
Abstract
Background:
To compare the safety and effectiveness of endoscopic ultrasound-guided gallbladder drainage (EUSGBD) with percutaneous transhepatic gallbladder drainage (PTGBD) for acute cholecystitis with high surgical risk.
Methods:
An electronic search was performed of the major databases, namely PubMed, Embase, Web of Science, the Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov until July 1, 2020. Studies comparing EUSGBD with PTGBD were included.
Results:
We identified 8 studies involving 801 patients, and patients were divided into two groups (EUSGBD group = 338 and PTGBD = 463). EUSGBD was associated with less reintervention (odds ratio [OR] = 0.15; 95% confidence interval [CI]: 0.07–0.32; P < .00001) and readmission (OR = 0.24; 95% CI: 0.08–0.67; P = 7). With lumen-apposing metal stents (LAMS), EUSGBD was associated with fewer adverse events (OR = 0.35; 95% CI: 0.13–0.93; P = .03), recurrent cholecystitis (OR = 0.27; 95% CI: 0.10–0.71; P = .008) and readmission (OR = 0.10; 95% CI: 0.03–0.32; P = .0001). There were no significant differences between the groups regarding clinical success (OR = 1.47; 95% CI: 0.75–2.90; P = .26). Technical success with PTGBD was higher than that with EUSGBD (OR = 0.32; 95% CI: 0.13–0.83; P = .02).
Conclusions:
EUSGBD was comparable with PTGBD regarding clinical success, with less reintervention and readmission, for acute cholecystitis with high surgical risk. The cholecystitis recurrence rate was lower with EUSGBD with LAMS.
Introduction
Acute cholecystitis is one of the most common conditions seen in the emergency department. 1 Several serious complications, namely gangrene, perforation, and septic shock may occur if acute cholecystitis is untreated.2–4 Early laparoscopic cholecystectomy (LC) has been confirmed as the standard treatment for acute cholecystitis. Including several guidelines, previous studies recommended that early LC has more benefit than delayed LC.5,6 However, some patients with moderate or severe acute cholecystitis are not suitable for surgery because of comorbidities, serious status, or because they are receiving anticoagulants. Gallbladder drainage is necessary to resolve the gallbladder inflammation in patients with a high surgical risk, and several procedures for gallbladder drainage have been proposed. Percutaneous transhepatic gallbladder drainage (PTGBD), a minimally invasive technique, is the traditional first-line treatment for gallbladder drainage. 7 However, PTGBD may be associated with several complications such as catheter dislodgment and occlusion, bile leak, and the need for reintervention. In addition, this technique may not be suitable for patients with ascites, coagulopathy, and those at high risk of removing the tube themselves.8,9
With developments in endoscopy, endoscopic ultrasound-guided gallbladder drainage (EUSGBD) was reported in 2007 and was rapidly and widely implemented.10,11 Several articles have reported the clinical outcomes of EUSGBD for gallbladder drainage.12–14 EUSGBD is currently being performed more often as an alternative to PTGBD. As described in the Tokyo Guidelines, EUSGBD is an acceptable method in high-volume medical centers. 7 Nevertheless, complications such as perforation and stent migration can occur in EUSGBD. Several studies compared EUSGBD and PTGBD and revealed inconsistent results.15,16 With the use and continuous development of lumen-apposing metal stents (LAMS), comparisons between EUSGBD and PTBGD have changed. It is important to note that the sample sizes in previous comparative studies were small, and that several new studies have been published. Recently, an international multicenter randomized controlled superiority trial (DRAC 1) revealed the 1-year results comparing EUSGBD and PTBGD. 17 Thus, we conducted a meta-analysis and systematic review to compare the efficacy and safety of EUSGBD and PTGBD for acute cholecystitis with high surgical risk.
Methods
Literature search
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement. 18 We systematically searched the literature in the major databases of PubMed, Embase, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), and ClinicalTrials.gov to July 1, 2020. The following English free text and medical subject heading terms were applied: “endoscopic ultrasound gallbladder drainage,” “percutaneous transhepatic gallbladder drainage,” “cholecystogastrostomy,” “cholecystoduodenostomy,” “percutaneous cholecystostomy,” and “acute cholecystitis.” The search was restricted to human subjects and English-language articles. References from the initial articles were checked manually for further analysis, and disagreements between the authors were resolved by consensus.
