
Abstract
Background:
A limited number of publications are available in the literature regarding laparoscopic living donor nephrectomy with vaginal extraction (LLDN-VE) for kidney transplantation. The aim of this study was to compare long-term recipient outcomes of standard laparoscopic living donor nephrectomy (S-LLDN) and LLDN-VE.
Methods:
A total of 652 patients [119 LLDN-VE (18.3%) and 533 S-LLDN (81.7%)] were included in this retrospective cross-sectional study. The data related to donor and recipient demographics, surgical and anatomical characteristics, and recipient and graft status were retrieved and compared using nonparametric statistical methods. Kaplan–Meier and Cox proportional hazards regression analyses were applied to compute survival according to the surgical technique.
Results:
The mean follow-up duration was 73.0 ± 25.4 months for S-LLDN and 69.8 ± 20.4 months for LLDN-VE recipients. The main determinants of long-term outcomes were the serum creatinine (SCr) levels, death-censored graft survival, and recipient survival at the end of the post-op 5th year. LLDN-VE recipients' discharge SCr was found to be statistically lower (P = .049) than S-LLDN patients. Graft survival rates censored for death were 93.8% for the S-LLDN and 93.3% for the LLDN-VE recipients. Cox regression analysis showed significance for younger donor age (P = .010) with the application of 17 parameters, indicating better graft survival outcomes for kidney recipients with younger donors.
Conclusions:
Compared with the standard method, the long-term results of LLDN-VE are in accordance with or could even be more advantageous than S-LLDN in certain aspects. LLDN-VE appears to be a feasible, safe, and cosmetically superior approach with no negative postoperative sexual or morbid effects on the donor.
Introduction
First laparoscopic living donor nephrectomy (LLDN) was performed in 1995 and it has rapidly replaced open living donor nephrectomy (OLDN) to this date. 1 As the minimally invasive approach in the field of transplantation has become a feasible option in recent years, vaginal extraction of the donor's kidney in LLDN has become an emerging surgical technique in recent years, with the first use of it being in 2009. 2 LLDN is associated with less postoperative pain, shorter hospital stays, shorter periods of rehabilitation, and earlier return to daily work and physical activities in comparison with the OLDN. 3 Furthermore, LLDN with vaginal extraction (LLDN-VE) procures more desirable outcomes such as reduced postoperative pain, less analgesic requirements, and better cosmetic appearance. 4 In addition, no decrease in the quality of postoperative sexual life, including dyspareunia, reduction in vaginal lubrication, nor diminished pleasure was reported among the donors. 5
In accordance with the Primum non nocere doctrine, the donor, being a healthy individual, must not be harmed by the procedure. A limited number of publications are available in the literature regarding LLDN-VE for kidney transplantation. Likewise, there was no available material regarding the long-term outcomes of LLDN-VE. According to the Global Observatory on Donation and Transplantation (GODT) report, Turkey has the highest number of living kidney donors in Europe, and one of the greatest percentages all over the world. 6 Only in 2019, 3862 transplantations were performed, representing 46.4 transplants per million people in Turkey. 7
The aim of this study was to compare long-term recipient outcomes of standard laparoscopic living donor nephrectomy (S-LLDN) and LLDN-VE based on our experience as a kidney transplantation center that performs 125 transplants on average per year.
Methods
The ethical approval of this study was authorized by the Acibadem Mehmet Ali Aydinlar University's Institutional Review Board (ATADEK) on the 14th of May 2020 with the decision number: 2020-08/30. This retrospective cross-sectional study was conducted at Acibadem International Hospital Kidney Transplantation Center.
