
Abstract
Introduction:
Nissen Sleeve (NS) was introduced in the bariatric armamentarium with the purpose to decrease the risk of reflux symptoms following sleeve gastrectomy. The aim of this study was to evaluate our personal experience with this new technique, in particular concerning early postoperative complications (<30 days).
Methods:
We retrospectively reviewed our prospectively collected data on consecutive morbid patients with obesity receiving NS from December 2019 to August 2020. All data pertaining to each patient, including demographic data and preoperative and postoperative clinical data, were collected.
Results:
A total of 28 N-sleeve procedures were performed in the considered period. All the patients had a hiatal hernia that was evaluated between 2 and 6 cm of extent in the preoperative work. Esophagitis of stage A, according to the Los Angeles classification, was detected in 71% of the patients, while 8 out of 28 patients presented a stage B esophagitis. One of the patients had a preoperative diagnosis of Barrett esophagus. A complete disappearance of gastroesophageal reflux disease (GERD) symptoms was achieved in 25 patients out of 28, while the remaining patients reported an improvement in symptoms and continued to be treated with low doses of proton pomp inhibitors. Two reinterventions (7.1%) were performed (Clavien-Dindo IIIb). Three other patients (10.7%) experienced a transient postoperative dysphagia that in one case persisted for 4 months (Clavien-Dindo II). All the patients were managed with conservative treatment, and in each case an endoscopic dilatation was necessary.
Conclusions:
NS appears to be a safe surgical technique with an acceptable early postoperative complication rate. NS appears to be effective in treating patients suffering from obesity and preoperative reflux, but the data are insufficient to establish whether it can reduce the long-term risk of de novo GERD in laparoscopic sleeve gastrectomy patients.
Introduction
Over the last 10 years, laparoscopic sleeve gastrectomy (LSG) has become the most frequently performed bariatric procedure.1–3 Its success among the other bariatric procedures can be explained by several factors. First, LSG offers similar results comparing to laparoscopic Roux-en-Y gastric bypass (LRYGB) 4 between the effectiveness in treating obesity and related comorbidities in the short- and long term with good quality of life. Moreover, LSG is considered less technically demanding compared to other malabsorptive procedures. Unfortunately, as with all other bariatric surgery procedures, sleeve gastrectomy is not exempt of long-term complications. The main long-term side effect of LSG seems to be the gastroesophageal reflux disease (GERD). Following LSG, the presence of GERD symptomatology was reported in up to 20%–60% of patients, in recent studies.5–9 For these reasons, in case of patients presenting with GERD before bariatric surgery, the current recommendation is to propose LRYGB as a primary operation. These recommendations are even stronger when preoperative reflux is associated with a hiatal hernia. Unfortunately, even patients undergoing LRYGB are not completely exempt from the risk of developing postoperative GERD. In addition, more than 35% of the patients who underwent RYGB had at least one complication within the 10-year follow-up period. 10
Considering all these findings, Montpellier University bariatric team proposed in 2016 a modification to the usual surgical technique of LSG by adding a Nissen fundoplication—Nissen Sleeve (NS). 11 The intents of this technique were to minimize the rate of postoperative GERD, to protect the staple line of the angle of His, and finally to provide a safe and effective alternative for patients with contraindication to LRYGB because of GERD. Even if the initial results of the technique are encouraging, performing the Nissen valve remains a sensible technical point that can turn a relatively simple intervention like LSG to a more complex procedure like NS. The aim of this study was to evaluate our personal experience with this technique, in particular concerning early postoperative complications (<30 days).
Methods
The IRB approval was validated by ELSAN and informed consent was obtained from all individual participants included in the study. We retrospectively reviewed our prospectively collected data on consecutive morbid patients with obesity receiving NS from December 2018 to August 2020. All data pertaining to each patient, including demographic data and preoperative and postoperative clinical data, were collected. The adoption of this nouvelle technique took place gradually. For this reason, only patients with clinical signs of GERD under proton pump inhibitor (PPI) treatment and the presence of severe esophagitis, according to the Los Angeles classification, with concomitant presence of hiatal hernia were included in the first phase of our experience. From a clinical point of view, preoperative GERD was considered for patients presenting with intense heartburn, epigastric pain, nausea, vomiting, regurgitation, ascent of gastric fluid into the mouth in a lying position, and continuous dry cough, hoarseness, and sore throat, according to the Montreal definition. For a better definition of the grade of hiatal hernia, a double check with gastroscopy and upper gastrointestinal series was performed during the preoperative workout. All the patients were informed about the nature of new technique, and they signed an informed consent. The main outcome of this study was the type and the rate of postoperative complications. Postoperative complications were classified based on the Clavien-Dindo classification 12 and the time of onset (early, during the first postoperative month; or late, after the first postoperative month). The remission of GERD was validated clinically by the disappearance of the preoperative symptoms in patients without PPI treatment. Continuous demographic variables were expressed as mean ± standard deviation and range. Categorical variables, in addition to complications, were reported as numbers and percentages. Continuous outcome variables were generally reported as mean ± standard deviation and range.
