
Abstract
Objective:
The effectiveness and feasibility of the primary closure after laparoscopic common bile duct exploration (LCBDE) have been well demonstrated, however, the incidence of postoperative bile leakage after LCBDE remains high. The current study aimed at investigating whether our new suturing method could reduce the risk of bile leakage after LCBDE.
Materials and Methods:
This retrospective study included 81 patients who underwent primary two-layered closure or traditional primary closure of the common bile duct (CBD) after LCBDE, and the related clinical data were compared and analyzed.
Results:
The primary two-layered closure group had a lower rate of bile leakage compared with the traditional primary closure group (P < .05). There were no significant differences in additional parameters, such as operative time, estimated blood loss, postoperative stay duration, time to drain removal, postoperative pancreatitis, stone recurrence, and overall morbidity. No patients developed bile duct stenosis during the follow-up period.
Conclusions:
Primary two-layered closure of CBD can reduce the postoperative bile leakage after LCBDE. Moreover, it is a safe and effective therapeutic option for patients with choledocholithiasis.
Introduction
Laparoscopic common bile duct exploration (LCBDE) has become the most common surgical procedure in the treatment of choledocholithiasis. In the majority of cases, a T-tube insertion is needed after LCBDE to prevent postoperative common bile duct (CBD) stricture and bile leakage. Nevertheless, T-tube drainage is often associated with complications, including displacement of the T-tube, bile leakage after extubation, electrolyte disorders, and prolonged hospitalization, and it has a serious impact on the quality of life of patients. 1 Many studies have recently shown that primary closure of the CBD after LCBDE provides better outcomes than the T-tube drainage,2,3 but postoperative bile leakage remains one of the most considerable concerns for physicians. To reduce the incidence of postoperative bile leakage, we propose a new suturing method allowing for the closure of the CBD incision. This study aimed at investigating whether primary two-layered closure of CBD could reduce bile leakage after LCBDE.
Materials and Methods
We performed a retrospective analysis of 81 patients who underwent LCBDE between January 2018 and March 2020 at our department after a diagnosis of choledocholithiasis. According to the type of CBD closure, patients were divided into the primary two-layered closure group (n = 41) and the traditional primary closure group (n = 40). Choledocholithiasis was diagnosed by imaging examinations, including ultrasonography, computed tomography (CT), or magnetic resonance cholangiopancreatography (MRCP).
Patients with acute pancreatitis, acute suppurative cholangitis, calculus of an intrahepatic duct, history of previous abdominal surgery, or conversion to open surgery were excluded. Demographic characteristics and additional data such as age, sex, serum bilirubin level, CBD diameter, number of stones in CBD, and maximum diameter of stones were recorded by the research team. Intraoperative and postoperative outcomes were compared and analyzed. The study was approved by the Ethics Committee of Zigong First People's Hospital, and written informed consent was obtained from all patients.
Surgical technique
No laparoscopic surgery contraindications were seen in all patients. After a routine preoperative preparation, all patients underwent general anesthesia. Surgery was carried out with a four-port approach. The gallbladder was retracted to expose the Calot's triangle on entering the abdominal cavity, and the cystic artery and cystic duct were dissected and ligated with absorbable clips. The gallbladder was then dissected from the liver bed. Before choledochotomy, the anterior wall of the CBD was clearly exposed. A longitudinal choledochotomy of about 8–10 mm was made by electrocautery. Choledochoscopy was inserted into the CBD for detection. Under the choledochoscopic vision, CBD stones were removed with a saline flush or extracted by using a stone basket. If the stones were too large or impacted at the ampulla, biliary lithotripsy was usually performed. CBD clearance was confirmed by direct visualization downward to the ampulla of Vater and upward to the bifurcation of the left and right hepatic ducts.
After removing the stones, patients were divided into the primary two-layered closure group and the traditional primary closure group. In the primary two-layered closure group, patients underwent a two-layered closure of CBD. In the first layer, the CBD was closed with absorbable 5-0 PDS II sutures (Ethicon, Inc., Somerville, NJ) in an interrupted fashion (Fig. 1A). In the second layer, the serosa of the anterior wall of CBD was closed from the bottom to top in a continuous fashion (Fig. 1B). In the traditional primary closure group, the CBD was closed by a single layer with the same suture material and technique as the first layer in the primary two-layered closure group. After ensuring no bile leakage, drainage was placed near the Winslow hole and fixed on the port of the right anterior axillary line in both groups. The suction drain was removed 3–4 days after the surgery in the absence of bile leakage. Intraoperative data were collected and included the operative time and estimated blood loss. Postoperative outcomes included peritoneal drainage of the first 3 days, time to drain removal, postoperative stay duration, postoperative pancreatitis, stone recurrence, bile duct stenosis, and overall morbidity. Postoperative follow-up visits were scheduled 2, 6, and 12 months after the surgery to assess the clinical status of patients. Blood tests, liver function tests, and abdominal ultrasonography were performed at every follow-up. Imaging examinations such as MRCP or CT were performed if any unusual findings were detected.