Institutional Review Board approval is not applicable for this study.
Inclusion and exclusion criteria
The studies had to meet the following criteria: (1) only studies comparing EUSGBD with PTGBD for acute cholecystitis were included in this study. (2) Studies including data and details for technical success, clinical success, adverse events, recurrent cholecystitis, reintervention, and readmission were included. The exclusion criteria were as follows: (1) articles published in languages other than English; (2) case reports, reviews, guidelines, and letters; and (3) studies without adequate outcomes, and nonhuman studies.
Outcome measures
The primary outcomes were technical success, clinical success, and adverse events. The secondary outcomes were recurrent cholecystitis, reintervention, readmission, and hospital stay. The definitions of technical success and clinical success were according to the original studies. Subgroup analysis was conducted for studies using LAMS in EUSGBD versus PTGBD. There were few studies that compared fully covered self-expandable metal stent (FCSEMS) with PTGBD. Therefore, we did not perform a subgroup analysis of FCSEMS.
Data extraction
Two independent authors applied the inclusion and exclusion criteria to identify potential studies for inclusion. The following study details were selected: the first author, year of publication, type of study, country in which the study took place, sample size, gender, age, and the definition of technical success and clinical success. Attempts were made to contact the study authors if data were not available or not interpretable. Conflicts in data abstraction were resolved by consensus and by referring to the original article.
Risk of bias assessment
The Newcastle–Ottawa scale (NOS) was used to evaluate the quality of nonrandomized studies. NOS scores range from 0 to 9, and studies with scores >6 were deemed to have qualified. 19 The randomized controlled trial (RCT) quality was assessed using the Jadad scale, 20 and studies with a score ≥4 were defined as high-quality studies.
Statistical analysis
All statistical analyses were performed using Review Manager (RevMan) version 5.3 software (Cochrane Informatics and Knowledge Management Department, Nordic Cochrane Centre, Copenhagen, Denmark). Odds ratios (ORs) and the weighted mean difference with 95% confidence intervals (CIs) were used for dichotomous outcomes and continuous outcomes, respectively. Heterogeneity among studies was evaluated by the χ 2 test, and a two-tailed P value <.05 was considered statistically significant. We also assessed the potential for publication bias through a visual inspection of funnel plot asymmetry.
Results
Study selection and trial characteristics
A total of 279 studies were selected after the initial search of the online databases using the search criteria. After removing duplicate studies, 78 studies remained. We excluded 71 studies for various reasons by reviewing the title, abstract, and full text. Finally, eight studies (six retrospective studies and two RCT) were suitable for inclusion in this study.9,12–14,17,21–23 Figure 1 illustrates the PRISMA flowchart of the literature search strategy, and Table 1 describes the baseline characteristics of the included articles. A total of 722 patients were divided into EUSGBD and PTGBD groups. The drainage methods for EUSGBD were as follows: four studies used LAMS; one used fully covered self-expandable metal stent (FCSEMS); one used endoscopic nasobiliary drainage (ENBD); one used a mixture of LAMS, FCSEMS, and plastic stents; and the method was not reported in one study. The definitions of technical success and clinical success in the included studies are shown in Table 2.
