
Abstract
Introduction:
Success rate of laparoscopic pyeloplasty for ureteropelvic junction obstruction (UPJO) in children is comparable with open pyeloplasty. Prolonged ileus and injury to adjacent viscera more often occurred in transperitoneal approach; however, longer operation time is noted in retroperitoneal approach.
Purpose:
This study presented a hybrid retroperitoneoscopic pyeloplasty (HRP), for congenital UPJO in infants weighing <10 kg.
Materials and Methods:
From February 2017 to June 2020, 10 HRP procedures were performed in 9 patients by 1 surgeon. Retroperitoneal dissection of the renal pelvis and the upper third ureter was first performed, followed by extracorporeal suturing for pyeloureterostomy.
Results:
Mean operative age and body weight were 4.23 ± 3.69 months and 6.18 ± 1.57 kg. Operative, CO2 inflation, and extracorporeal suture time were 147.9 ± 39.5, 40.6 ± 11.2, and 62.9 ± 26.1 minutes, respectively. Surgical outcome was confirmed by renal ultrasound and diuretic renogram. Postoperative follow-up duration was 15.2 ± 7.7 months. Three patients had postoperative febrile urinary tract infection and recovered after antibiotic treatment.
Conclusion:
In infants or smaller children with UPJO, the HRP procedure may be considered as an effective and minimally invasive alternative with shorter learning curve for inexperienced surgeons.
Introduction
Anderson-Hynes pyeloplasty is still the gold standard for surgical intervention of ureteropelvic junction obstruction (UPJO) in children, and minimally invasive options have blossomed and ripened over the past two decades.1,2 Robotic pyeloplasty has similar results with open pyeloplasty (OP) in patients weighing <10 kg, but costs more compared with laparoscopic pyeloplasty (LP).3,4 A meta-analysis study shows that LP shortens length of hospital stay and lowers complication rate compared with OP. 5 Controversies remain while comparing transperitoneal with retroperitoneal approach: transperitoneal laparoscopic pyeloplasty provides a shorter operative time and lower conversion rate; retroperitoneal laparoscopic pyeloplasty (RLP) advances the start of oral feeding and decreases hospital stay.6,7
Lima and colleagues performed retroperitoneoscopic-assisted approach since January 2005, which later proved to shorten operative time compared with other minimally invasive choices. 8 The authors had published a hybrid procedure in UPJO patients <1 year old or weighing <10 kg, and found it to be a safe, effective, and less time-consuming alternative to LP. However, Di Pace et al. proposed posterior one-trocar-assisted pyeloplasty to prevent accidental peritoneal tears, which were thought to be related to lateral incision. 9
Past studies rarely focused on specific range of age or weight. Some studies even contain mostly older children or adolescence. But with the improvement of ultrasound and surgical technique, early intervention for those in need could prevent deterioration of kidney function. 10 Therefore, this study conducted a hybrid retroperitoneoscopic pyeloplasty (HRP) for congenital UPJO in infants weighing <10 kg and evaluated the surgical outcomes.
Materials and Methods
From February 2017 to June 2020, the patients with congenital UPJO, <1 year old, and <10 kg were included by retrospectively reviewing the medical records and image studies. The diagnosis of congenital UPJO was based on clinical manifestations, renal ultrasound, and diuretic renography. Indication of obstruction was confirmed by renal ultrasound showing severe hydronephrosis with renal cortical thinning, society of fetal ultrasound grade 3 or grade 4, and diuretic renography revealing no response to Lasix (half-life <20 minutes) to clear the isotope from the kidney. 11 All of the patients received HRP under the lateral decubitus position. Retroperitoneal dissection of the renal pelvis and upper third ureter was first performed through the first port over the subcostal area, and another one port above the iliac crest for assistance was made.
The renal pelvis and upper ureter were pulled out from the subcostal incision, and dismembered pyeloplasty was then completed extracorporeally. The surgical outcomes were collected and analyzed. Patient's demographics are summarized in Table 1. All subjects enrolled in this study were approved by the Institutional Committee on Human Research of Taichung Veterans General Hospital (TCVGH), Taichung, Taiwan, in accordance with the guidelines of the Declaration of Helsinki and the International Conference on Harmonization for Good Clinical Practice (Institutional Review Board TCVGH No. CE19373A).
