
Abstract
Background:
This study aimed to compare artificial intelligence (AI)-aided colonoscopy with conventional colonoscopy for polyp detection.
Methods:
A systematic literature search was performed in PubMed and Ovid for randomized clinical trials (RCTs) comparing AI-aided colonoscopy with conventional colonoscopy for polyp detection. The last search was performed on July 22, 2020. The primary outcome was polyp detection rate (PDR) and adenoma detection rate (ADR).
Results:
Seven RCTs published between 2019 and 2020 with a total of 5427 individuals were included. When compared with conventional colonoscopy, AI-aided colonoscopy significantly improved PDR (P < .001, odds ratio [OR] = 1.95, 95% confidence interval [CI]: 1.75 to 2.19, I2 = 0%) and ADR (P < .001, OR = 1.72, 95% CI: 1.52 to 1.95, I2 = 33%). Besides, polyps in the AI-aided group were significantly smaller in size than those in conventional group (P = .004, weighted mean difference = −0.48, 95% CI: −0.81 to −0.15, I2 = 0%). In addition, AI-aided group detected significantly less proportion of advanced adenoma (P = .03, OR = 0.70, 95% CI: 0.50 to 0.97, I2 = 46%), pedicle polyps (P < .001, OR = 0.64, 95% CI: 0.49 to 0.83, I2 = 0%), and pedicle adenomas (P < .001, OR = 0.60, 95% CI: 0.44 to 0.80, I2 = 0%).
Conclusion:
AI-aided colonoscopy could significantly increase the PDR and ADR, especially for those with small size. Besides, the shape and pathology recognition of the AI technique should be further improved in the future.
Introduction
With the rapid development of modern technology in recent years, artificial intelligence (AI) technique has been increasingly and widely used in each field, including medicine. 1 Except for the ability to reduce fearless labor, modern AI technique mainly aims to reduce human errors and improve work efficiency. 2 In current clinical use of AI technique, it is mainly applied for the automatic identification of some medicine imaging, including radiology, endoscopy, and pathology to improve the diagnosis accuracy. 3
Colorectal cancer (CRC) has been one of the most common carcinomas worldwide and brought serious threat to human life. 4 Early screening program has been proved as an efficient mean to improve the prognosis of CRC and further reduce social burden. 5 Until now, colonoscopy is still regarded as the most cost-effective and available tool for early screening of CRC. 6 It could help detect polyp, adenoma, and some other precancerous lesions of the bowel mucosa. Besides, colonoscopy could also be used for the surveillance and treatment of some other mucosa disease. 7 In the outpatient service of big centers, the demand for colonoscopy examination is increasing, leading to the subsequent increase in routine work of endoscopists. 8 Under high work pressure, the work efficiency of endoscopists and quality assessment for colonoscopy could be damaged. Besides, some small lesions are difficult to be detected by the human eye even under enlarged and high-resolution imaging. 9 Therefore, it is desperate to develop an AI system for colonoscopy to assist endoscopists.
Recently, an AI-aided system for colonoscopy has been developed in several centers to help endoscopists detect disease. 1 Up to now, several randomized clinical trials (RCTs) have been conducted and published. This study aimed to synthesize the current evidence about AI-aided colonoscopy for polyp detection and find the potential advantages and current shortcomings of AI technique as possible.
Methods
Search strategy
We performed a systematic literature search with no limitation in PubMed and Ovid for studies comparing AI-aided colonoscopy with conventional colonoscopy for detection of polys. The key search terms included (polyp OR adenoma OR neoplasia OR neoplasm OR lesion) AND (colonoscopy) AND (real time OR AI OR computer aided OR automatic detection OR neural network). The last search was performed on July 22, 2020. To avoid literature omission, we also performed a manual search of references of articles and reviews for additional potentially eligible studies. IRB approval is not necessary for this meta-analysis.
Inclusion and exclusion criteria
The inclusion criteria for this meta-analysis were as follows: (1) AI-aided colonoscopy versus conventional colonoscopy, (2) detail outcomes were reported, and (3) RCTs. The exclusion criteria were as follows: (1) review articles, (2) correspondences or editorial, (3) conference abstract without detail data, (4) single-arm study.
