
Abstract
Background:
Bariatric surgery is an effective treatment for obesity and its associated morbidities. They are safe surgeries, their general complication rate is 0%–10%. However, acute gastric dilation is an unusual complication. It requires rapid diagnosis and treatment to avoid major complications. Image-guided surgery represents a group of minimally invasive procedures. Acute gastric dilation is a complication that can benefit from the application of this type of procedure. We present a report of patients with acute gastric dilation of the remnant as a complication after bariatric surgery, its resolution through image-guided surgery, and updating.
Materials and Methods:
A retrospective review of patients who presented postoperative complications after bariatric surgery was carried out. The time period was 10 years. All patients were operated on in a single center by the same surgical team.
Results:
A total of 3507 bariatric procedures were analyzed (sleeve gastrectomy, 1929—55.1% ± 0.49%; Roux-en-Y gastric bypass [RYGB], 1403—40% ± 0.48%; other techniques, 175—4.9% ± 0.21%). The RYGB branch reported a total of 11 (0.78% ± 0.08%) complications, of which 2 (0.14% ± 0.03%) were reported as acute gastric dilation of the remnant.
Conclusions:
Acute gastric dilation of the post-RYGB remnant is a rare complication, but it can be serious. It is necessary to have a high suspicion to obtain an early diagnosis and treatment. Percutaneous gastrostomy is an image-guided procedure that can solve the problem temporarily or permanently.
Introduction
It is a proven fact that bariatric surgery is an effective treatment for obesity and its associated morbidities. 1 There are a wide variety of types of bariatric procedures, although the most widespread are sleeve gastrectomy (SG) and Roux-en-Y gastric bypass (RYGB).2,3 They are safe surgeries, whose general complication rate is 0%–10%. 4 The most frequent are leaks and bleeding, among others. Acute gastric dilation is an unusual complication (0%–0.8%) 5 that affects the gastric remnant of the RYGB. It is necessary to have a high suspicion as it can be serious. For this reason it requires rapid diagnosis and treatment to avoid major complications.
Image-guided surgery represents a group of minimally invasive procedures.6–8 It has the characteristic of being carried out with the support of various imaging systems (fluoroscopy, ultrasonography, tomography, and resonance). 9 Its advantages such as minimally invasive, fast recovery, and low rate of complications put it in a favorable position for the treatment of complications in bariatric surgery. 10 Acute gastric dilation is a complication that can benefit from the application of this type of procedure.
Objectives
The objective of this study was to present a case report of patients with acute gastric dilation as a complication after bariatric surgery, its resolution through image-guided surgery, and an update.
Materials and Methods
A retrospective review of patients who presented with postoperative complications after bariatric surgery was carried out, analyzing in particular the presence of acute gastric dilation of the post-RYGB remnant. The time period was 10 years (from 2009 to 2019). All patients were operated on in a single center by the same surgical team (Diagnomed, Buenos Aires, Argentina). The following selection criteria were established: (1) inclusion criteria: acute gastric dilation of the RYGB remnant in the postoperative period, previous normal upper gastrointestinal (UGI) endoscopy study; (2) exclusion criteria: acute gastric dilation secondary to metabolic alteration, acute gastric dilation secondary to drug intake, acute gastric dilation associated with another complication (for example, peritoneal ileus due to peritonitis or hemoperitoneum), and presence of signs and symptoms of delayed gastric emptying and/or gastroparesis in preoperative studies (UGI radiographic series).
Bioethical aspects
All participants signed an informed consent. The study was approved by the bioethics committee of the participating hospitals.
Results
A total of 3507 bariatric procedures of our team in a single center were analyzed retrospectively. Of this, 1929 (55.1% ± 0.49%) were SG, 1403 (40% ± 0.48%) were RYGB, and 175 (4.9% ± 0.21%) were other types of surgeries. The analysis of the complications of the RYGB branch reported a total of 11 (0.78% ± 0.08%) complications, of which 2 (0.14% ± 0.03%) were reported as acute gastric dilation of the remnant (Table 1). When performing the disaggregated critical analysis of post-RYGB complications, acute gastric dilation corresponded to 18.1% ± 0.40%.
Demographic Data
BMI, body mass index; DLP, dyslipidemia; F, female; HBP, high blood pressure; RYGB, Roux-en-Y gastric bypass.