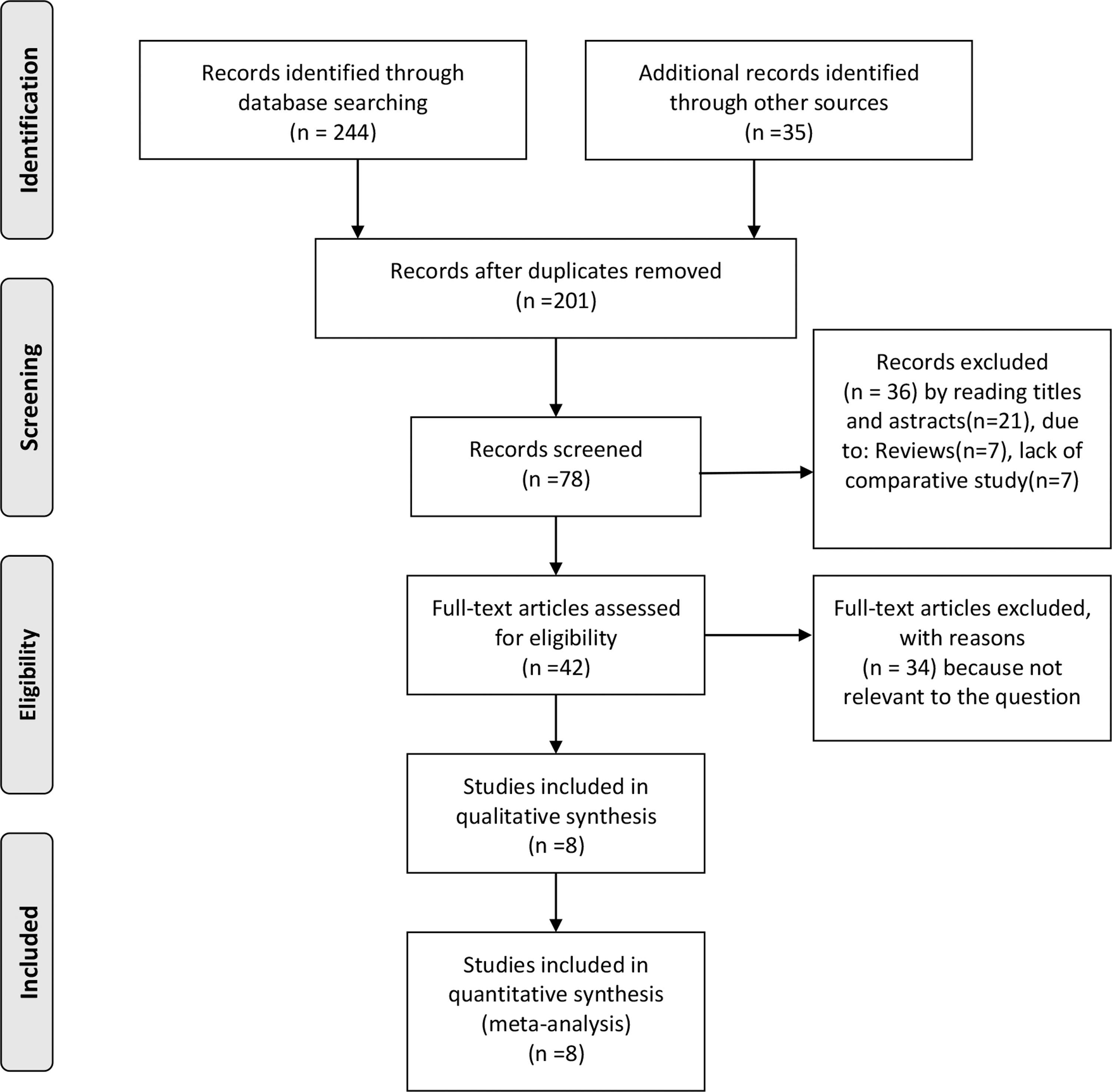
Flow diagram of the published articles evaluated for inclusion in this meta-analysis.
The Characteristics of Included Studies
Report as range (min, max).
Jadad score.
E, endoscopic ultrasound-guided gallbladder drainage (EUSGBD); ENBD, endoscopic nasobiliary drainage; FCSEMS, fully covered self-expandable metal stent; LAMS, lumen-apposing metal stents; NA, not available; NOS, Newcastle–Ottawa scale; P, percutaneous gallbladder drainage (PTGBD); RCT, randomized controlled trial; Retro, retrospective studies; SD, standard deviation.
The Definition of Technical Success and Clinical Success
EUSGBD, endoscopic ultrasound-guided gallbladder drainage; LAMS, lumen-apposing metal stents; NA, not available; PTGBD, percutaneous gallbladder drainage.
