of intraoperative complications during percutaneous procedures.
Conclusion
The creation of an in vivo bile duct dilatation animal model is feasible with a low short-term mortality. It provides a realistic and meaningful training model in percutaneous biliary procedures.
Footnotes
Acknowledgments
The authors would like to thank Mourad Bouhadjar, the team of IHU and IRCAD radiology technicians, and Guy Temporal for his assistance in proofreading the article.
Authors' Contributions
(1) Study concept: M.E.G. and J.M.X.; (2) Study design: M.E.G. and C.F.D.; (3) Surgical procedures, M.E.G., C.F.D., E.G., M.P., B.D., S.P., P.A.A., and M.D.; (4) Data collection: C.F.D. and A.G.V.; (5) Data analysis: C.F.D. and A.G.V.; (6) Article drafting and submission: A.G.V., J.V., and C.F.D.; (7) Article revision for important intellectual content: M.D., E.H., and J.M.X.; (8) Supervision: M.G. and J.M.X.
Bioethical Aspects
The study received the approval of the institutional and national Ethics Committee (Protocol No. 2017071315487959-2017011216428090) and with due deference to both French laws for animal use and care and the European Community Council Directive (2010/63/EU).
Disclosure Statement
No conflicts of interest to declare: M.G., C.F.D., A.G.V., E.S., M.P., E.H.J., B.D., S.P., M.D., and P.A.A.; Professor Jacques Marescaux: is the President of IRCAD and General Director of the IHU-Strasbourg, which are partly funded by Karl Storz, Medtronic, and Siemens Healthcare.
Funding Information
This work benefited from state aid managed by the French National Research Agency (ANR) under the “investissements d'avenir” program with the reference, ANR-10-IAHU-02.