
Abstract
Background:
Uniportal video-assisted thoracoscopic surgery (VATS) has been shown to offer improved postoperative outcomes compared with multiportal technique. Shorter operative time has rarely been described. Our objective was to compare operative time and clinical outcomes between uniportal and multiportal VATS approaches for lung resection.
Methods:
This is a retrospective review of patients that underwent video-assisted thoracoscopic lung resection at United States Veterans Affairs centers between 2008 and 2018 using the Veteran Affairs Surgical Quality Improvement Program. Cases were assigned to uniportal (single surgeon) or multiportal cohorts. Multivariable analysis of clinical outcomes was performed, adjusting for preoperative confounding covariates. Temporal trend in operative time in uniportal cohort was analyzed in the context of cumulative operative volume using Spearman's rank correlation coefficient, rho (ρ).
Results:
In total, 8,212 cases were selected from 2008 to 2018 at Veterans Affairs centers: 176 (2.1%) uniportal and 8036 (97.9%) multiportal cases. Uniportal cohort was significantly associated with shorter operative time (1.7 hours versus 3.1 hours, P < .001), higher adjusted odds of surgical site infection (adjusted odds ratio = 2.76; P = .005), and longer length of stay (6 days versus 5 days; P = .04). Uniportal cohort operative time decreased over time (ρ = −0.474), with most significant change corresponding with increased cumulative operative volume from 25 to 44 cases.
Conclusions:
Uniportal technique offered shorter operative duration in veterans compared with multiportal approach, validating its technical advantages. Operative time decreased as cumulative operative volume increased, demonstrating a learning curve. Future studies should prospectively investigate any association between operative time and clinical outcomes after thoracoscopic lung resection.
Introduction
Since first being described in 1912 by Jacobeus to lyse adhesions from tuberculosis, thoracoscopy has grown into an important pillar of thoracic surgery. 1 Over the past three decades, the field has evolved with the widespread use of video-assisted thoracoscopic surgery (VATS) in the diagnosis and treatment of chest pathology.2,3 When compared with conventional open thoracotomy, VATS has been shown to have superior perioperative outcomes, with lower rates of postoperative complications, shorter length of hospital stay, and decreased 30-day mortality.4,5 In addition, several studies have shown VATS to have noninferior oncologic outcomes, including 5-year overall survival and disease-free survival in the treatment of lung cancer.6,7
VATS has traditionally been performed through three incisions, or ports. However, surgical approach across all fields has continued to move toward minimally invasive techniques, which has led to the development of single incision, or uniportal VATS (U-VATS). Since the first U-VATS wedge resection described by Rocco et al. in 2004, the technique has been continuously refined and adopted in increasingly complex procedures. 8 By utilizing one incision, U-VATS offers less postoperative pain and improved patient satisfaction compared with multiportal VATS (M-VATS).9,10 Several meta-analyses comparing U-VATS versus M-VATS have shown U-VATS to have superior postoperative outcomes, including length of stay and complication rates, and comparable oncologic outcomes.11,12
There is a growing body of literature to validate the technical superiority of U-VATS, with the geometric characteristics and use of articulating instruments providing precision with intrathoracic maneuvers and exposure akin to that of an open procedure. By deploying the instruments and optical source through the same port, a visual field more spatially congruent with current two-dimensional VATS monitors is created.13,14 As with all innovations in surgery, there is an expected learning curve with U-VATS. Several cumulative sum analyses have calculated that between 27 and 44 cases needed to be performed before significant decreases in operative time were detected.15,16
United States veterans are an ideal cohort to compare these two minimally invasive techniques for several reasons. The veterans affairs (VA) health care system is the single largest integrated health care delivery model in the country, with veterans comprising 7.6% of the population. 17 In addition, the Veterans Affairs Surgical Quality Improvement Program (VASQIP) database is the central repository for surgical outcomes at all Veteran Affairs Medical Centers (VAMCs). 18
Although the role of M-VATS over thoracotomy has been explored in the veteran population, the potential benefits of U-VATS must be further elucidated. 19 To our knowledge, there are no existing studies comparing outcomes between these two techniques in the veteran population. The objective of this study was to compare the perioperative and postoperative outcomes of veterans undergoing U-VATS versus those undergoing M-VATS, with operative time being the primary outcome of interest.