Selection and description of participants
A total of 652 patients [119 LLDN-VE (18.3%) and 533 S-LLDN (81.7%)] were included in this retrospective cross-sectional study. Age, gender, body mass index (BMI) of both donors and recipients, etiology for transplant, donor surgery type, duration of recipient follow-up (months), recipient survival, duration of graft survival and follow-up (months), acute rejection, delayed graft function, death-censored graft survival (DCGS), the relation of donor with the recipient, number of renal arteries and veins, extracted kidney side, discharge, 1st, 3rd, and 5th-year serum creatinine (SCr) levels, duration of warm and cold ischemia (seconds), donor surgery time (minutes), donor blood loss volume (mL), and the post-op recipient and donor complications were evaluated. The data were retrieved from the hospital's electronic medical records system. The patient population transplanted from female donors was included in the study. Recipients transplanted with other donor nephrectomy techniques, recipients from deceased donors, recipients with male donors, and retransplantations were excluded. DCGS was determined by the exclusion of the patients' deaths with functioning grafts. Delayed graft function was verified if the recipient had to undergo hemodialysis during the post-op first week. The demographics of the patients are presented in Table 1.
Demographics of the Patient Population
Independent-samples t-test.
Mann–Whitney U test.
BMI, body mass index; LLDN-VE, laparoscopic living donor nephrectomy with vaginal extraction; SD, standard deviation; S-LLDN, standard laparoscopic living donor nephrectomy.