Surgical technique
According to the technique presented by Nocca et al. 11 with the patient placed in modified lithotomy position, N-sleeve was performed using a five-port technique. The first step comprises the dissection and reduction within the abdominal cavity of the hiatal hernia.
The mobilization of the esophagus is performed on at least 5 cm, carried out cautiously to avoid any damage to the vagus nerve. The hiatal orifice is closed with nonabsorbable interrupted sutures. The greater curve of the stomach is dissected from the short gastric vessels and the gastrocolic ligament by means of an impedance coagulator Ultracision (Ethicon Endo-surgery; Johnson-Johnson, Inc., 2010). A careful dissection is performed at the level of the gastric fundus, keeping an appropriate distance from the gastric wall, thus avoiding any possible thermal injury to this important part that would be used later to perform the fundoplication. A short 3 cm Nissen valve is created using 2.0 Ethibond suture (Johnson-Johnson, Inc.), calibrated on a 38 Fr gastric bougie. Finally, the stomach is transected with sequential firings of 60-mm Echelon linear stapler with green cartridges (Ethicon Endosurgery). Reinforcing the staple line was not systematically performed. While firing the stapler at the level of the new created valve, particular attention was paid to maintain the natural position of the valve and to preserve its vascularization. No abdominal drains or gastric probes were left at the end of the operation. All the interventions were video recorded to improve our surgical skill in performing the technique. An upper gastrointestinal series was systematically performed at postoperative day (POD) one, and if negative for leak—oral clear liquid started, and patient discharged. All patients were prescribed systematic postoperative multivitamin supplementation and 40 mg PPI during the first 6 months.
Results
A total of 28 N-sleeve procedures were performed in the considered period. Table 1 shows patients' characteristics. All the patients had a hiatal hernia that was evaluated between 2 and 6 cm of extent in the preoperative work. Stage A esophagitis, according to the Los Angeles classification, was detected in 71% of the patients, while 8 out of 28 patients presented a stage B esophagitis. One of the patients had a preoperative diagnosis of Barrett esophagus. A complete disappearance of GERD symptoms was achieved in 25 patients out of 28, while the remaining patients reported an improvement in their symptoms and were treated with low dose of PPI. Operative data are presented in Table 2. There were no deaths. Two reinterventions (7.1%) were performed (Clavien-Dindo IIIb). One patient (n° 7 of the series) was reoperated on at POD 21 for severe dysphagia confirmed by upper gastrointestinal swallow (Fig. 1). A postoperative gastroscopy revealed an important posterior dilation of the Nissen valve. After a complete liberation of the valve an LRYGB was performed. The second patient (n° 26 of the series) presented fever and important epigastric pain at POD 8. A computed tomography (CT) scan showed a pneumoperitoneum at the upper part of the abdomen, and consequently, the patient was taken to the operative room. During a concomitant upper gastrointestinal endoscopy and laparoscopy, a staple line leak was detected at the level of the lower part of the gastric body. A washout of the abdominal cavity was performed, the leak was sutured with three 2-0 PDS stitches, and a drain was placed. At POD 5 an upper gastrointestinal series was carried out with the evidence of leak recurrence, and an endoscopic pig-tail drain was placed. After a first recovery period, at POD 28 the patient presented with vomiting, fever, tachycardia, and thoracic pain, due to a retro-splenic collection associated to an important dilation of the Nissen valve. A diagnosis of gastroparesis associated to a pyloric spasm was made, and an attempt of pyloric pneumatic dilatation and pig-tail drain replacement was performed with favorable outcome. Three other patients (10.7%) experienced a transient postoperative dysphagia that in one case persisted for 4 months (Clavien-Dindo II). All the patients were managed with conservative treatment, and in each case an endoscopic dilatation was necessary.