Materials and Methods
This is a retrospective review of the VASQIP database, a validated source of data for quality improvement and surgical outcomes, with data extraction and review meticulously performed by specially trained nurses. 20 Veterans undergoing VATS at all VAMCs from 2008 to 2018 were retrospectively identified using current procedural terminology (CPT) codes for thoracoscopic pulmonary resections including wedge resection (CPT = 32666, 32667, 32668), lobectomy (CPT = 32663, 32670), segmentectomy (CPT = 32669), and pneumonectomy (CPT = 32671).
The sample was then divided into two groups. The first group comprised patients who underwent VATS lung resection through the uniportal technique, performed by a single thoracic surgeon at one VAMC using the unique VASQIP facility identifier. The second group consisted of those who underwent VATS lung resection at all other VAMCs in the database, and represented the M-VATS arm (Fig. 1). Patient demographics and unadjusted outcomes were compared between the two groups.
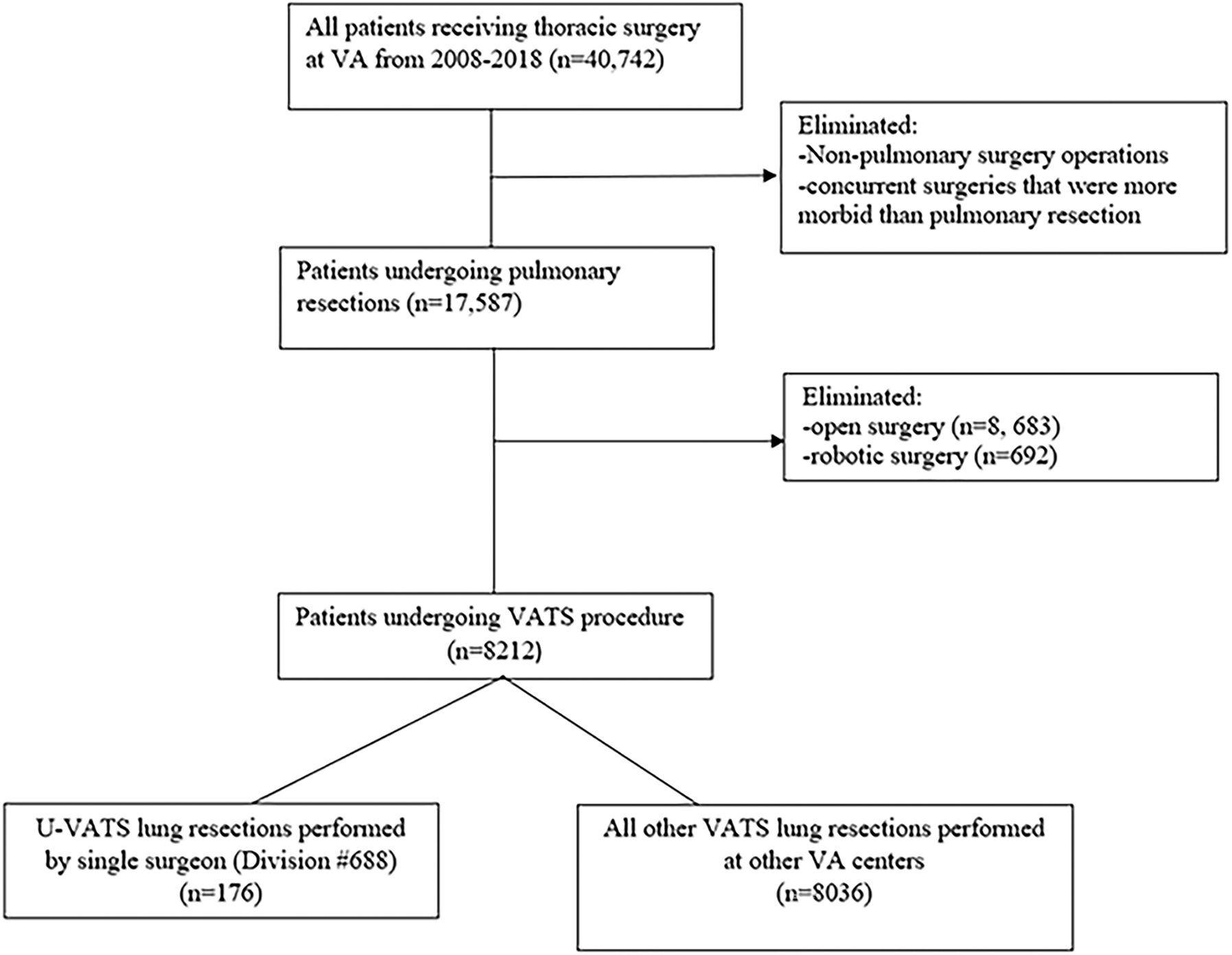
Method of cohort selection and assignment. VA, veterans affairs; VATS, video-assisted thoracoscopic surgery; U-VATS, uniportal video-assisted thoracoscopic surgery.