The primary outcomes
Technical success
All eight studies reported data for technical success. The incidence of technical success in the PTGBD group (458/463 patients) was higher than that in the EUSGBD group (325/338 patients) (OR = 0.32; 95% CI: 0.13–0.83; P = .02; I2 = 0%) (Fig. 2a). A subgroup meta-analysis showed that the incidence of technical success in the EUSGBD (LAMS) group was lower than that with PTGBD (OR = 0.30; 95 CI%: 0.10–0.92; P = .04; I2 = 0%) (Fig. 4a).
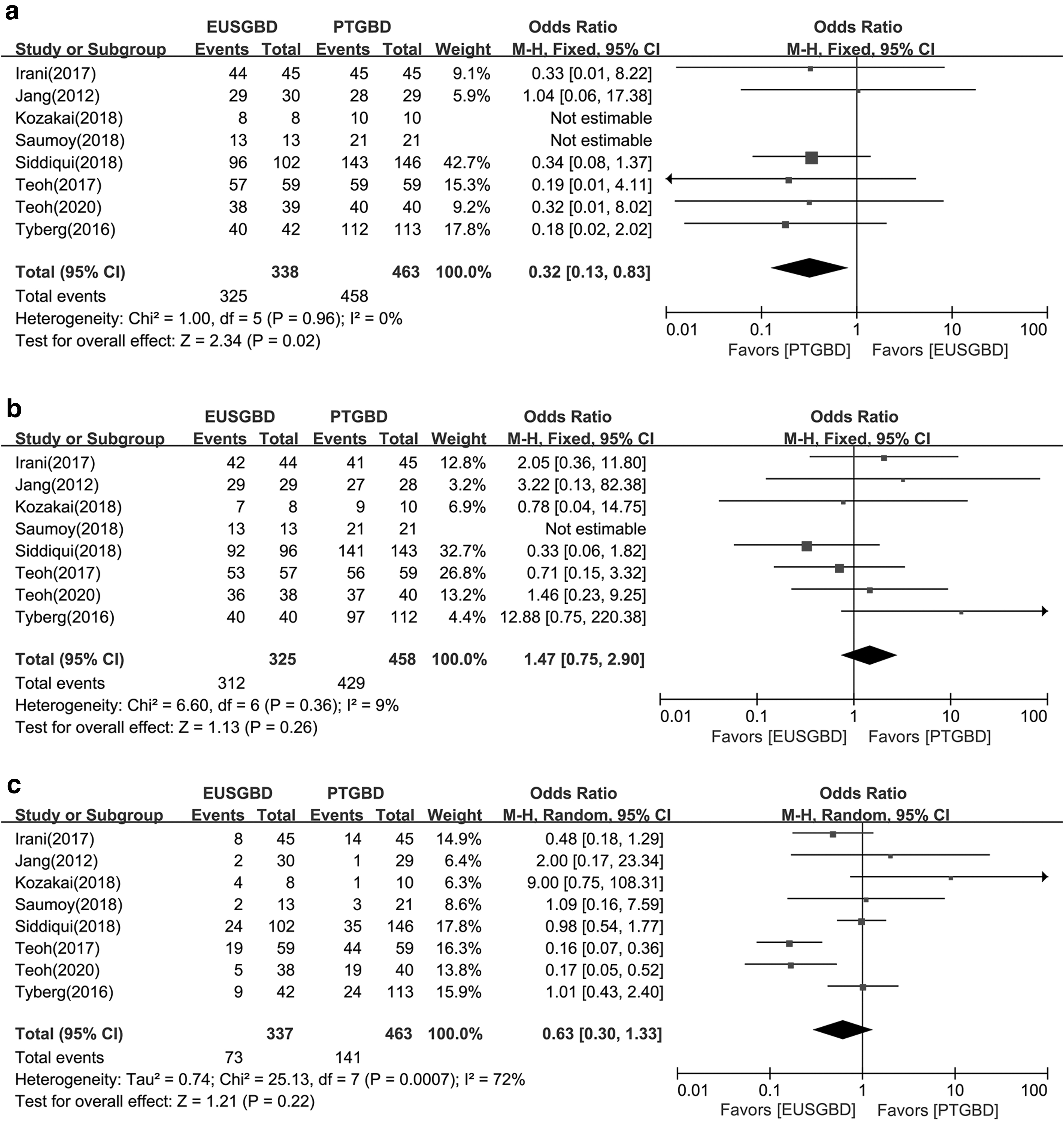