Technical information (right LLDN)
LLDN procedure, a transperitoneal surgery, was performed under intratracheal general anesthesia while the kidney donor is situated in the lateral decubitus position for S-LLDN and the modified gynecological lateral decubitus position for LLDN-VE (Fig. 1). A 12 mm trocar was placed from the right lower quadrant and the abdominal cavity was dilated with CO2 on 11 mmHg pressure. A 5 mm trocar was placed 3 cm below the intersection point of the anterior axillary line and arcus costarum and another 5 mm trocar was placed laterally to the umbilicus. A 5 mm trocar was placed 3 cm superio-medially of cristia iliaca anterior superior to retract the liver. After the trocar placement, Toldt's fascia was cut and the colon medially deviated, followed by the exposure and suspension of the ureter. Following the path of the gonadal vein, tissues were dissected through Ligasure™. The renal artery and vein were dissected, and the surrounding tissues of the kidney were mobilized through Ligasure. After the complete mobilization of the kidney, the S-LLDN involves the Pfannenstiel incision to the abdomen for the extraction of the kidney, whereas LLDN-VE proceeds with the incision of the posterior cul-de-sac to allow the extraction of the kidney (Fig. 2). In the LLDN-VE, a large 15 mm Endobag™ was placed inside the abdomen through the vagina (Fig. 3). Next, the ureter was clipped and cut. The kidney was placed inside the Endobag. Afterward, the renal artery and vein were cut