Primary outcome of interest was operative time. Secondary outcomes of interest were mortality, length of postoperative hospital stay (LOS), postoperative complications, and number of red blood cell units transfused intraoperatively. Mean operative time, incidence of postoperative complication, and LOS were further stratified by type of procedure using corresponding CPT code for wedge resection, lobectomy, segmentectomy, and pneumonectomy and compared between the two arms.
Independent samples t-test was used to infer statistical significance between parametric continuous variables. Mann–Whitney U test was used for comparison of nonparametric continuous variables. Normality of continuous variables was analyzed using the Kolmogorov–Smirnov test in conjunction with measures of skew and kurtosis. Chi-square or Fisher's exact test was utilized for analysis of categorical variables between the two cohorts for adequate and low cell counts (≥25% of cells with expected count ≤5), respectively.
Preoperative demographics, clinical, and operative characteristics were compared between cohorts to identify potential confounding covariates. Multivariable logistic regression models were used to compare categorical outcomes. Adjusted odds ratio with 95% confidence intervals and P values were reported. Multivariable generalized linear models were used to compare continuous variables. For continuous variables, beta coefficient (β) was reported with corresponding standard error.
Continuous outcomes including LOS and number of red blood cell units given were severely positively skewed with moderate kurtosis. Therefore, these outcomes were natural logarithm (ln) transformed to meet the assumptions of normally distributed residuals and homoscedasticity among variance of error terms within multivariable linear regression. All multivariable models followed a backward stepwise selection procedure triangulated with purposeful selection to obtain final reduced multivariable models. Univariate patient demographics, clinical, and operative characteristics with corresponding univariate test P value <.2 were entered into multivariable models for adjustment, and stay criterion for the selection procedure was α = 0.1.
Within the U-VATS cohort, mean operative time was reported by year and chronologic trend was assessed with Spearman's rank correlation coefficient rho (ρ) and corresponding P value. Mean operative time per year was provided with cumulative operative volume of the single surgeon in the U-VATS cohort during the study period. For this study, a two-sided P value <.05 was deemed statistically significant. Statistical analysis was performed with SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA). Institutional review board (IRB) approval was obtained, and waiver of consent was applied on the basis that this study was purely retrospective and utilized deidentified data (Institutional Number #01943).
Results
A total of 8212 VATS lung resection procedures were performed at VA centers from 2008 to 2018, with 176 (2.1%) cases performed by a single surgeon and assigned to U-VATS arm and 8036 (97.9%) cases at all other VA centers assigned to M-VATS arm (Fig. 1). Of the U-VATS cohort, there were 77 (43.7%) lobectomy cases, 71 (40.3%) segmentectomy cases, 14 (8.0%) wedge resection cases, and 14 (8.0%) pneumonectomy cases. Of the 8036 M-VATS group, there were 2507 (31.2%) wedge resection cases, 4702 (58.5%) lobectomy cases, 467 (5.8%) segmentectomy cases, and 360 (4.5%) pneumonectomy cases.
Cases in the U-VATS arm were significantly associated with higher proportion black race, history of angina, peripheral arterial disease, history of chronic obstructive pulmonary disease, obstructive sleep apnea, dependent functional status, bleeding disorder, disseminated cancer, preoperative radiotherapy.