Data extraction
Two authors (Y.Z. and X.Z.) reviewed all the identified articles independently. We solved the discrepancies by discussion first and a third reviewer (Z.W.) was consulted if necessary. We extracted the following items from each study: first author's name, year of publication, publication type, study type, number of total patients and male genders, age, history of prior colonoscopy, indication for colonoscopy, and outcomes of interests in each group.
Outcomes of interests
The primary outcomes were polyps detection rate (PDR) and adenoma detection rate (ADR).
The secondary outcomes were the location, size, and shape of polyps and adenoma, and average number of polyps and adenomas detected.
Quality assessment
The quality evaluation was performed by 2 reviewers (Zhang Yuanchuan and Zhang Xubing). The methodological quality of the randomized controlled trials was assessed by modified the Jadad score system. 10
Statistical analysis
All data analyses were conducted using the Review Manager version 5.0 (The Cochrane Collaboration, Software Update, Oxford) and P < .05 was considered statistically significant. Weighted mean difference (WMD) was calculated for the continuous outcomes, and pooled odds ratios (ORs) were calculated for the dichotomous outcomes. For continuous outcomes, if the study only provided means and range values or median and range values, the means and standard deviations were calculated using methods described by Wan et al. 11 Chi-squared test and Higgins I-squared statistic were used for heterogeneity test. A value of P < .05 and I2 > 50% was regarded as existing heterogeneity. If I2 > 50% and P < .05, a random-effects model was applied. Correspondingly, if I2 < 50% and P > .05, a fixed-effects model was applied. Begg's funnel plot was used to evaluate publication bias. Only the results that were reported by three or more studies were included for meta-analysis.