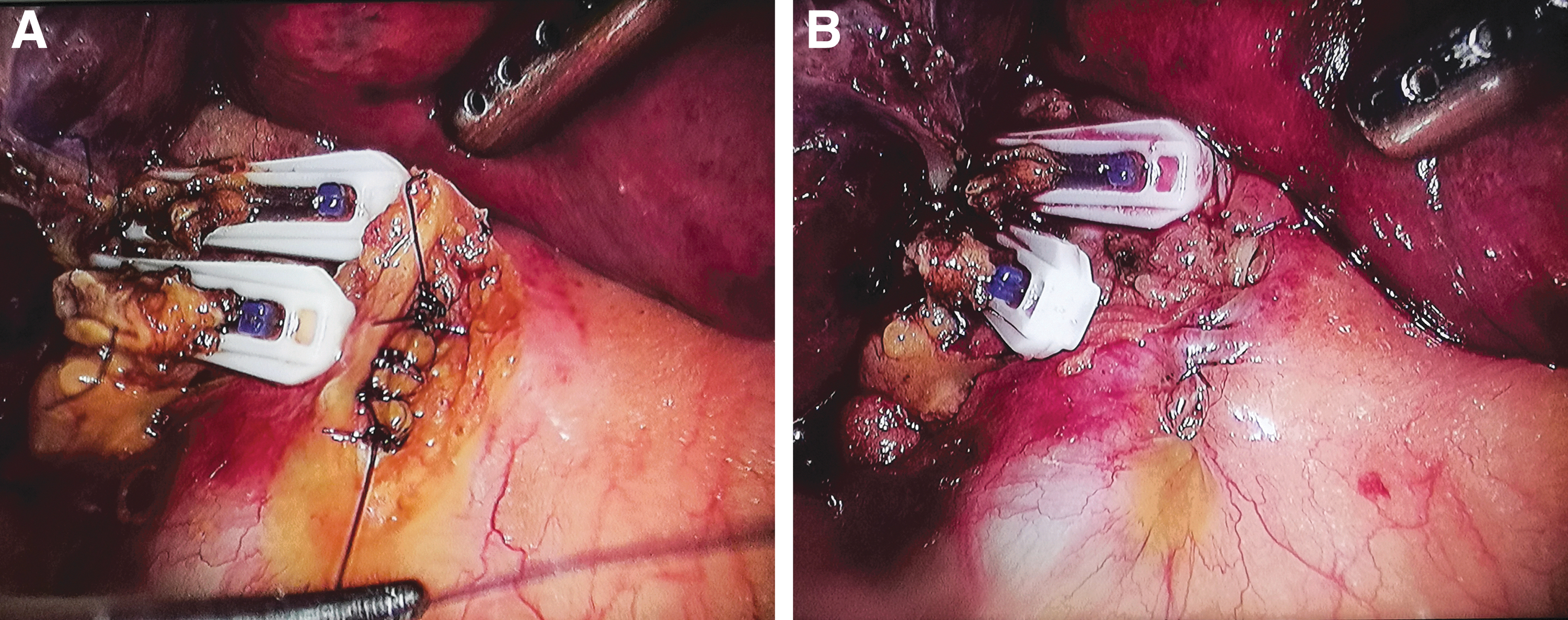
Surgical technique of the two-layered closure of CBD after LCBDE.
Statistical analysis
Statistical Product and Service Solution (SPSS, Version 26.0, IBM Corporation, Armonk, NY) was used for statistical analysis. Continuous variables were expressed as the mean with deviation and compared by using the independent-sample t-test or Mann–Whitney U test. A chi-square test or a Fisher's exact test was performed for categorical variables to calculate frequencies and percentages among the groups. P < .05 was considered statistically significant.
Results
LCBDE was performed in a total of 81 patients: 41 with primary two-layered closure and 40 with traditional primary closure. There were no significant differences between the two groups in terms of demographic characteristics, serum bilirubin level, CBD diameter, number of stones, or maximum diameter of stones (Table 1).
Demographic Data of Enrolled Patients
CBD, common bile duct.
The perioperative outcomes of the two groups are shown in Table 2. The operative time, estimated blood loss, peritoneal drainage of the second and third days, time to drain removal, and postoperative stay duration were not significantly different between the two groups. However, on the first day, the peritoneal drainage was lower in the primary two-layered closure group (P < .05).