U-VATS was also associated with lower proportion of prior myocardial infarction, American Society of Anesthesiologists (ASA) Class >3, and rates of smoking within 1 year before surgery (Table 1). Univariate analysis showed U-VATS to be significantly associated with shorter operative time (1.7 hours versus 3.1 hours), as well as higher proportion surgical site infection (SSI) (2.8% versus 0.8%), Clostridium difficile infection (1.7% versus 0.4%), and significantly longer LOS (median 6 days versus 5 days) (Table 2).
Patient Demographics
Reported as n (%), mean ± SD.
ASA, American Society of Anesthesiologist physical status classification system; BMI, body mass index; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident; EtOH, history of alcohol use; MI, myocardial infarction; PAD, peripheral arterial disease; PCI, percutaneous coronary intervention; SD, standard deviation.
Univariate Analysis of Perioperative and Postoperative Outcomes of Uniportal Versus Multiportal Video-Assisted Thoracoscopic Lung Resection
Reported as n (%).
CAUTI, catheter-associated UTI; CVA, cerebrovascular accident; DVT, deep venous thrombosis; MI, myocardial infarction; PE, pulmonary embolism; RBCs, red blood cell transfusion units; UTI, urinary tract infection; VASQIP, veterans affairs surgical quality improvement program; VTE, venous thromboembolism.
Multivariable adjusted analysis revealed that U-VATS was associated with an adjusted mean operative time 1.41 ± 0.13 hours shorter than M-VATS (P < .001). U-VATS was also significantly associated with higher adjusted odds of SSI (adjusted odds ratio [aOR] = 4.17; P = .003) and C. difficile infection (aOR = 5.92; P = .005). Furthermore, U-VATS cases was significantly associated with an adjusted 13% ± 5% longer hospital stay (P = .013). There were no significant differences detected between the two cohorts in 30-day mortality, overall complication rate, or incidence of unplanned reoperation (Table 3). When stratified by type of lung resection through relevant CPT code, operative time remained significantly decreased in the U-VATS group regardless of procedure (all respective P values <.05) (Table 4).
Multivariate Analysis of Perioperative and Postoperative Outcomes of Uniportal Versus Multiportal Video-Assisted Thoracoscopic Lung Resection
Reported as n (%).
aOR, adjusted odds ratio; CI, confidence interval; β, beta coefficient; CAUTI, catheter-associated UTI; CVA, cerebrovascular accident; DVT, deep venous thrombosis; ln, logarithm; MI, myocardial infarction; NE, not estimable due to too few events; PE, pulmonary embolism; RBCs, red blood cell transfusion units; SE, standard error; UTI, urinary tract infection; VASQIP, veterans affairs surgical quality improvement program; VTE, venous thromboembolism.
Comparison of Mean Operative Time of Uniportal and Multiportal Video-Assisted Thoracoscopic Lung Resection, Stratified by Type of Procedure
Wedge resection defined by CPT = 32666, 32667, 32668. Lobectomy defined by CPT = 32663, 32670. Segmentectomy defined by CPT = 32669. Pneumonectomy defined by CPT = 32671.
CPT, current procedural terminology; VATS, video-assisted thoracoscopic surgery; M-VATS, multiportal VATS; U-VATS, uniportal VATS.
Stratified by procedure type, no statistically significant differences in complication rate were detected between the U-VATS and M-VATS across all operations (Table 5). LOS was significantly longer in U-VATS lobectomy (P < .001) and wedge resection cases (P = .005) relative to M-VATS cases. However, no significant difference in LOS was appreciated in U-VATS versus M-VATS when analyzing segmentectomy and pneumonectomy cases (Table 6).
Comparison of Complication Rate of Uniportal and Multiportal Video-assisted Thoracoscopic Lung Resection, Stratified by Type of Procedure
Presented as (%) of cases with recorded VASQIP complication. Wedge resection defined by CPT = 32666, 32667, 32668. Lobectomy defined by CPT = 32663, 32670. Segmentectomy defined by CPT = 32669. Pneumonectomy defined by CPT = 32671.
CPT, current procedural terminology; VATS, video-assisted thoracoscopic surgery; M-VATS, multiportal VATS; U-VATS, uniportal VATS; VASQIP, veterans affairs surgical quality improvement program.