Details of the Patient's Characteristics
Patient no. 8 and 10 is the same patient.
UPJO, ureteropelvic junction obstruction.
Surgical technique
The patient was placed in a lateral position, and the procedures are shown in Figure 1. A 5 mm in length transverse incision was first made over the subcostal area of midaxillary line, and the retroperitoneal space was entered directly after the Gerota's fascia was opened. A 5 mm balloon blunt tip trocar (Applied Medical Resources Corp., Rancho Santa Margarita, CA) was inserted, and a 30° rigid telescope (Karl Storz Endoscopy, Taipei, Taiwan) was entered. Blunt dissection of perirenal soft tissue by the telescope was performed under direct vision to create the retroperitoneal space until it was enough to insert another trocar just above the anterior spine of iliac crest. A nontraumatic forceps was inserted to perform blunt and sharp dissection until the kidney, renal pelvis, and the upper third ureter were isolated.
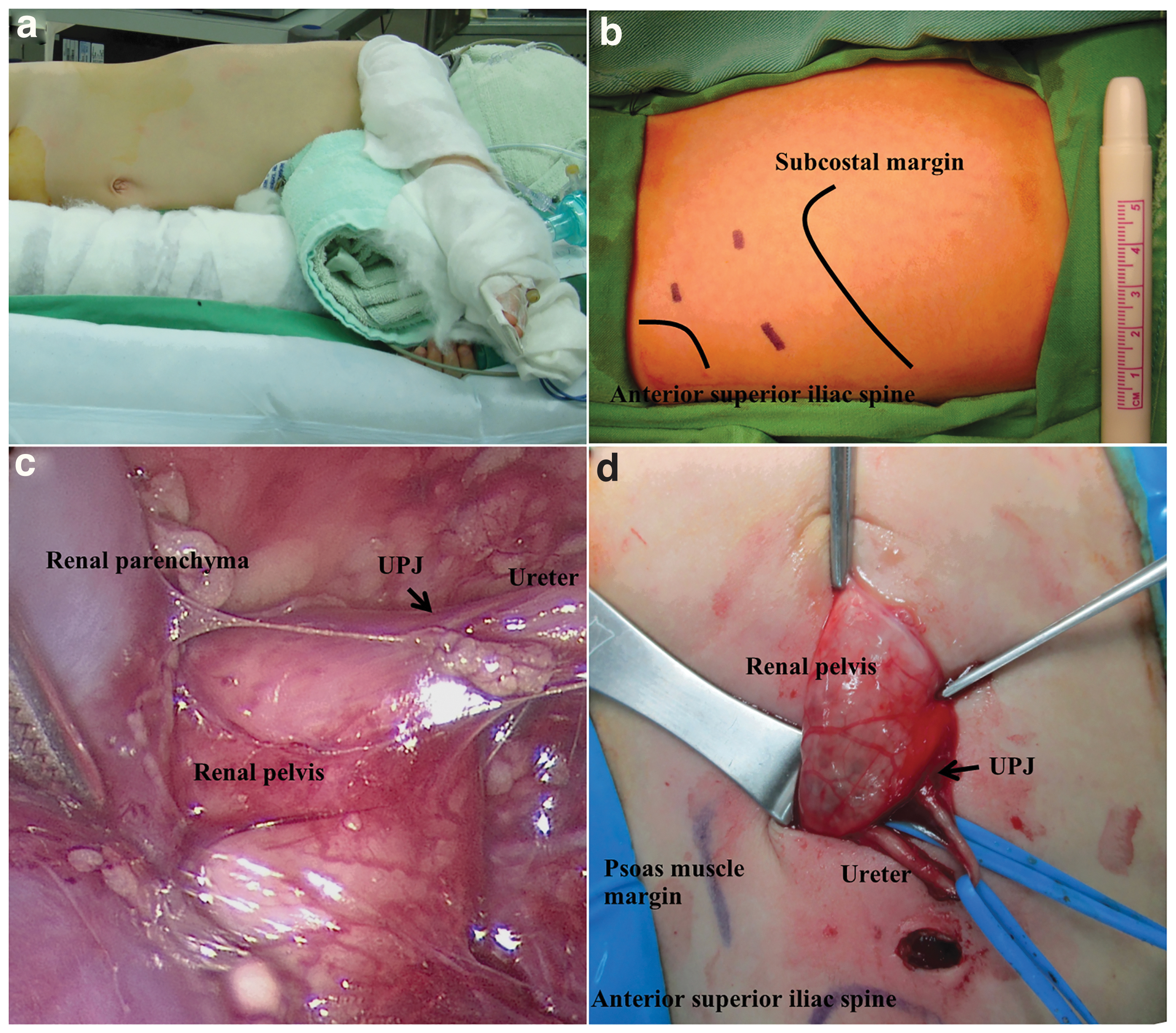
The operative photography:
The ureteropelvic junction (UPJ) site was identified and looped with a vessel loop. The subcostal wound was enlarged to 1.5 cm in length, and the UPJ site was pulled out from the wound. Anderson-Hynes dismembered pyeloplasty was then performed extracorporeally with 6-O PDS*II sutures (Ethicon, Inc., Johnson & Johnson Company, New Brunswick, NJ), and a 3F or 4F Double-J ureteral stent (BIOTEQ Corp., Taipei, Taiwan) was inserted in an antegrade manner through the anastomosis. The position of the catheter may be confirmed by intraoperative fluoroscope. The renal unit was put back into the retroperitoneal space, and a perirenal drainage tube was placed in all patients. Foley was removed 1–2 days after the operation, and the patients were discharged after oral feeding resumed. The Double-J stent was removed 2–4 weeks after pyeloplasty under general anesthesia.
All of the patients were followed up 1 month after pyeloplasty using renal ultrasound or diuretic renography, then with renal ultrasound in a 3-month interval. The minimum, maximum, average, and standard deviation were calculated using Microsoft Excel.
Results