Forest plot of the meta-analysis comparing EUSGBD and PTGBD
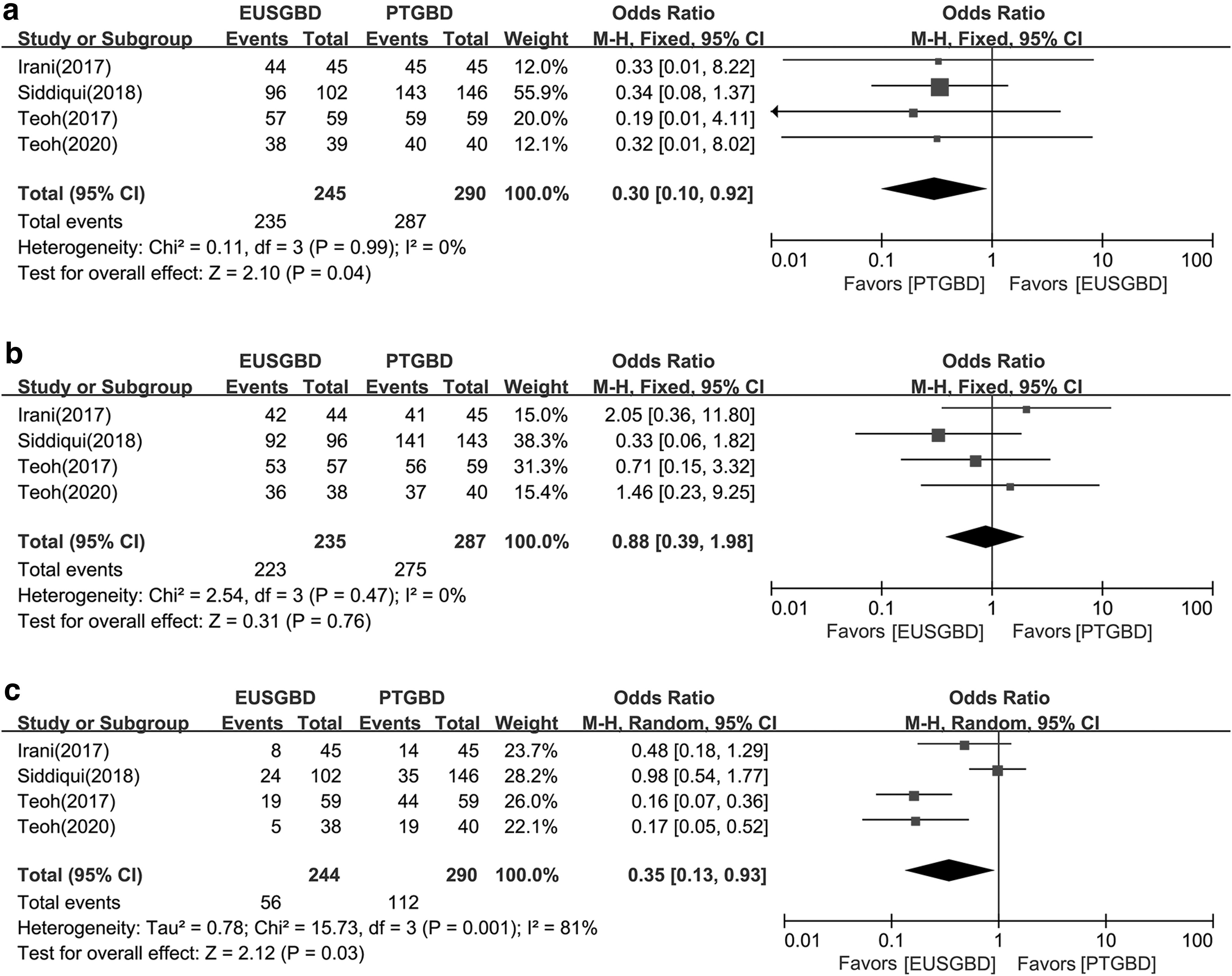
Forest plot of the meta-analysis comparing EUSGBD with LAMS and PTGBD
Clinical success
A total of 783 patients achieved clinical success (312/325 with EUSGBD and 428/458 with PTGBD). Pooled analysis showed no significant difference between the groups (OR = 1.47; 95% CI: 0.75–2.90; P = .26; I2 = 9%) (Fig. 2b). Similar results were seen in the subgroup analysis of EUSGBD (LAMS) versus PTGBD (OR = 0.88; 95% CI: 0.39–1.98; P = .76; I2 = 0%) (Fig. 4b).