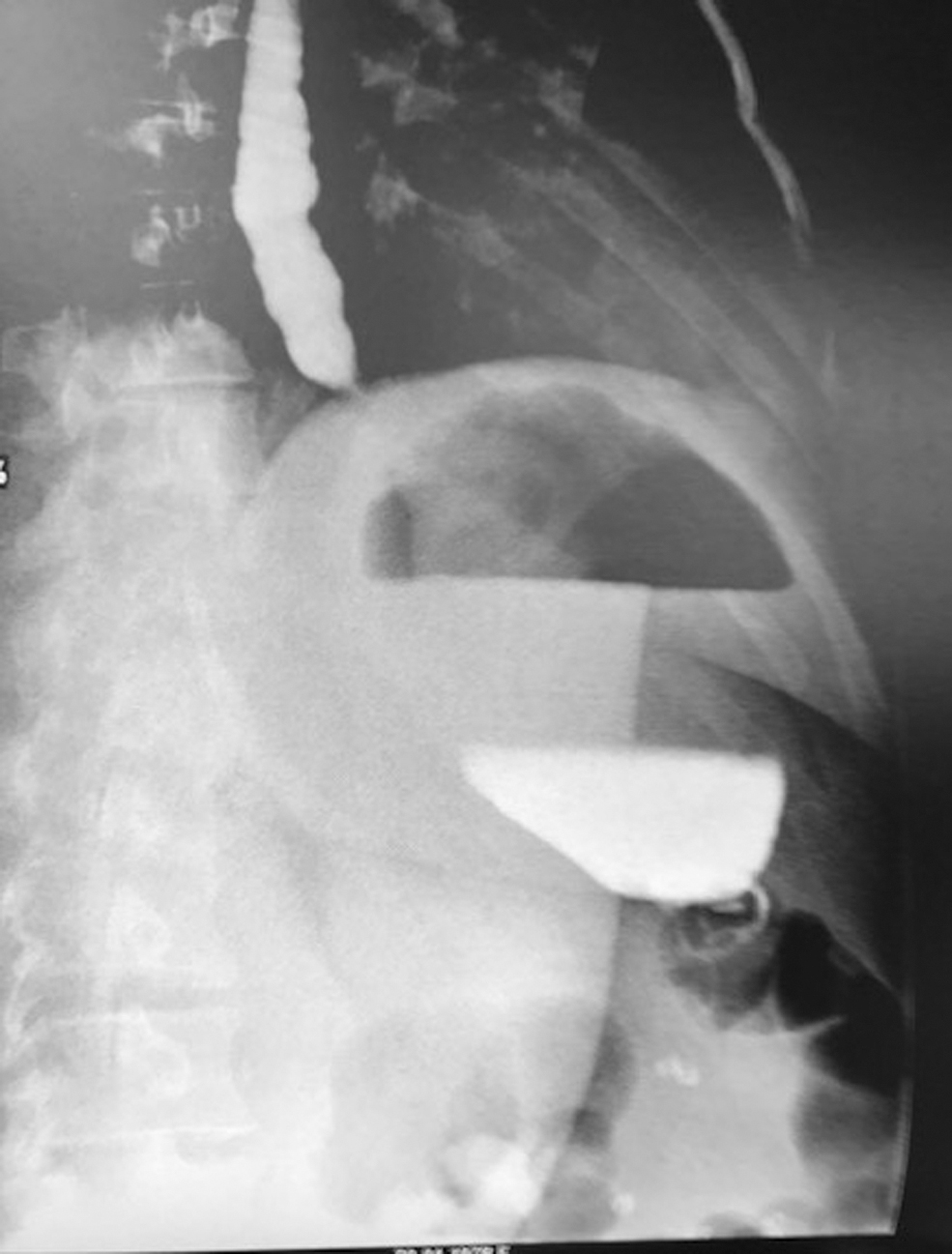
Abnormal postoperative gastrointestinal swallow.
Population Preoperative Characteristics
BMI, body mass index.
Operative Data
LOS, length of hospital stay.