A total of 9 patients with 10 renal units was enrolled, 8 male patients with 5 left-side UPJO, 3 with right-side UPJO, and 1 female patient with bilateral UPJO. Details of the patient's characteristic are listed in Table 1. All patients underwent HRP without conversion to open surgery. The mean operative age was 4.23 ± 3.69 months (*range 27 days to 11 months 28 days), and the mean operative weight was 6.18 ± 1.57 kg (range 3.5–8.9 kg). Complete duplex of left collecting system with UPJO in the lower moiety was noted in patient no. 5, and anterior urethral valve was concurrently found and managed by transurethral incision in patient no. 9.
Operative and postoperative parameters are shown in Table 2. The mean operative time (incised the wound to stitch up) was 147.9 ± 39.5 minutes (range 115–230 minutes); carbon dioxide inflation time was 40.6 ± 11.2 minutes (range 25–60 minutes); extracorporeal suture time was 62.9 ± 26.1 minutes (range 40–120 minutes); duration of perirenal drainage tube placement was 3.3 ± 1.4 days (range 2–7 days); duration of Double-J stent placement was 12.1 ± 8.1 days (range 0–24 days); and hospital stay was 8.4 ± 5.9 days (range 3–20 days). Six of these patients had the hospital stay from 3 to 5 days, but 4 of them had comorbidity to prolong the hospital stay (one had the history of hypoxic encephalopathy and urinary tract infection, one received percutaneous nephrostomy before the operation, and two had febrile urinary tract infection [UTI] before the operation.). Mean postoperative follow-up duration was 15.2 ± 7.7 months (range 2.3–24.4 months).
Operative and Postoperative Parameters in 10 Hybrid Retroperitoneoscopic Pyeloplasty Procedures
SD, standard deviation.
All of the patients received HRP. Extracorporeal suture time ranged from 40 to 60 minutes per anastomosis, which was randomly performed by 2 pediatric surgeons. Resolution of UPJO was confirmed by ultrasound and diuretic renography (Fig. 2). Three patients had postoperative febrile urinary tract infection and recovered after antibiotic treatment. Two patients had recurrent UPJO due to torsion of the previous anastomosis and received transperitoneal laparoscopic pyeloureterostomy with good result. One child with prematurity and congenital neurological deficits died of pulmonary infection with sepsis, but no operative complication was noted for 2 months postoperatively.