with a laparoscopic vascular stapler. The kidney inside the Endobag was extracted through the incised region of the vagina. The extracted kidney is perfused with a liter of cold ringer lactate solution. After the control of bleeding, a soft drain was placed on the location of the extracted kidney. Port sites were sutured with 1-0 vicryl and the skin was sutured with 3-0 rapid vicryl. The vaginal incision site was sutured continuously with 0 vicryl. The patient was transferred to the recovery room under stable conditions.
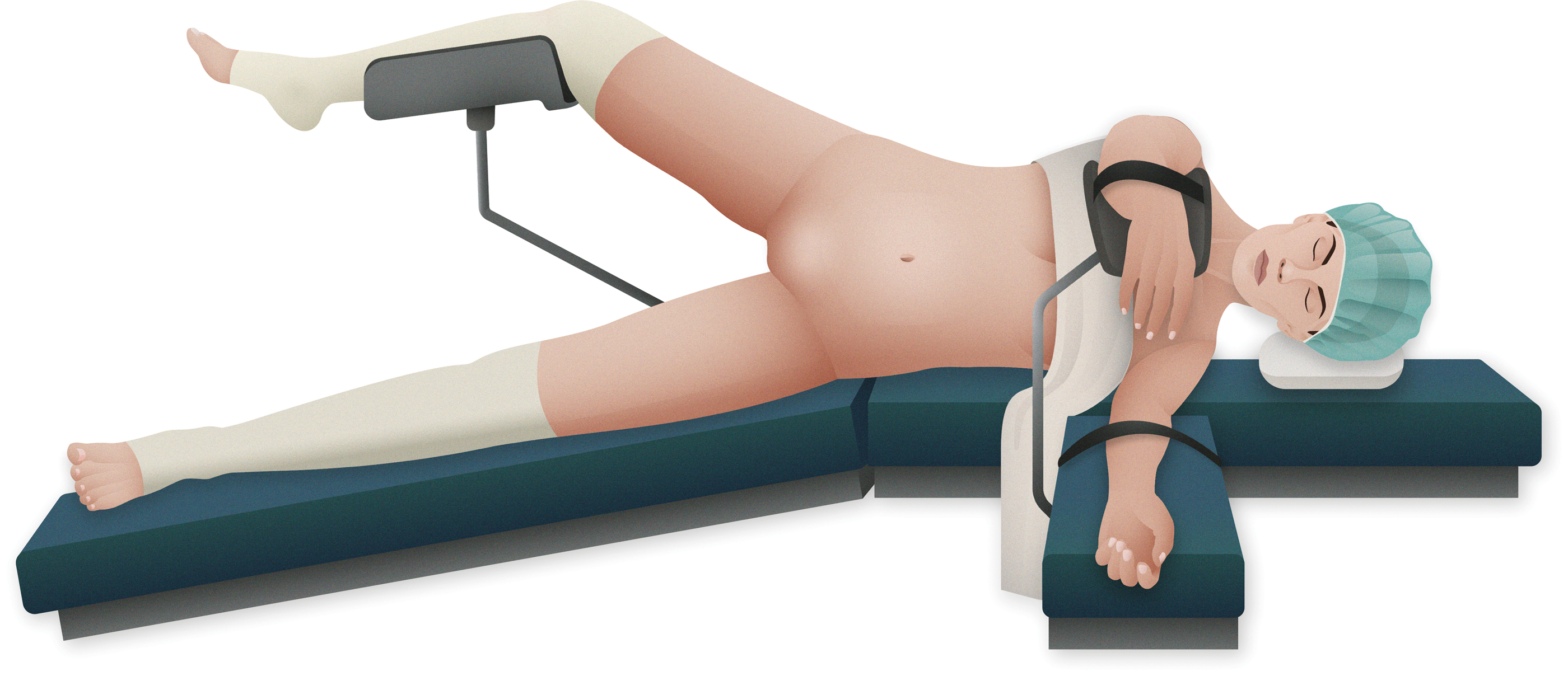
Illustration of the modified gynecological lateral decubitus position for a LLDN-VE patient. LLDN-VE, laparoscopic living donor nephrectomy with vaginal extraction. Color images are available online.
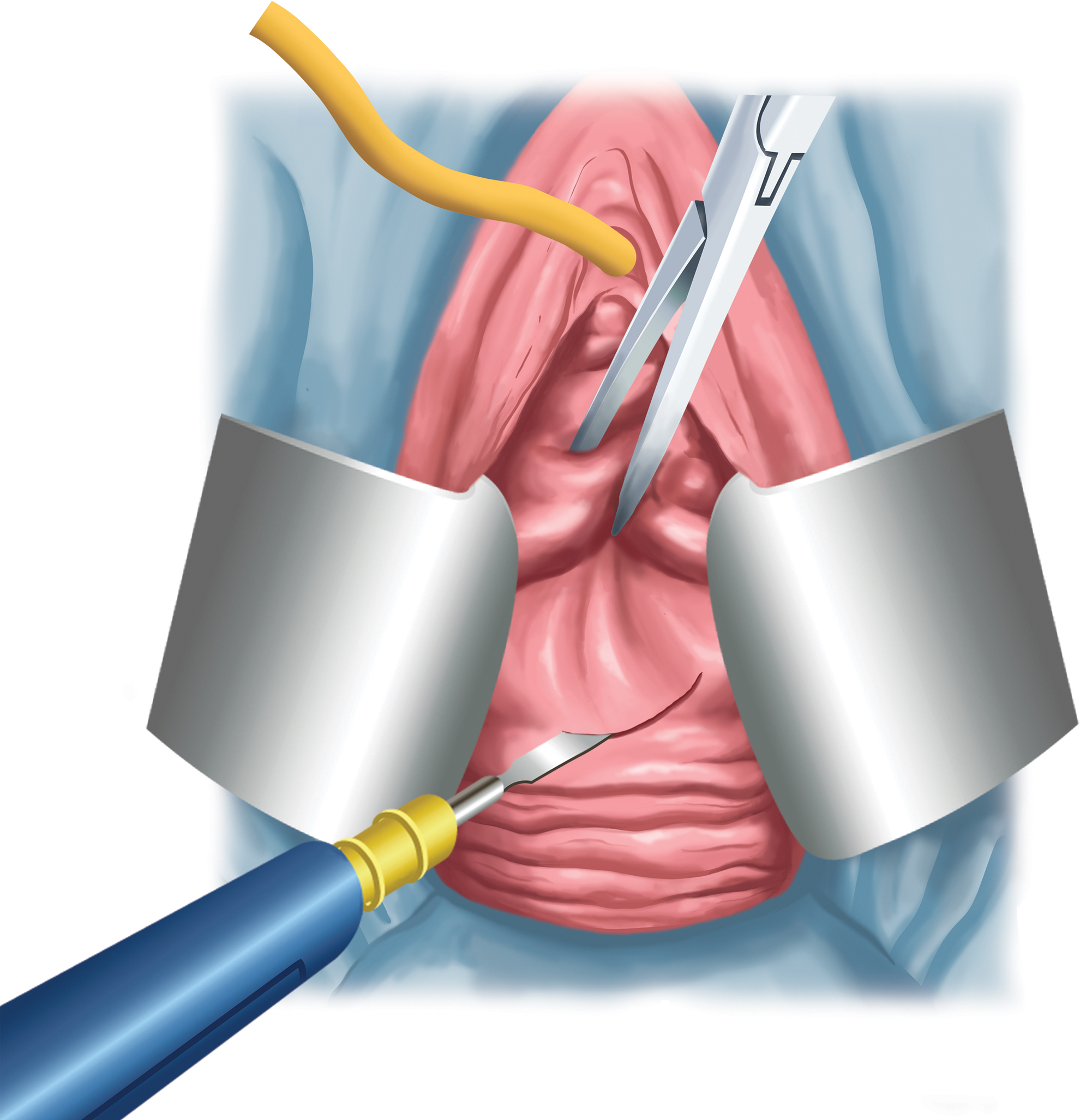
Incision of the posterior cul-de-sac for the extraction of the kidney in LLDN-VE. LLDN-VE, laparoscopic living donor nephrectomy with vaginal extraction. Color images are available online.
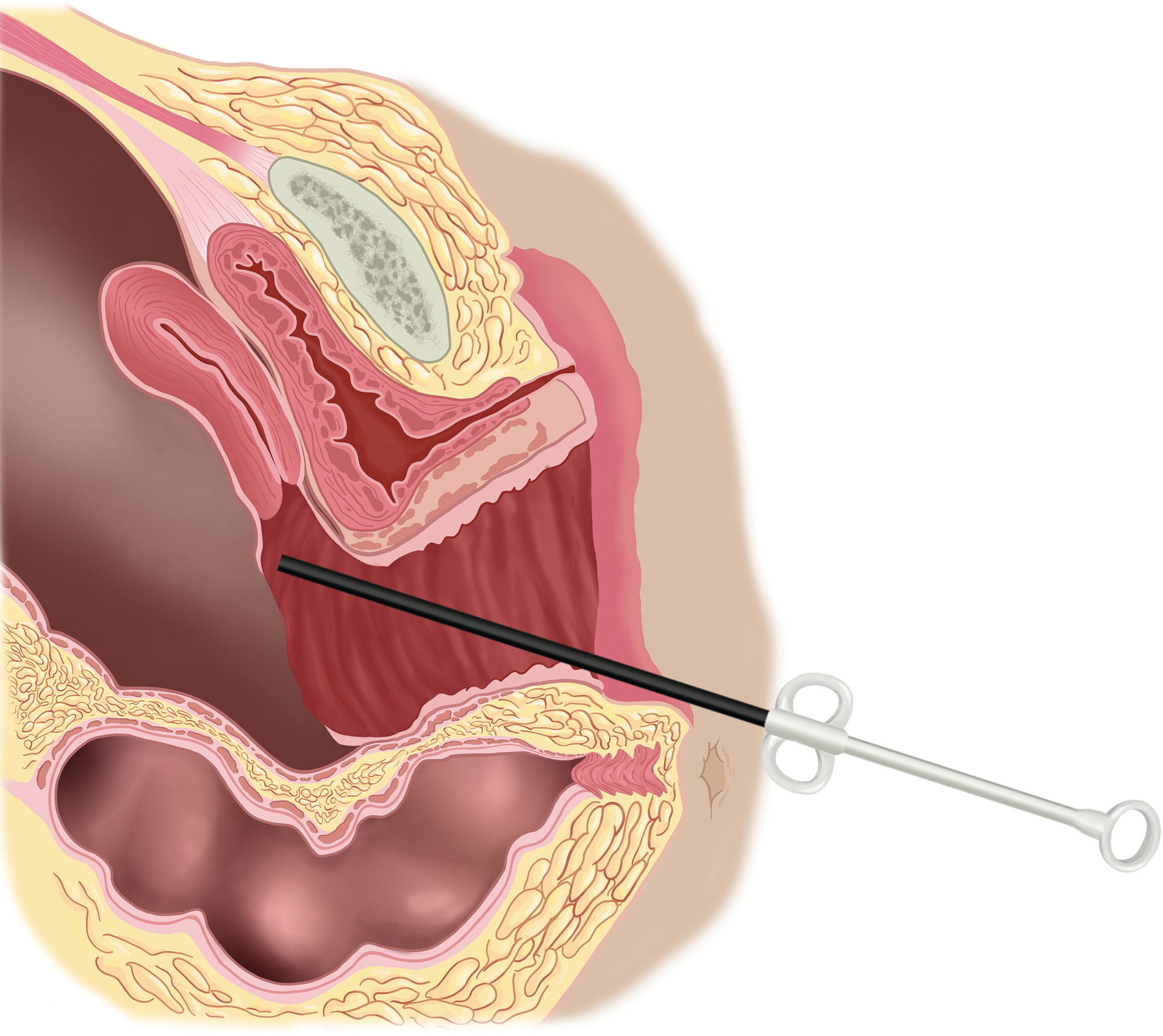
A large endobag is shown inside the abdomen through the vagina for the extraction of the kidney. Color images are available online.
Statistics
The normality test was performed with the Shapiro–Wilk test. Nonparametric statistical methods were used for values with skewed (non-normally distributed, Shapiro–Wilk P > .05) distribution. Descriptive statistics were presented using mean and standard deviation for normally distributed variables and median (and minimum–maximum) for the non-normally distributed variables.