Comparison of Median Length of Stay of Uniportal and Multiportal Video-Assisted Thoracoscopic Lung Resection, Stratified by Type of Procedure
Presented as median length of stay (days) with interquartile range. Wedge resection defined by CPT = 32666, 32667, 32668. Lobectomy defined by CPT = 32663, 32670. Segmentectomy defined by CPT = 32669. Pneumonectomy defined by CPT = 32671.
CPT, common procedural terminology; VATS, video-assisted thoracoscopic surgery; M-VATS, multiportal VATS; U-VATS, uniportal VATS.
Temporal analysis of operative time by year in the U-VATS group showed that more recent operative years were significantly associated with shorter operative times with a moderate effect size (ρ = −0.474; P < .001) (Fig. 2; Supplementary Table S1). The effect size of the trend was larger when just looking at the latter half of the study period (2011–2018; ρ = −0.531; P < .001) (Fig. 2; Supplementary Table S1). The greatest decrease in mean operative time occurred between 2012 and 2013, with a 1 hour decrease in mean operative time from 2.8 to 1.8 hours. By the end of 2012, 25 U-VATS consecutive cases had been performed, and by the end of 2013, 44 consecutive U-VATS cases had been performed (Fig. 3).
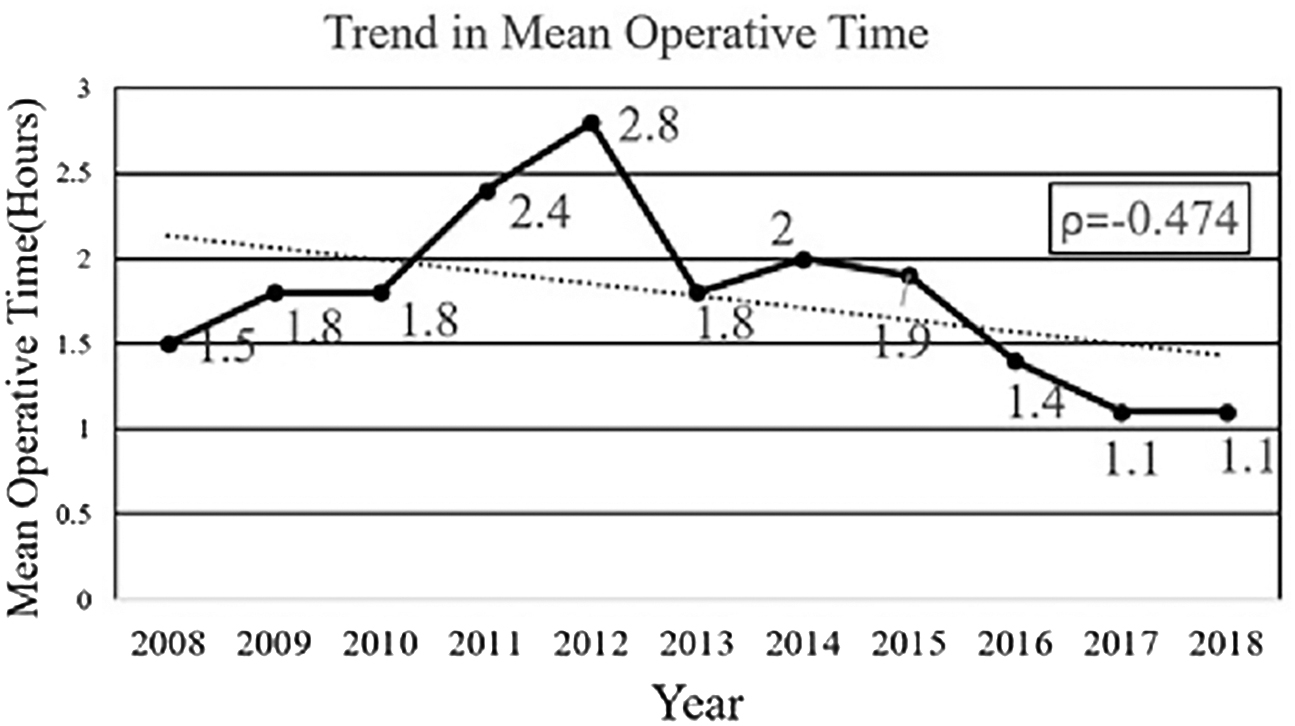
Trend in operative duration of uniportal video-assisted thoracoscopic lung resection cases over time (2008–2018).