Results
The literature search process and result are shown in Figure 1. The initial search algorithm retrieved 2070 studies in total. After removing duplications, there still remained 1327 studies. After reviewing titles and abstracts, only 34 relevant studies were kept for further evaluation. Besides, no additional record was identified through manual search. Among the 34 studies, 27 studies were excluded for the following reasons: 10 were reviews, 7 were correspondence and editorial, 8 were conference abstracts without detail data, 1 was a single-arm study, and 1 was not randomized trial. Finally, seven articles published between 2019 and 2020 with a total of 5427 individuals (AI-aided group 2702, conventional group 2725) were included in this meta-analysis.12–18
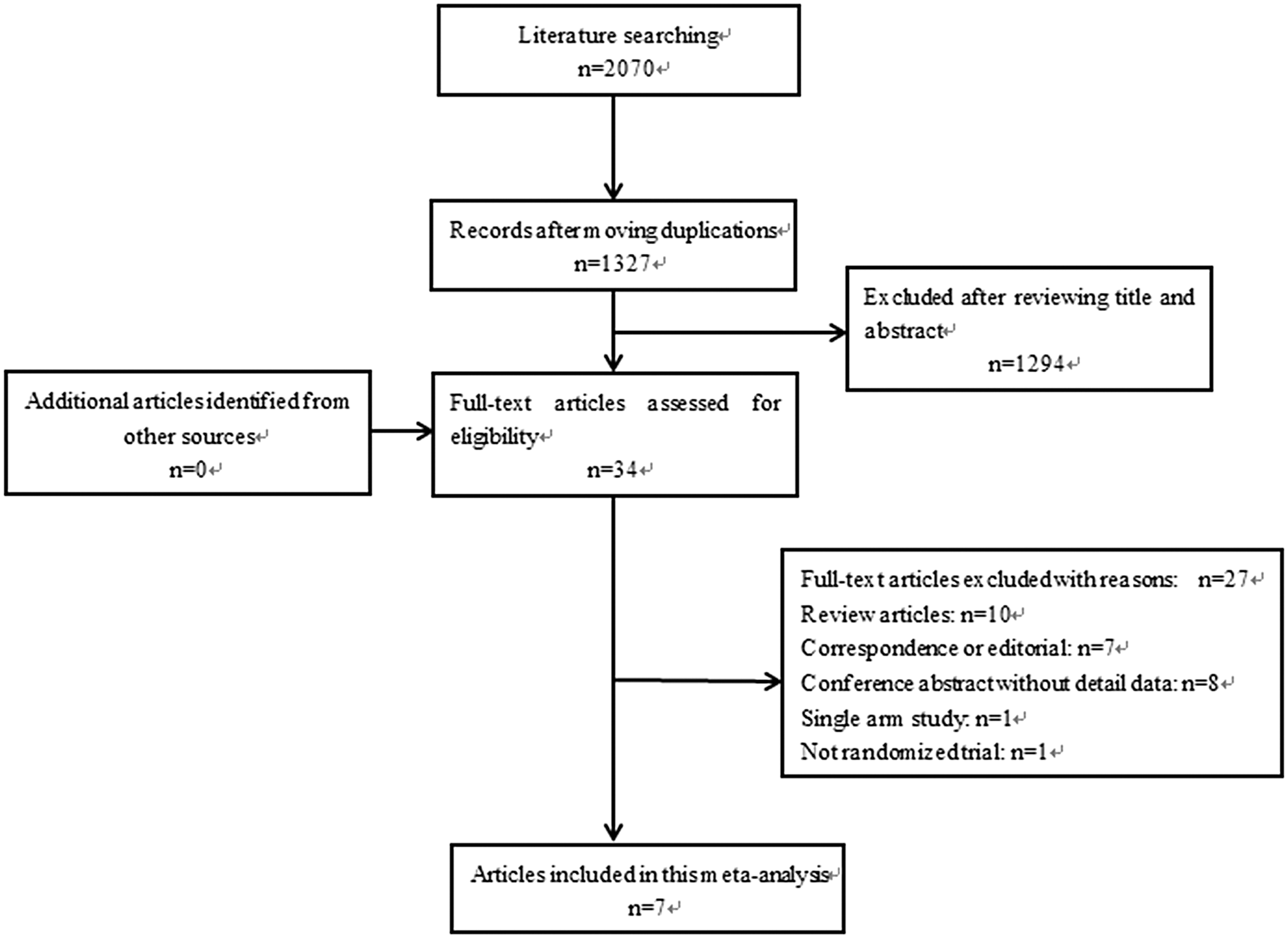
PRISMA flow diagram.
Participants' demographics
The basic information of included studies and participants is given in Table 1. No significant difference was observed between the two groups in terms of age, male gender, body mass index, or indication for colonoscopy.
Participants' Demographics
AI, artificial intelligence; BMI, body mass index; Con, conventional; RCT, randomized clinical trial.
Quality of included studies
The scores of methodological quality assessment of the enrolled studies are given in Table 1. All studies were judged as high quality.
Primary outcomes
We found that AI-aided colonoscopy could achieve significantly higher PDR (P < .001, OR = 1.95, 95% confidence interval [CI]: 1.75 to 2.19, I2 = 0%) and ADR (P < .001, OR = 1.72, 95% CI: 1.52 to 1.95, I2 = 33%) than conventional colonoscopy (Fig. 2).