Adverse events
Adverse events were reported in all eight studies; however, there was no significant difference between EUSGBD and PTGBD (OR = 0.63; 95% CI: 0.30–1.33; P = .22; I2 = 72%) (Fig. 2c). EUSGBD with LAMS was associated with fewer adverse events than in the PTGBD group (OR = 0.35; 95% CI: 0.13–0.93; P = .03; I2 = 81%) (Fig. 4c).
The secondary outcomes
Recurrent cholecystitis
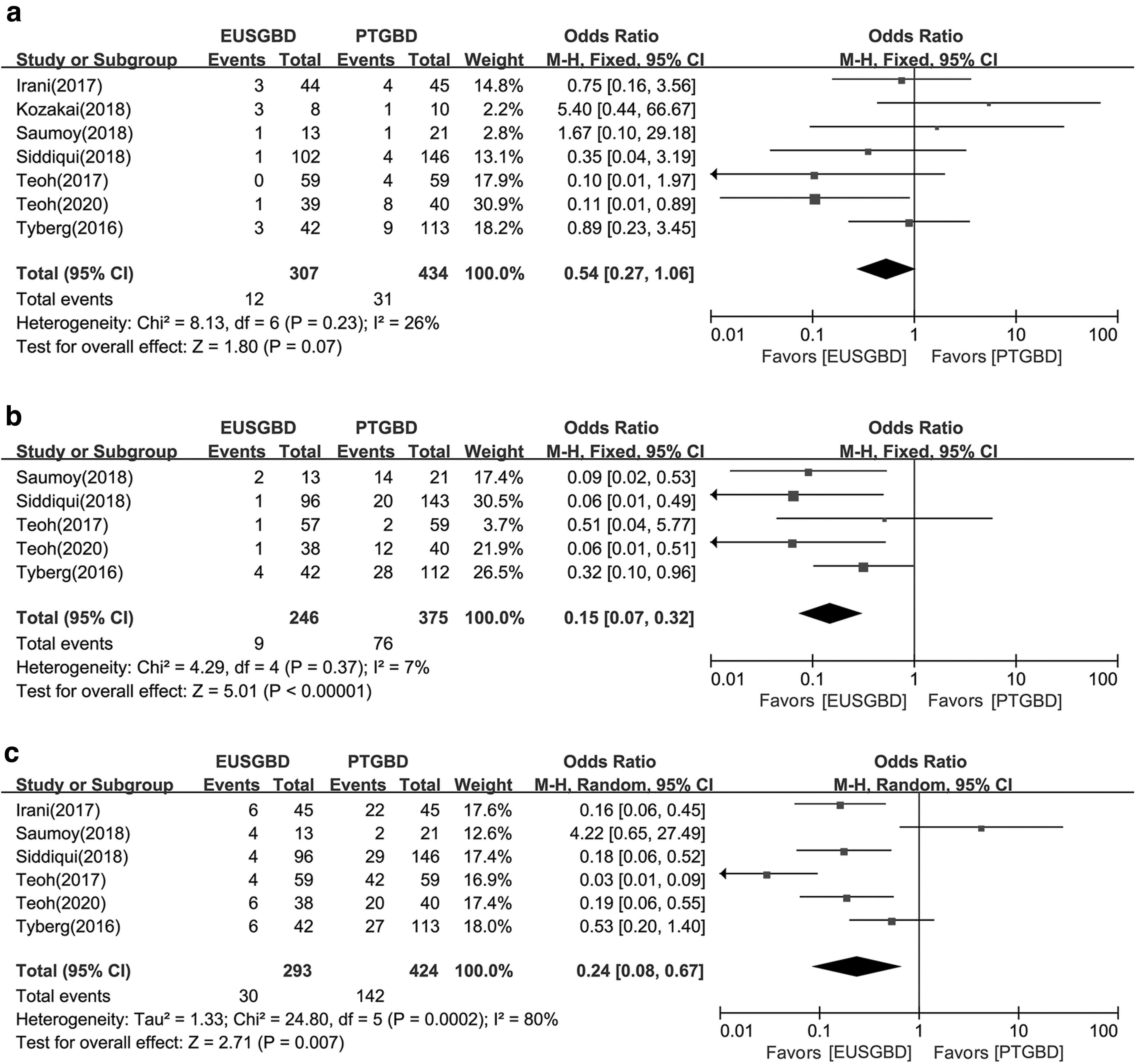
The incidence of recurrent cholecystitis was similar with EUSGBD and PTGBD in all studies (OR = 0.07; 95% CI: 0.27–1.06; P = .41; I2 = 26%) (Fig. 3a); however, EUSGBD with LAMS was associated with less recurrent cholecystitis (OR = 0.27; 95% CI: 0.10–0.71; P = .008; I2 = 0%) (Fig. 5a).
Forest plot of the meta-analysis comparing EUSGBD and PTGBD

Forest plot of the meta-analysis comparing EUSGBD with LAMS and PTGBD
Reintervention
Four studies reported data for reintervention rates. Pooled analysis showed that the incidence of reintervention in the PTGBD group was higher than that in the EUSGBD group (OR = 0.15; 95% CI: 0.07–0.32; P < .00001; I2 = 7%) (Fig. 3b). In studies using EUSGBD (LAMS), the incidence of reintervention was lower than with PTGBD (OR = 0.09; 95% CI: 0.03–0.31; P = .0001; I2 = 6%) (Fig. 5b).
Readmission
Five studies reported data for readmission related to the procedure. Readmission was less common in the EUSGBD group (30/293) than in the PTGBD group (142/424) (OR = 0.24; 95% CI: 0.08–0.67; P = 7; I2 = 80%) (Fig. 3c). Similar result showed in subgroup analysis between EUSGBD (LAMS) and PTGBD (OR = 0.10; 95% CI: 0.03–0.32; P = .0001; I2 = 70%) (Fig. 5c).
Sensitivity analysis
The influence of a single study on the overall meta-analysis estimate was investigated by omitting one study at a time. The omission of any study resulted in no significant difference, indicating that our results were statistically reliable.
Publication bias
Most graphical funnel plots of the parameters were symmetrical.
Discussion