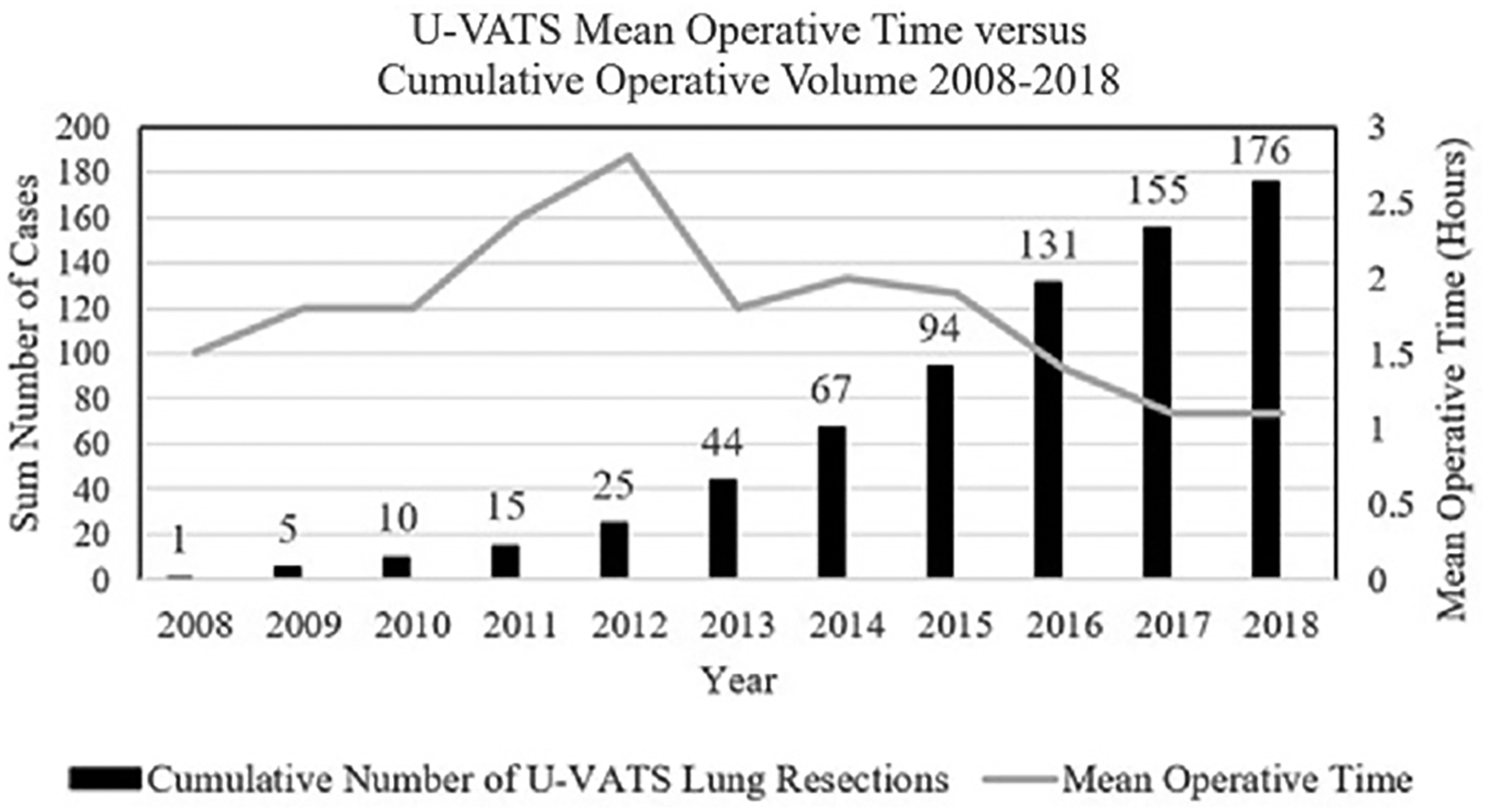
Trend in operative duration of uniportal video-assisted thoracoscopic lung resection cases over time in the context of cumulative operative volume (2008–2018). U-VATS, uniportal video-assisted thoracoscopic surgery.