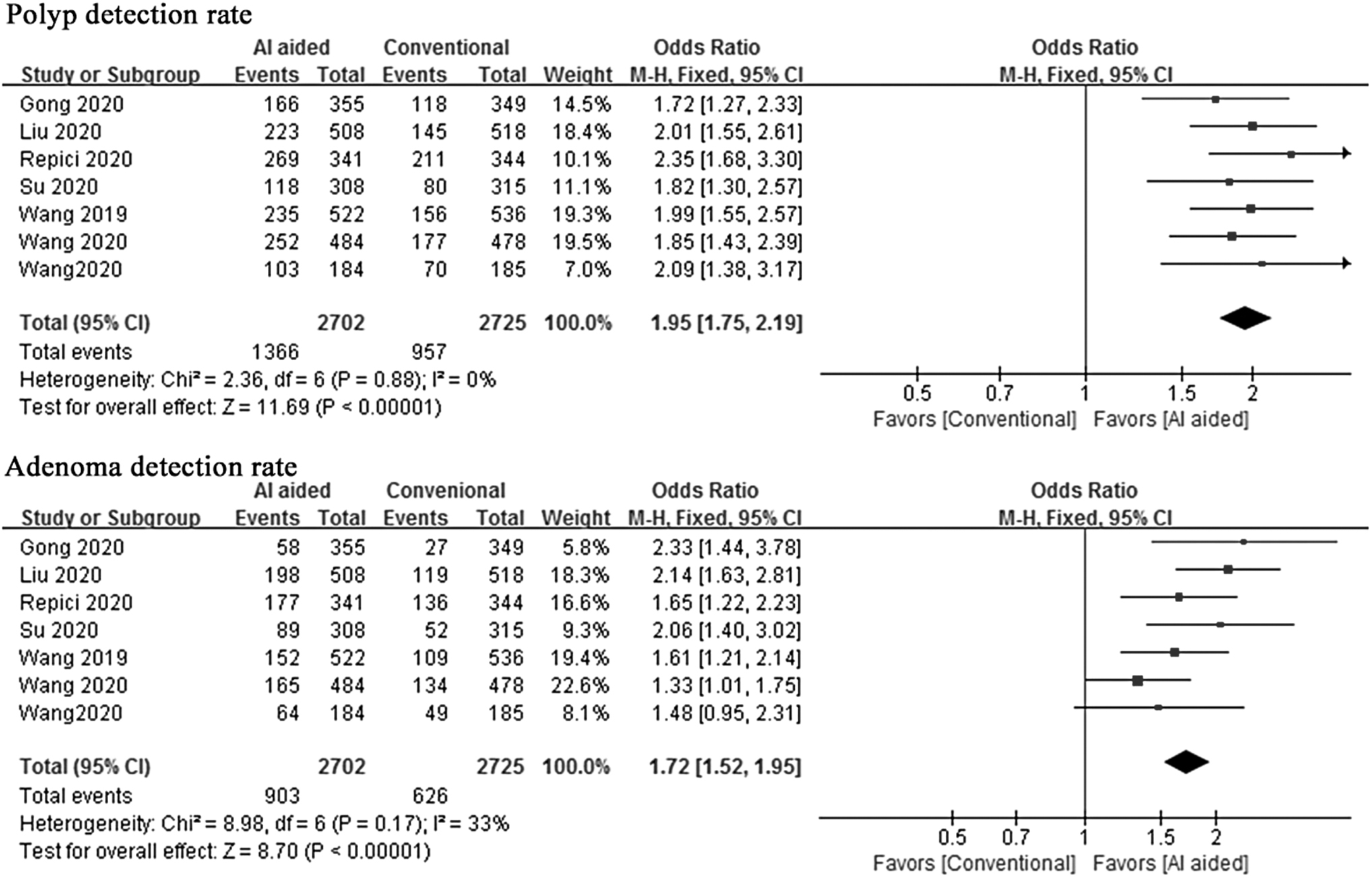
Meta-analysis for PDR and ADR. ADR, adenoma detection rate; AI, artificial intelligence; PDR, polyp detection rate.
Secondary outcomes
According to the pathological outcomes, among all detected polyps, AI-aided colonoscopy could identify significantly more benign disease, which included proliferative, inflammatory, hamartoma, and normal colonic mucosa (P = .009, OR = 1.26, 95% CI: 1.06 to 1.50, I2 = 0%). However, the proportion of advanced adenoma was significantly less in the AI-aided colonoscopy group (P = .03, OR = 0.70, 95% CI: 0.50 to 0.97, I2 = 46%). Besides, the proportion of sessile serrated adenoma/polyp was comparable between the two groups (Table 2).
Meta-Analysis of Secondary Outcomes
AI, artificial intelligence; CI, confidence interval; OR, odds ratio.