Clinical case 1
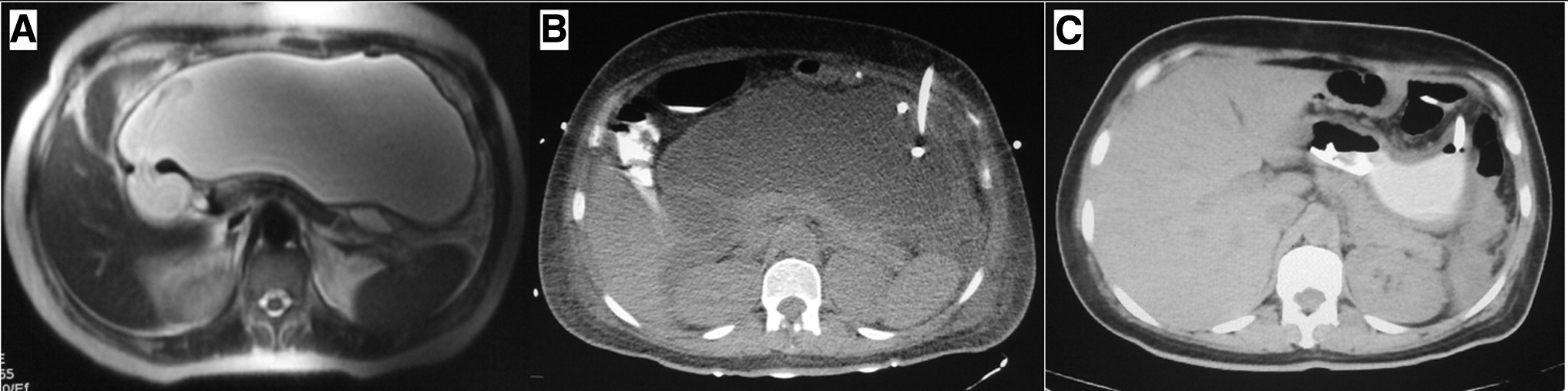
A 43-year-old female patient presented with a body mass index (BMI) of 41 kg/m2, and high blood pressure (HBD) as associated morbidity. Full preoperative studies revealed no other problems. She underwent RYGB, which was a standard procedure with no intraoperative complications. On postoperative day 12, she presented with mild abdominal pain, which then became more intense. Then digestive intolerance, nausea, and vomiting were added, which did not subside with antiemetics. Physical examination revealed a mild–moderately distended abdomen, with pain in the epigastrium, together with a decrease in the stool rhythm. The patient was admitted to the hospital and initial studies were performed. Analyses report mild leukocytosis, whereas abdominal ultrasonography does not provide relevant data. A computed tomography (CT) scan of the abdomen revealed a large dilation of the gastric remnant with liquid content (Fig. 1A). With the diagnosis of acute gastric dilation, and taking into account the increasingly intense symptoms of the patient, a gastric decompression was performed by means of a percutaneous gastrostomy (Fig. 1B, C). Once the initial symptoms had resolved, studies with fluoroscopy with oral contrast were completed, which resulted in a stenosis of the entero-entero anastomosis. Revision surgery with laparoscopic reconstruction of this anastomosis was performed as definitive treatment.
Clinical case 2
A 49-year-old female patient presented with a BMI of 38 kg/m2, and associated morbidity of HBD and dyslipidemia. Laparoscopic cholecystectomy was reported 5 years ago as a surgical history. After completing the preoperative studies, she underwent RYGB. The procedure did not present intraoperative complications, but only the release of some surgical adhesions from the liver to the round ligament. She had an immediate postoperative period without problems, until on day 34 she reported symptoms of abdominal distention. As the weeks went by, she had nausea and abdominal pain, despite fluid tolerance. The intestinal transit was preserved. After she was admitted to the hospital, physical examination revealed bloating on percussion, and radiology revealed great gastric dilation. Abdominal CT scan confirmed acute gastric dilation of the gastric remnant. Percutaneous gastrostomy was performed without complications. The study was completed with a gastrointestinal radiographic series, not observing stenosis or sites of obstruction throughout the digestive tract. The patient presented a good evolution, with oral tolerance at 48 hours, discharge at 72 hours, and removal of the gastrostomy catheter at 28 days.
Percutaneous gastrostomy (radiologically inserted gastrostomy)
Percutaneous gastrostomy (or radiologically inserted gastrostomy “RIG”) is an image-guided procedure that involves placing a catheter into the stomach. Being a minimally invasive surgery, it has the advantages of little pain, low complication rate, and quick recovery. It has a 95%–100% success rate and 5.9% complications. 11 It should be taken into account that in patients with acute gastric dilation of the post-RYGB gastric remnant, there are some changes with respect to the usual technique.