Discussion
Our study demonstrated that veterans undergoing U-VATS lung resection by a single surgeon experienced significantly shorter operative duration compared with those veterans undergoing M-VATS lung resection. This was demonstrated in several types of VATS procedures, including wedge resection, lobectomy, segmentectomy, and pneumonectomy. There was also a downward trend in operative duration over time in those undergoing U-VATS with increased cumulative operative volume, validating the previously described learning curve of the technique. However, patients who received U-VATS lung resection did experience higher rates of SSI and LOS 1 day longer on average compared with the M-VATS arm. This is one of few retrospective reviews of U-VATS to demonstrate superior operative time, and the only review of the technique in the veteran population to this author's knowledge.
Several meta-analyses have found equivalence or superiority of U-VATS in various postoperative outcome metrics, yet to our knowledge, a statistically significant reduction in operative time has only been demonstrated in one previous single-center retrospective review. However, in that study, the author did not perform a multivariate or propensity matched analysis and acknowledged the limited conclusions of their results.11,12,21 In our study, this finding is preserved even with multivariate analysis to control for possible confounders between the two groups.
Although the technical and visuospatial benefits of U-VATS over M-VATS have been described in detail by Dr. Rocco and colleagues, one must ask why has this not consistently translated to shorter operative duration?13,22 Zhang et al. did not demonstrate a difference in operative time, but they speculated that in the early period of utilizing U-VATS, longer operative times are to be expected as both the surgeon and assistant learn the technique and best strategies for economy of motion. Furthermore, they predicted that as more surgeons gain experience with U-VATS, operative time has potential to be considerably shortened, and our results suggest that this was indeed the case. 23
As with any new surgical technique, the quantification of the U-VATS learning curve has been the subject of much interest and how this could be translated to shorter operative duration and ultimately improved outcomes. To that end, we did demonstrate a downward trend in operative time over the span of our retrospective review, with the greatest change coming from 2012 to 2013. This occurred in the range of 25 cases (by end in 2012) to 44 cases (by end of 2013). This may constitute the U-VATS learning curve in our study, which interestingly is exactly within the range of cumulative sum analyses in the literature.15,16,24
Of note, the thoracic surgeon who performed the U-VATS cases in this study has prior extensive experience with traditional M-VATS, and Martin-Ucar et al. demonstrated that this experience could help “shorten” the learning curve for U-VATS. 25 Our improvements in operative time did not stop after the supposed learning curve was reached. Indeed, Stamenovic et al. explored the presence of both efficiency and “mastery” in which objective metrics have minimal variation. Using the metric of operative time, “mastery” was reached after 39 consecutive U-VATS cases performed by an experienced minimally invasive thoracic surgeon. 16
We posit that the continual improvements in operative time we demonstrated suggest the presence of multiple dynamic tiers of performance in U-VATS. It is not as distinct as learner, proficient, and master. After obtaining proficiency, the operative potential one can reach in U-VATS has yet to be established and will continue to be elucidated as more data are reported and added to the growing body of literature.
The longer LOS seen in the U-VATS cohort was an unexpected finding. One meta-analysis compared the two techniques and found that U-VATS was associated with significantly shorter hospital stay and equivalent rate of postoperative complications and attributed the decreased LOS to less postoperative pain, allowing patients to resume activities faster. This meta-analysis also found U-VATS to be associated with shorter duration of thoracostomy drainage. 22
Another meta-analysis by Abouarab et al. reported similar findings with shorter LOS in U-VATS and equivalent postoperative complication rate, which they also attributed primarily to less postoperative pain and duration of thoracostomy drainage. 12 However, a literature review by Akter et al. found no significant difference between the two techniques in terms of LOS or length of chest tube drainage. 26 Although there is a clear relationship between duration of chest tube drainage and LOS, this was a metric we were not able to assess in our analysis. Furthermore, many multicenter reviews commented on the lack of chest tube removal criteria and heterogeneity between hospitals on this protocol, which could ultimately affect LOS regardless of surgical technique.