As for polyp distribution, the two groups had similar location at cecum (P = 1.00, OR = 1.00, 95% CI: 0.53 to 1.90, I2 = 0%), ascending colon (P = .50, OR = 1.07, 95% CI: 0.87 to 1.32, I2 = 0%), descending colon (P = .15, OR = 1.32, 95% CI: 0.90 to 1.94, I2 = 57%), and sigmoid colon (P = .82, OR = 1.05, 95% CI: 0.72 to 1.51, I2 = 73%). However, AI-aided colonoscopy detected significantly more polyps in transverse colon (P = .03, OR = 1.25, 95% CI: 1.02 to 1.53, I2 = 0%), but less in rectum (P = .03, OR = 0.67, 95% CI: 0.47 to 0.96, I2 = 65%). In addition, AI-aided colonoscopy could identify significantly more flat polyps (P = .08, OR = 1.19, 95% CI: 0.98 to 1.45, I2 = 0%), but less pedicle polyps (P < .001, OR = 0.64, 95% CI: 0.49 to 0.83, I2 = 0%). The two groups had similar proportion of sessile polyps (P = .50, OR = 1.07, 95% CI: 0.88 to 1.29, I2 = 43%). We also observed that polyps in the AI-aided colonoscopy group were significantly smaller in size than those in conventional group (P = .004, WMD = −0.48, 95% CI: −0.81 to −0.15, I2 = 0%). Besides, the AI-aided colonoscopy group had significantly more diminutive (0–5 mm, P < .001, OR = 1.42, 95% CI: 1.18 to 1.72, I2 = 26%) and small polyps (6–10 mm, P < .001, OR = 0.67, 95% CI: 0.54 to 0.83, I2 = 0%) (Table 2).
When it came to the separate analysis for adenoma detection, we found no significant difference between the two groups for adenoma distribution, regardless of cecum (P = .98, OR = 1.01, 95% CI: 0.46 to 2.23, I2 = 0%), ascending colon (P = .09, OR = 0.80, 95% CI: 0.62 to 1.04, I2 = 10%), transverse colon (P = .13, OR = 1.21, 95% CI: 0.94 to 1.55, I2 = 0%), descending colon (P = .29, OR = 1.17, 95% CI: 0.88 to 1.56, I2 = 0%), sigmoid colon (P = .84, OR = 0.97, 95% CI: 0.75 to 1.26, I2 = 0%), or rectum (P = .53, OR = 0.90, 95% CI: 0.66 to 1.24, I2 = 0%). As for adenoma shape, the two groups had similar proportion of flat (P = .13, OR = 1.23, 95% CI: 0.94 to 1.60, I2 = 0%) and sessile polyps (P = .15, OR = 1.20, 95% CI: 0.94 to 1.54, I2 = 0%), but AI-aided colonoscopy detected significantly less pedicle adenoma when compared with conventional colonoscopy (P < .001, OR = 0.60, 95% CI: 0.44 to 0.80, I2 = 0%). In addition, adenoma size was not significantly different between the two groups (P = .26, WMD = −0.22, 95% CI: −0.59 to 0.16, I2 = 0%). AI-aided colonoscopy detected comparable number of diminutive (0–5 mm, P = .22, OR = 1.14, 95% CI: 0.93 to 1.39, I2 = 0%), small (6–10 mm, P = .12, OR = 0.83, 95% CI: 0.66 to 1.05, I2 = 27%), and large adenoma (>10 mm, P = .80, OR = 1.05, 95% CI: 0.73 to 1.52, I2 = 0%) (Table 2).
We also found that average number of both polyps (P < .001, OR = 11.43, 95% CI: 2.75 to 47.53, I2 = 97%) and adenomas (P < .001, OR = 2.35, 95% CI: 2.09 to 2.63, I2 = 28%) detected in the AI-aided colonoscopy group was significantly more than that in the conventional colonoscopy group (Table 2).
Publication bias
A funnel plot of the studies reporting on PDR shows that there was no obvious publication bias among the studies (Fig. 3).

Funnel plot based on PDR. PDR, polyp detection rate.