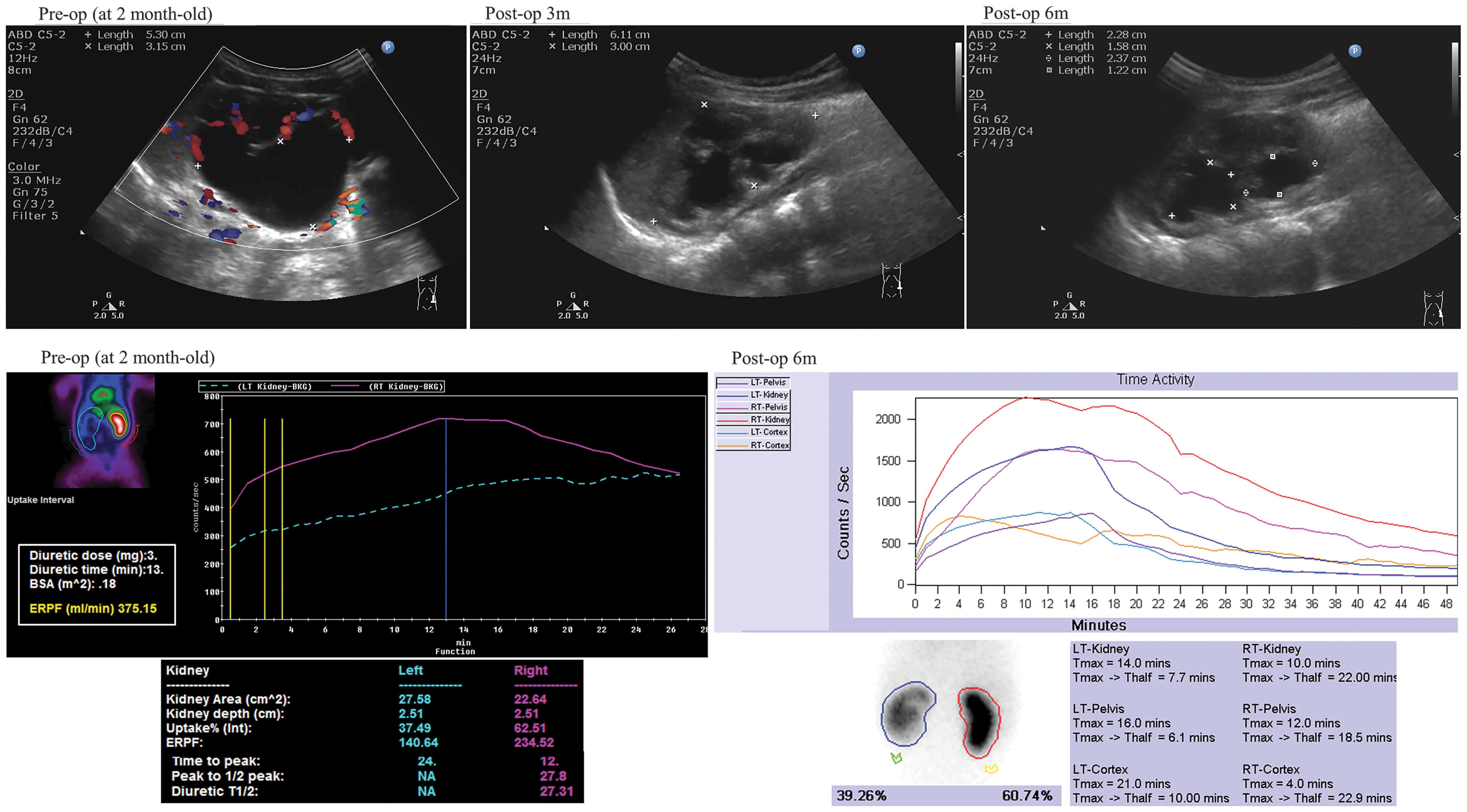
Pre- and postoperative images of Patient no. 2 in this study: significant improvement of left hydronephrosis and renal cortex growth were noted by ultrasound at 3 and 6 months after surgery (upper role). Good response to lasix of left kidney on diuretic renography was confirmed 6 months after surgery (lower role).