The higher rate of SSI seen in our U-VATS cohort was another finding that we did not predict. It is especially perplexing given that a direct association between operative duration and increased infectious complications has been demonstrated in a previous review of VASQIP data. 27 However, the versatility and multiple functions of the single incision may also contribute to a higher risk of wound complication given the excessive manipulation from multiple instruments concentrated into one space. In a prospective comparison of the two techniques, Mier et al. found U-VATS to be associated with a higher rate of SSI, and they attributed this to the increased pressure on the surgical site and surrounding soft tissue from the multiple instruments. Their port also was used as location of tube thoracostomy. 10
Another unexpected finding was the low operative time initially from 2008 to 2010 in the U-VATS cohort, which might appear to contradict the presence of learning curve. However, this can be attributed to the low number of cases initially performed through U-VATS during that time frame. Of the 176 cases, only 10 were performed (5.6%) between 2008 and 2010. By accounting for such a small percentage, we believe that the operative time of these cases represent outliers rather than contributions to the overall trend.
There were several important limitations in our study to disclose. First, as a retrospective study, the outcomes presented are reliant on accuracy of recordkeeping and data entry into VASQIP—although the database is well validated, data entry is still subject to human error. Furthermore, there are several key variables that were not available for assessment in our database. Duration of tube thoracostomy drainage in the postoperative period was not able to be assessed as variable, which as the literature has determined plays an important role in overall LOS. Similar to many other database analyses, VASQIP does not contain outcome data past 30 days, so long-term implications cannot be interpreted.
Another important limitation, present in all large databases, is the current lack of modifying code that can be applied to VATS procedures to delineate them as U-VATS versus M-VATS, or a different variant. It is possible that within the other VA hospitals that some lung resections were performed with U-VATS technique. However, we do not believe that this proportion was large enough to significantly affect the results of our sample size of >8000 for several reasons. The adoption of the U-VATS technique has been slow, with a 2018 survey of 600 North American thoracic surgeons conducted by the Ottawa Hospital Research Institute revealing that 70% of respondents had never performed a U-VATS procedure, and only 11% had performed >50 cases. 28
Furthermore, utilization of VATS for lung resection has been shown by Maiga et al. to be slower over time in the VA system compared with the civilian sector. 29 When reviewing our own VASQIP analysis, we found that only 692 (3.2%) of all lung resections in the VA system were performed robotically, whereas the adoption of the robotic platform in civilian population was significantly higher during this time frame per Subramanian et al. 30 There is a slower adoption of new surgical techniques within the VA system, and this may be due to administrative or infrastructural differences difficult to elucidate. Therefore, although we cannot definitively exclude the possibility of U-VATS procedures existing within the M-VATS arm, we believe this number minimally affects our overall results.
A key limitation in the U-VATS arm is our utilization of 1 surgeon at one institution. Although this allows full accountability of the technique as well as analysis of cumulative case volume, it is possible there are surgeon-centric confounding factors that cannot be accounted for in our analysis and thus our results must be interpreted with caution. For example, our surgeon may perform VATS lung resections faster for technical reasons regardless of number of incisions. Lastly, the U-VATS cohort is a comparatively small sample size compared with all other VAMCs, which increases the risk of unaccounted confounders or type II error.
Conclusion
We have demonstrated superior operative duration in U-VATS lung resection versus M-VATS technique in the veteran population, which has rarely been shown in other studies. Although we did not report other superior postoperative metrics, future studies should focus on assessing whether shortened operative time can definitively improve outcomes prospectively. This study confirms the potential technical advantages that proponents of the technique have posited since its inception. U-VATS should continue to grow as an important tool in the armamentarium of the thoracic surgeon, and benefit veterans and civilians alike.
Footnotes
Authors' Contributions
All listed authors made significant contributions to the creation of this article in the following areas: study design, data acquisition/analysis, data interpretation, article drafting, and/or critical revisions. In addition, all authors have reviewed the final version and provided approval. All authors agree to be accountable for all aspects of the work including accuracy and integrity.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.