Our results showed that EUSGBD was associated with less reintervention and readmission, and shorter hospital stays. EUSGBD was comparable with PTGBD regarding clinical success, adverse events, and recurrent cholecystitis. However, the technical success rate was higher with PTGBD. Given the limitations of our study, high-quality RCTs are required in future.
For patients with high surgical risk, PTGBD is widely accepted as the first-line approach for gallbladder drainage for acute cholecystitis. 24 Previous studies have confirmed the efficacy of PTGBD, with technical success rates with PTGBD and EUSGBD reported in previous studies ranging from 98% to 99% and 91.5% to 100%, respectively.12,13,25,26 Debate continues regarding comparing the technical success rates between the two approaches. In the present meta-analysis, the technical success in the PTGBD group was slightly higher than that in the EUSGBD group. This is may be related to the fact that EUSGBD is more technically challenging; EUSGBD requires both endoscopy and endoscopic ultrasonography. Alternatively, the differences in our study may be associated with the smaller sample size in the EUSGBD group. The subgroup analysis showed that with LAMS, EUSGBD had a slightly lower technical success rate compared with PTGBD. The study conducted by Tyberg et al. used LAMS, FCSEMS, and plastic stents for EUSGBD; however, we excluded this study from the subgroup analysis. A comparative meta-analysis conducted by Mohan et al. published in 2019 showed that PTGBD was superior to EUSGBD regarding technical success; however, the study included case report series. Another studied published in 2018 comparing EUSGBD versus PTGBD showed that there were no significant differences regarding the technical success rate (OR = 2.3; 95% CI: 0.7–7.5; P = .18). Compared with some previous studies, one strength of our meta-analysis is that we included recently published studies. As EUSGBD becomes more widely used, the technical success rate will continue to change. It is worth noting that the definition of technical success varied in the included studies.