Discussion
AI-aided technique for colonoscopy has rapidly risen in recent years. 19 In several centers, AI-aided colonoscopy has been well developed for clinical use. 20 In consideration that several RCTs have been conducted to compare AI-aided colonoscopy with conventional colonoscopy for polyp detection, we performed this meta-analysis to synthesize the current relevant evidence, hoping to find the advantages, or, perhaps the potential shortcomings of AI-aided colonoscopy. In this study, seven RCTs with a total of 5427 individuals were included. Similar to previous studies, 21 we found AI-aided colonoscopy could significantly improve the polyps and ADR when compared with conventional colonoscopy. It has particular advantages for detecting lesions with smaller size. However, AI-aided colonoscopy should be further perfected in terms of different shape and pathology recognition.
Colorectal polyps, especially adenomas, are recognized as the precancerous lesions of CRC. 22 Early screening program aims to find these lesions as much as possible, for the early intervention and preventing CRC incidence. 23 So, we can see, in most clinical trials, PDR or ADR was regarded as an importance parameter. 20 In this study, both PDR and ADR were significantly improved in the AI-aided colonoscopy group, demonstrating the huge role of the AI technique. In addition to the quality of bowel preparation and mucosa disease, the detection rate of bowel lesions could be related to the learning curve of endoscopists. 24 However, even experienced doctors can also miss some lesions, especially for those with small size and flat shape. As we all know, the malignant transformation rate of polyps and adenoma is associated with size and shape. Doubtlessly, the risk for canceration would increase with the size of polyps and adenoma. 25 Previous studies also demonstrated that sessile polyps or adenomas have higher risk for cancer formation than pedicle lesions. 26 Fortunately, except the improved PDR and ADR, we also observed that the AI technique could help find significantly more small lesions, which perhaps cannot be totally found under conventional colonoscopy with human eye. Potentially, not all these small lesions were up to the criteria for clinical treatment, but no one can assure these would not generate tumor in the future. Actually, these positive detections could change the surveillance strategy for individuals. In the included studies, patients with history of inflammatory bowel disease, CRC, and some other diseases were excluded. We thought this might be because these diseases could influence the probability for positive finding. The consistency of indication for colonoscopy between the two groups could also contribute to the favorable outcomes.
Before the development of the AI detection system, computer must experience the process of machine learning. 27 In the detected polyps and adenomas, the proportion of different shape was not consistent between the two groups. This might be related to the sample chosen for training set. Besides, we thought this might be because pedicle polyps and adenomas are easier to be identified by the human eye, since less proportion of both pedicle polyps and adenomas was detected by AI-aided colonoscopy. This could be further explored in the future. Except automatic detection, some centers have begun to explore the real-time pathological diagnosis with AI-aided colonoscopy. 28 This would influence the treatment strategy during colonoscopy, and further reduce the burden of pathologists because some biopsy would be avoided. We believe this is achievable in the near future, but now it is still not fully mature. We could see the pathological classification was not balanced between the two groups and the AI-aided group had significantly less proportion of advanced disease. On the one hand, generally, advanced lesions would have a larger size and are easy to be detected by the human eye. On the other hand, AI-aided colonoscopy detected significantly more lesions with smaller size, which had lower risk for advanced disease. We also think that we can divide the development of AI technique for colonoscopy into two steps: the first step is automatic detection and the second step is pathological diagnosis. Although the automatic detection system has been developed for clinical use, it was not widely popularized and still had some defects to be further perfected.
The strengths of this study should be highlighted. First, all included studies were RCTs. Second, we have included more studies than previous meta-analysis. The limitation of this study is that high heterogeneity was observed in some outcomes. Although we performed sensitivity analysis by removing one study each time, the outcomes remained unchanged. We thought this could be related to the learning curve of endoscopists, heterogeneity from the inner of AI system, and some other factors.
In conclusion, AI-aided colonoscopy could significantly increase the PDR and ADR, especially for those with small size. Besides, the shape and pathology recognition of the AI technique should be further improved in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by 1•3•5 project for disciplines of excellence—Clinical Research Incubation Project, West China Hospital, Sichuan University (No. 2019HXFH031)