Perioperative Outcomes in the Two Groups
No patients in the primary two-layered closure group experienced a bile leakage, whereas 5 patients experienced postoperative bile leakage in the traditional primary closure group. The rate of postoperative bile leakage in the primary two-layered closure group was lower than that in the traditional primary closure group (P < .05). Most of the patients recovered with conservative treatment, except for 1 patient in the traditional primary closure group who received endoscopic nasobiliary drainage. In addition, 2 patients in the primary two-layered closure group and one in the traditional primary closure group had a serum amylase level of more than 200 IU/L with no abdominal pain or distension, which normalized within 2 days. The median follow-up period was 10 months (range, 6–18 months); 1 patient in the traditional primary closure group had recurrence of CBD stones, which was treated by endoscopic retrograde cholangiopancreatography. During the follow-up period, bile duct stricture did not occur in either group, and there was no difference in the incidence of overall complications between the two groups (Table 3).
Postoperative Complications in the Two Groups
Fisher's exact test.
Discussion
Choledocholithiasis is a common disease and it is the main cause of obstructive jaundice and cholangitis. According to the literature, 10%–18% of patients with cholecystolithiasis experience a choledocholithiasis complication. 4 With the progress of minimally invasive laparoscopic techniques, LCBDE has gradually become one of the most common surgical procedures in the treatment of choledocholithiasis, with advantages in terms of minimally invasive, low incidence of complications, preservation of sphincter function, and only a one-stage procedure. 5 In the past, LCBDE was customarily followed by a T-tube insertion to prevent postoperative CBD stricture and bile leakage6,7; however, the need for a T-tube insertion is associated with a high risk of complications, such as disturbance of water and electrolyte metabolism, retrograde infection of bile duct, and bile leakage. Moreover, the patients also have a poor quality of life with a T-tube after surgery. It has been reported that T-tube-related morbidity after laparoscopic surgery can reach 15.3%. 8 In recent years, more and more studies have shown that the primary closure of CBD provides better outcomes and may be a safe and feasible alternative to the T-tube placement after LCBDE.9–11 Nevertheless, due to increased pressure in the bile duct caused by the Oddi sphincter edema during the stone extraction and unskilled suturing techniques, including inappropriate suture spacing, loosening of the knots, and laceration of the bile duct, the incidence of bile leakage can reach 16.7%, 12 and postoperative bile leakage remains one of the most important clinical concerns. 13
At present, the ways to reduce postoperative bile leakage after primary closure of the CBD include reducing the pressure of the bile duct and strengthening the incision of the CBD. The former includes internal or external stent drainage,14,15 whereas the latter includes changing the suture mode and covering it with an exogenous adhesive. Zhang et al. 16 used human fibrin sealant to cover the incision of CBD, which played a certain role in reducing the postoperative bile leakage; however, as an exogenous substance, the human fibrin sealant may lead to a risk of local inflammatory reactions and systemic allergic reactions. In this study, we proposed a two-layered suture method of CBD, the theoretical basis of which is as follows: (1) The suture of the CBD wall and serous layer is more in line with the anatomical physiology of the bile duct. (2) The suture of the serous layer of CBD reinforces the weak points of suture in the inner layer of the bile duct. (3) The bile may leak from the suture gap and pinhole with increased pressure of the CBD after surgery. The suture of the serous layer reduces the tension of the incision by pulling the CBD wall to the midline, so the incidence of postoperative bile leakage can be reduced. (4) When suturing the serous layer, the CBD wall is almost not sutured, so there is no increased risk of postoperative bile duct stricture. The results showed that the incidence of postoperative bile leakage was significantly lower in the primary two-layered closure group than that in the traditional primary closure group (P < .05). No significant differences were observed in the operative time, postoperative duration, estimated blood loss, time to drain removal, postoperative acute pancreatitis, stone recurrence, bile duct stricture, and overall complications between the two groups. In addition, the abdominal drainage volume of the primary two-layered closure group was less than that of the traditional primary closure group on the first day, and the difference was statistically significant (P < .05). In the early postoperative period, the pressure of the CBD was increased by the Oddi sphincter edema and deficiency of the gallbladder compensatory function. The bile still seeped from the gaps and pinholes, but the volume of bile leakage was much lower in the primary two-layered closure group due to the enhanced CBD incision. However, with the elongation of postoperative time, the patency of the bile duct recovered with the disappearance of the Oddi sphincter edema, the pressure of the bile duct decreased, and bile leakage from the CBD incision reduced or even disappeared. The difference in abdominal drainage became not significant between the two groups.