The procedure should be carried out in an operating room with the support of a fluoroscopy equipment. The patient was placed in a supine position. The vital parameters were controlled by an anesthesiologist, who performed general anesthesia with endotracheal intubation, reducing the risk of gastric content aspiration. In addition, the placement of a nasogastric tube is requested to evacuate the stomach, thus avoiding the accidental leakage of its contents to the abdomen during the puncture of the stomach. Using aseptic technique, a surgical field was formed in the upper abdominal region. Initial fluoroscopy was necessary to determine the location of the gastric remnant and determine the puncture site (Fig. 2A). Air was blown into the stomach for distention. In this way, it will come into contact with the anterior abdominal wall. Once the access site is defined, a local anesthetic is infiltrated (Fig. 2B). A 21G (gauge) needle was inserted into the dilated gastric remnant and contrast was injected to confirm its correct position. Then, the needle was changed for a larger gauge (14G), through which two attachment points were introduced. The purpose of this was to fix the anterior gastric wall to the anterior abdominal wall. A 0.035″ guidewire was then passed through the needle, which was removed, holding the guidewire in place. The abdominal wall was progressively dilated with 10 to 14F (French) dilators. Once the dilators were removed, a 14F gastrostomy catheter was placed (Fig. 2C). This entire procedure was verified with fluoroscopy. In this step, proper placement of the catheter can be verified with the outlet of air and gastric fluid through it (Fig. 2D). The guidewire was removed and the catheter was secured with skin stitches and the “pig tail” safety attached to such devices (Fig. 2E). A final control fluoroscopy was performed with contrast injection through the catheter to confirm its correct position and finish the procedure.
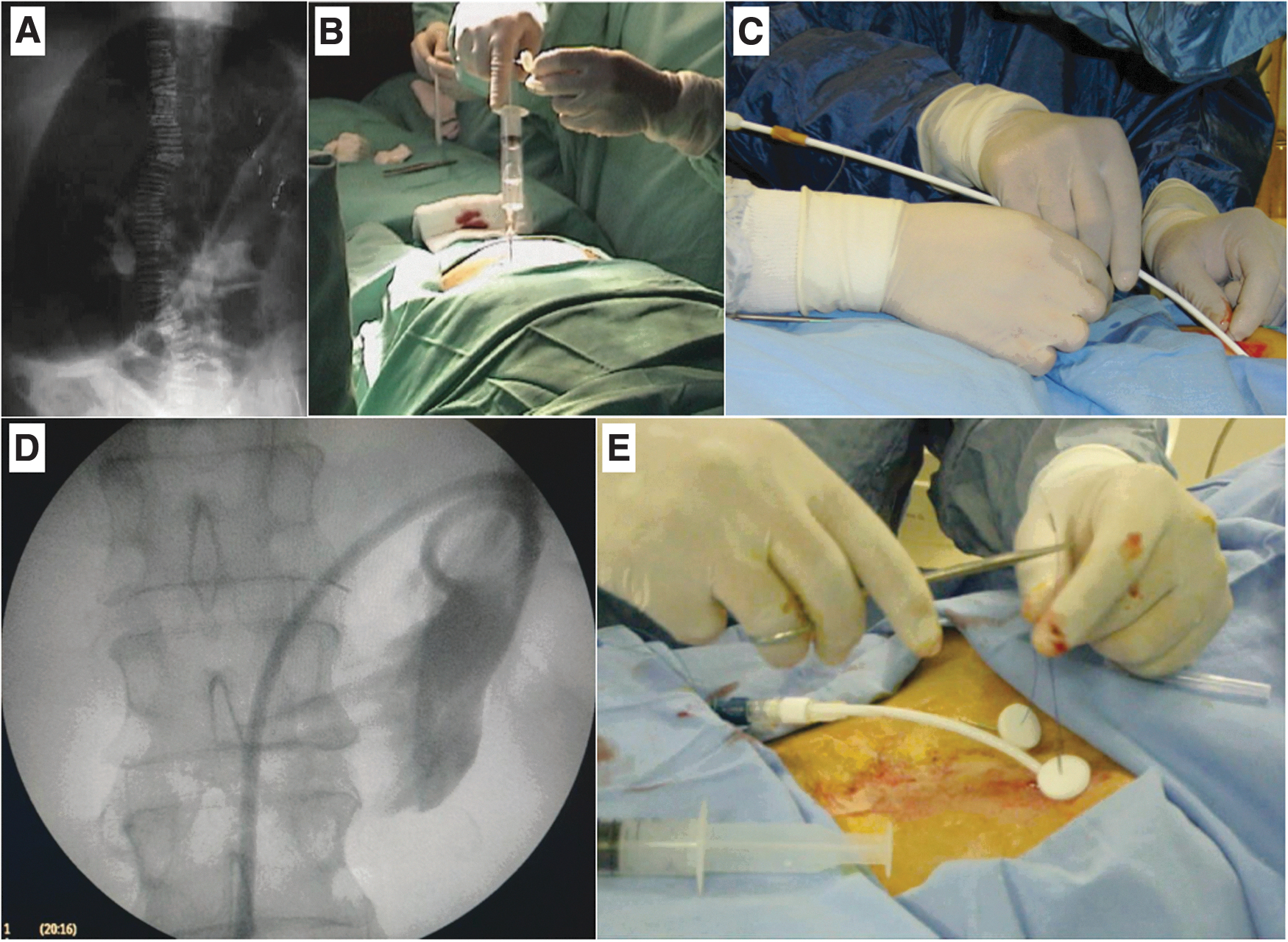
Percutaneous gastrostomy.