Discussion
The association between obesity and GERD is very well known. Compared to the general population, in obese patients GERD symptoms are present in more than 50% of patients, and more than 70% of patients present evidence of reflux disease at PH-metry.13,14 The pathophysiology of GERD in obese patients is notably multifactorial, and it includes an altered gastroesophageal gradient pressure due to intragastric and intra-abdominal adiposity compression, frequently associated with a hiatal hernia. The use of LSG treatment in patients with preoperative GERD remains controversial. While in some studies LSG combined to hiatal hernia repair showed good results in controlling GERD, in other recent studies LSG seems to worsen preexisting GERD and increase the risk of de novo GERD and Barrett's esophagus. The real pathogenesis of GERD after LSG is not completely clear. LSG induces an alteration in the angle of His with consequent hypotony of the lower esophageal sphincter after the division of muscular sling fibers, a decrease in gastric volume that for the Laplace's law results in an increase in intragastric pressure, and a decrease in ghrelin secretion that causes a gastric dysmotility. For all these reasons, a new bariatric technique able to better control GERD in patients with obesity was conceived by the Montpellier Bariatric Team. The association of a consolidated antireflux operation as Nissen fundoplication to an effective bariatric technique as LSG offered the possibility to perform LSG in patients with preexisting GERD and to decrease the onset of postoperative GERD and Barrett's esophagus in bariatric patients. Nocca et al. 11 recorded in their very early experience a disappearance of preoperative GERD in 22 out of 25 patients at 1 year of follow-up. Similarly, Ben Amor et al. 15 showed an impressive result, with only 1 patient with symptomatic GERD at 12-months follow-up. Our results seem to confirm this tendency although the follow-up is shorter. The downside is the increase in the technical difficulty of an intervention that owes its widespread worldwide diffusion also to its simplicity of execution. Inevitably, adding to the usual operating time of the sleeve the creation of the Nissen valve and above all the correct section of the stomach to preserve its vascularization increase the difficulty of the intervention and, consequently, increase the number of cases necessary to achieve the same proficiency as for LSG. This fact could theoretically increase the risk of postoperative complications. In reality, the creation of the Nissen valve and wrapping the region of the cardia allow to protect the upper part of the staple line and the esophagogastric junction. This region represents an anatomical area of weakness that is more sensitive to any increase in intragastric pressure. For this reason, almost all leaks after LSG originate from this location just below the gastroesophageal junction. The N-sleeve valve could avoid this potential complication. In our experience, we recorded only one leak that was located in the lower part of the staple line, far from the Nissen's valve. Ben Amor et al., in a cohort study of 70 patients, recorded 1 patient with a fistula at the level of the gastric longitudinal staple line that was successively converted in LRYGB. Similarly, Chouillard et al. 16 presented a clinical case of a patient operated by N-sleeve complicated by two leaks, one anterior at level of the transection line of the sleeved stomach and the second posterior at the level of the valve. For this case the patient was converted in LRYGB as well. Since the technique is recent, the literature data are insufficient to confirm whether the creation of the valve has a protective role at the level of the EG junction. The few cases presented seem to confirm this statement, but studies with a higher number of cases are mandatory.
On the other hand, transdiaphragmatic wrap migration, wrap ischemia with perforation, and severe postoperative dysphagia were also described after Nissen's fundoplication. As it was pointed out from the beginning, there are some technical details that are of paramount importance in the valve creation and resection. In the NS technique the vascular supply of the valve comes only from the left gastric artery, so during resection it's really important to avoid any rotation by applying a symmetrical traction through the anterior and posterior wrap wall. In our experience this is the key point of this procedure. An excessive and asymmetrical traction could generate a valve rotation with vascular damage, whereas an insufficient traction could leave a redundant posterior valve wall with consequent food stasis. In the first case we expose the patient to the risk of perforation while in the second to postoperative dysphagia and reflux recidivism. When a postoperative wrap perforation is diagnosed, as showed by Skalli, 17 it can be easily managed by laparoscopic wrap resection that allows a prompt recovery for the patient.
In the present series we recorded four cases of transient severe dysphagia. In 1 patient this symptom needed reoperation, and in another case it persisted until the fourth postoperative month. While in the first case postoperative dysphagia was consequent to an error in the valve construction, in the second patient the cause was different. A hiatal stenosis following crural repair and a too long or too tight or twisted valve are frequently invoked to explain postoperative Nissen dysphagia. To avoid these complications, we calibrated both the crural repair and valve construction over a 38 Fr nasogastric tube. Moreover, the video records of the initial procedure were reviewed, and we found neither a wrap twist nor a too long valve at the end of the operation. Nevertheless, in all these patients we started our gastric resection at about 2 cm from the pylorus. The aim of the Nissen operation is to create a high-pressure gradient between the 3-cm wrap zone and the remaining stomach that prevents the reflux. At the same time, the gastric resection during LSG decreases gastric compliance and increases intragastric pressure, with consequent alteration of this gradient. In our opinion, an excessive antral resection up to the pylorus, which further increases the intraluminal pressure, counteracts the emptying capacity of the Nissen valve causing a postoperative dysphagia. In the original technique, Nocca et al. 11 started gastric resection at 5 cm far from pylorus and so they spared a low-pressure zone like the antrum. This way they probably preserved the descendent pressure gradient between the valve and the pylorus that permits a correct transit of the bolus along the entire stomach.
Conclusions
NS appears to be a safe surgical technique with an acceptable early postoperative complication rate. This technique could potentially decrease the risk of leak at the level of the angle of His but on the other hand is more technically demanding than the classic LSG, with the risk of increasing the overall rate of complications. Regarding the LSG and GERD controversy, NS appears to be very effective in treating patients suffering from obesity and preoperative reflux, but the data are absolutely insufficient to establish whether it can reduce the long-term risk of de novo GERD in LSG patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.