Based on the data from literature and our experience, the following points should be considered to successfully perform the operative procedure. (1) When incising the anterior serosa of the Calot's triangle, the incision line should be made close to the gall bladder. In addition, the CBD incision should be made in two layers, and the serous layer should be incised in situ and a straight line to preserve the serosa tissue (Fig. 2). (2) We adopted the experience of Liu et al., 17 and the closuring margin of the CBD wall was controlled within 1.5 mm. In this way, the diameter of CBD was reduced by less than 1 mm and the circumference was reduced by <3 mm. (3) A whole-layered closure should be performed when closing the CBD wall, but it is difficult to accomplish when the patients are concomitant with acute cholangitis and a thickened bile duct wall, especially for young physicians with little experience in suturing. If in such a situation, the suture method in this study does not require a whole-layered closure and just suturing most of the inner CBD wall. A little outer CBD wall can be sutured to strengthen the incision when suturing the serosal layer. It not only increases the safety of surgery but also reduces the requirement of suturing technology, and makes it easier for young physicians to implement.
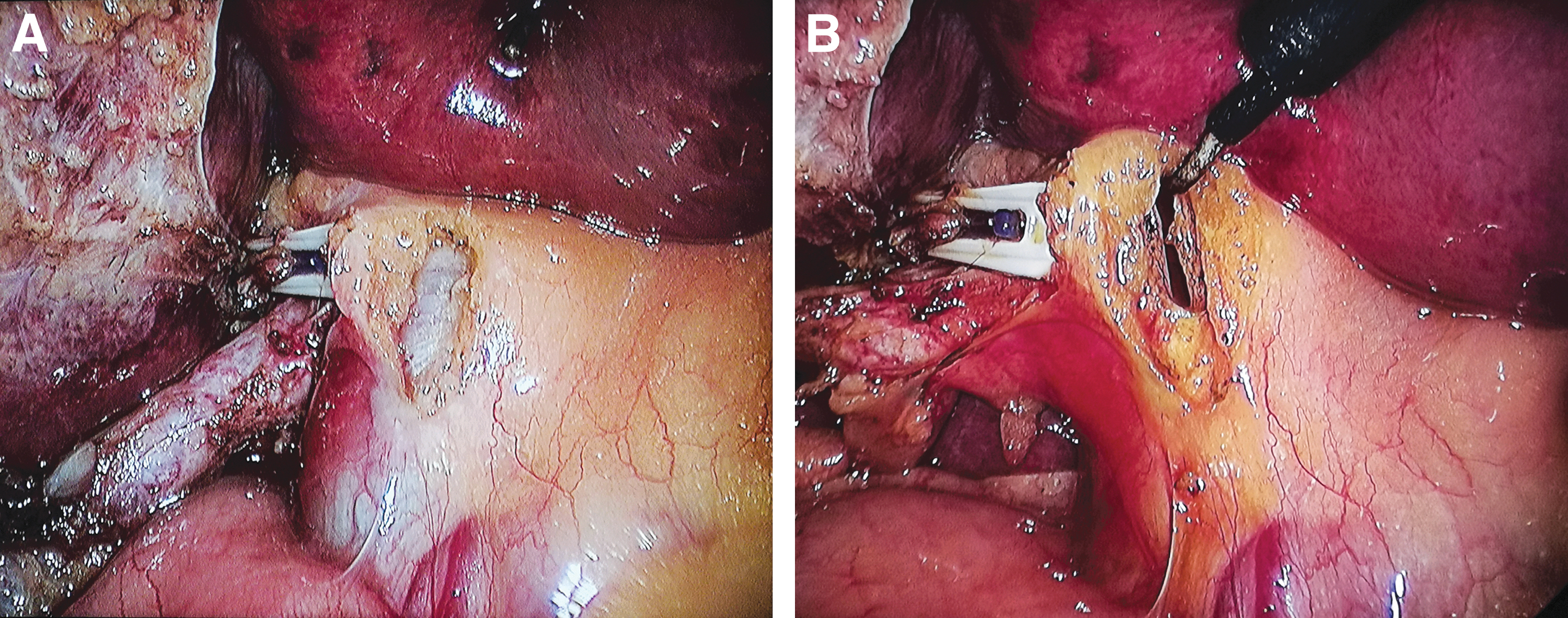
The CBD wall is incised in two layers.
In conclusion, primary closure of CBD has been gradually recognized by surgeons. In this study, we attempted the two-layered closure of CBD after LCBDE, which significantly reduced the incidence of postoperative bile leakage and did not increase the chance of related postoperative complications. Therefore, it is a safe and effective therapeutic option for patients with choledocholithiasis. However, considering the small sample size of this study, further trials with larger cohorts of patients will be needed to verify long-term outcomes of this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The research received no specific grant from any funding agency.