Discussion
Acute gastric dilation is the rapid and progressive increase in the volume of the gastric remnant in RYGB. Although one of its causes can be attributed to enteroenteric anastomosis stenosis, on some occasions its pathophysiology is not entirely clear. It is known that diabetic neuropathy generates potentially severe gastroparesis,12–14 although we are not in a position to affirm that this association is the origin of the dilation of the remnant in the postoperative period in all cases. There was also no relationship with the age of the patient. 15
It is a rare complication in bariatric surgery in general,16,17 as well as in RYGB in particular. Its clinical presentation usually appears weeks or months after the procedure. The prevalent symptoms are abdominal pain, distention, nausea, vomiting, and occasionally reflux. The diagnosis is based on medical images, especially CT, since due to the anatomical modification it is not possible to perform UGI endoscopy. 18 With CT, the large dilation of the gastric remnant and its content (air, fluid, or both) can be observed, and it also allows to rule out other complications, such as leaks and collections. The latter can generate a local peritoneal reaction that results in a regional gastric ileus that simulates gastric dilation. Treatment consists of gastric decompression as soon as possible, and resolution of the definitive problem in a second stage, if necessary.
The preoperative diagnosis of a dysfunctional stomach is not associated with acute gastric dilation. However, some authors suggest routine UGI endoscopy for all patients who are candidates for surgery, although others recommend that endoscopy be selective. This allows a correct selection of the procedure. 19 Furthermore, the UGI endoscopy could be very useful to predict the perforation of the gastric remnant, since the cause of this rare complication may be the presence of an ulcer or the development of gastric cancer.20–22 The UGI radiographic series is also a routine study in all patients who are candidates for bariatric surgery. Although not considered strictly necessary by all authors, it can provide information on hiatal hernia, anatomy, presence of gastric dilation, or delayed gastric emptying.23,24
In the 2 cases we reported, none of the patients had previous symptoms of gastroparesis or gastric pathology confirmed by endoscopy. They also did not have diabetes mellitus as a background. In one of the cases, it could be concluded that the dilation of the gastric remnant was secondary to the stenosis of the entero-entero anastomosis. However, it is striking that the case that was reported initially presented gastric dilation, not a typical clinical case of abdominal obstruction. Although the CT scan showed the presence of fluid inside the stomach, in the other case only air was observed. This could be due to the fact that in the latter patient, the cause of acute gastric dilation was not obstructive, corroborated by the study of normal gastrointestinal transit.
The most commonly used techniques for gastrostomy in minimally invasive surgery are endoscopic (percutaneous endoscopic gastrostomy “PEG”) and radiological (“RIG”).11,25,26 Less common is per-oral image-guided gastrostomy (PIG). Surgical gastrostomy in many cases became a second-line indication in selected patients. Anatomical modification after RYGB does not allow for PEG, so RIG is the recommended technique. The application of image-guided percutaneous gastrostomy surgery gave good results in these patients. When it was not possible to solve the problem with a single procedure, at least it was tried to improve the symptoms for a while, then to treat it definitely. They were procedures that required a short intraoperative time, without perioperative complications. Symptoms improved within a few days, as did the patients' condition. One of the main disadvantages of RIG is the small diameter of the catheters used in this technique. 27 This could be a limitation in patients requiring gastrostomies for enteral feeding. But in this case report, the goal of this procedure was gastric decompression, which was successfully achieved. 28
Perhaps there is a mixed pathophysiological origin (nerve injury during the section of the stomach, plus underlying neuropathy, associated with concomitant gastric pathology) that explains the development of acute gastric dilation of the remnant. The literature on this complication is brief and it is clear that clinical trials are required to answer this question.
Conclusions
Acute gastric dilation of the post-RYGB remnant is a rare complication, but it can be serious. It is necessary to have a high suspicion to obtain an early diagnosis and treatment. Percutaneous gastrostomy is an image-guided procedure that can solve the problem temporarily or permanently.
Footnotes
Acknowledgment
We wish to thank Felipe Alvear, MD, research fellow of the DAICIM Foundation in Buenos Aires, for editing of the images in this article.
Informed Consents
All patients signed an informed consent to participate in the research and to allow us to use their data for publication.
Ethical Approval
Approval of our institutional ethics committee was obtained before the start of the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.