Discussion
In the past two decades, two meta-analysis studies proved the feasibility and safety of LP with less length of hospital stay and lower complication rate than OP groups.5,12 However, surgeons rarely used it in children <12 months due to potential problems with hemodynamic and respiratory disorders, the difficulty of the technique, and most importantly, the rapid recovery from open surgery in patients within this age group.13,14 Years later, Kallas-Chemaly and colleagues found the duration of hospitalization and intravenous acetaminophen use were significantly lower, but the operative time was significantly longer in RLP than posterior lumbotomy group (85.8 versus 163.0, P = .001) in children <12 months of age. 15
In 2004, El-Gohary reported their experience with transperitoneal laparoscopic-assisted pyeloplasty, which combines the advantage of minimally invasive laparoscopy with the accuracy and effectiveness of open suturing. 16 It is able to avoid time-consuming intracorporeal suture and shorten learning curve for unexperienced surgeons, which is compatible with this study. In 2005, Lima and colleagues 8 started to use retroperitoneoscopic-assisted pyeloplasty, which provided rapid access to the kidney. Their 8-year experience demonstrates the similar or even shorter operative times than those of other minimally invasive choices, and high success rate as OP with minimal scars. 8 But the five conversion cases due to accidentally open of peritoneum gave birth to posterior one-trocar-assisted pyeloplasty, invented by Di Pace et al. 9 He hypothesized that in lateral position, the trocar incision is very close to the lateral peritoneum reflection, and the preliminary experience needs further follow-up. 9
Besides, the authors presented a hybrid procedure in UPJO patients <1 year old or weighed <10 kg, and found it to be a safe, effective, and less time-consuming alternative to LP. 17 In summary, compared with total retroperitoneoscopic pyeloplasty, HRP may provide larger working space and avoid time-consuming intracorporeal suture and shorten learning curve. Incised the abdominal wall layer by layer. Then open Gerota's fascia to expose the kidney, and keep going blunt dissection to free the kidney. During the extracorporeal pelviureteric anastomosis, possible traction injury to the renal vessels was prevented by complete dissection of renal parenchyma to surrounding soft tissue. To date, no patient demonstrated any postoperative deterioration of renal function.
In this study, it mainly focused on infants or young children (<1 year old or weighing <10 kg) with UPJO. Although the operative time is slightly longer compared with Lima's study (147.9 versus 139 minutes), the patients in this study are younger and lower in weight, resulting in smaller operative field. As for patient <12 months old, this HRP procedure slightly decreases operative time compared with RLP practiced by Kallas-Chemaly et al. (147.9 versus 163.0 minutes) 15 and the authors previously presented in 2014 (147.9 versus 231.9 minutes). 17 Since the patients were discharged after oral feeding resumed, the length of hospital stay is longer in this study. The complication rate is higher (30%) in this study, but all three urinary tract infections were treated by antibiotics and the patients recovered smoothly.
Torsion of the anastomosis occurring in 22% (2/9) patients is high and should be avoided. Similar to open retroperitoneal pyeloplasty, stay sutures over the medial side of the upper ureter and renal pelvis were marked before the renal pelvis and ureter were incised. After the extracorporeal pelviureteric anastomosis was completed, the axis of the anastomosis was rechecked by retroperitoneoscope to confirm no torsion of the anastomosis. The retrospective feature and lack of direct comparison with other surgical procedure still limits this study; therefore, a prospective randomized control trial may be needed.
Conclusion
In infants or smaller children (<1 year old or weighing <10 kg) with congenital UPJO, HRP can be an effective and minimally invasive procedure with shorter learning curve, but needs more experiences to reduce the complication rate.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors thank Taichung Veterans General Hospital (Project Nos. TCVGH-1095401B and TCVGH-1095402C) for funding this research.