This meta-analysis confirmed that EUSGBD was comparable with PTGBD regarding clinical success (OR = 1.48, I2 = 24%). Several studies have compared clinical success rates between the two methods. The study by Tyberg et al. revealed that EUSGBD had a higher clinical success versus PTGBD (100% versus 86.61%, respectively). 13 In contrast, a study comparing EUSGBD, endoscopic transpapillary gallbladder drainage (ETGBD), and PTGBD showed that PTGBD was associated with higher clinical success rates than EUSGBD (97% versus 90%, respectively). With developments in EUSGBD, metal stents are now widely used; LAMS have been widely accepted and could increase the clinical success rate. In our study, the subgroup analysis showed that EUSGBD with LAMS had comparable clinical success to PTGBD, which confirmed the efficacy of stents in EUSGBD. Compared with plastic stents, LAMS have a larger diameter, which is beneficial for gallbladder drainage.
The definition of clinical success varied in the included studies, which contributed substantial heterogeneity. Table 2 summarizes the definition of clinical success in the included studies. Larger studies using a uniform definition of clinical success are needed.
In this study, we showed that the rate of recurrent cholecystitis was comparable between EUSGBD and PTGBD in all studies. Interestingly, the subgroup analysis showed that the LAMS group had significantly less cholecystitis recurrence than the PTGBD group. We hypothesize that this difference may be related to the design of the LAMS. Recently, LAMS have been used for pancreatic fluid collection drainage 27 and biliary drainage, 28 and LAMS have several advantages over other metal and plastic stents. 26 LAMS have a large diameter, which not only ensures smooth bile drainage, but also permits stone removal through the LAMS, endoscopically. Using LAMS could help reduce bile leaks; the occurrence of anastomotic leak after successful placement of a LAMS for acute cholecystitis is exceedingly rare. 17 However, there is still a lack of high-quality studies comparing LAMS and other metal or plastic stents.
Regarding adverse events, EUSGBD and PTGBD were comparable, in our study. Including catheter dysfunction, pain, and bile leaks, the adverse events rate in the PTGBD group ranged from 4% to 51%. These events could lead to procedure-related reintervention and readmission. Our study confirmed that PTGBD was associated with higher reintervention and readmission rates compared with EUSGBD. Furthermore, the subtypes of adverse events after PTGBD and EUSGBD differ; EUSGBD may be associated with more bleeding and perforation, and PTGBD may be associated with more stent-related complications. 29 However, few studies have evaluated the long-term outcomes of EUSGBD and PTGBD. The DRAC 1 study compared the 1-year adverse events rate and showed that EUSGBD had a lower adverse events rate compared with PTGBD. 17 Saumoy et al. showed that cholecystectomy after EUSGBD was safe and feasible for the management of cholecystitis. 22 In this study, there were insufficient data reported in the included studies to evaluate long-term outcomes.
There are several limitations in this study. First, most of the included studies were retrospective; only one study was an RCT, and the study had a small sample size. In addition, retrospective studies could lead to selection bias. Second, the baseline characteristics of the enrolled patients may have contributed to heterogeneity, and the degree, if any, is unknown. Third, the definitions of the outcome measures varied. More high-quality RCTs are required.
Conclusion
EUSGBD was comparable with PTGBD regarding clinical success, with less reintervention and readmission for acute cholecystitis with high surgical risk. With LAMS, EUSGBD was associated with less cholecystitis recurrence.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.