Independent-samples t-test was used for the comparison of two normally distributed independent groups. Nonparametric statistical methods were used for values with skewed distribution. For comparison of two non-normally distributed independent groups, Mann–Whitney U test was used. The χ 2 test (Fisher's exact test) was used for categorical variables and expressed as observation counts (and percentages). Statistical significance was accepted when a two-sided P value was <.05. Kaplan–Meier analysis was used to compare graft survival censored for death with regard to both surgical techniques. Log-rank testing was used. In addition, Cox proportional hazards regression analysis was performed using 17 parameters (age, gender, and BMI of both recipients and donors, surgery type, acute rejection, delayed graft function, number of renal arteries and veins, side of the donor's kidney, warm and cold ischemia time (CIT), donor operation time and bleeding volume, and post-op recipient complication).
Statistical analysis was performed using the IBM© SPSS© Statistics Version 26.0 for Windows (Armonk, NY: IBM Corporation, released 2019).
Results
Recipient parameters
The mean age of the S-LLDN recipient population at the time of transplantation surgery was 42.7 ± 12.9 and it was 42.0 ± 12.6 for the LLDN-VE recipients. 23.6% of the S-LLDN patients were female and 76.4% of them were male; these values were measured as 15.8% for females and 84.2% for males in the LLDN-VE population. The mean BMI of the S-LLDN and LLDN-VE recipients was 24.6 ± 4.7 and 23.9 ± 4.0, respectively. Comparison of the individual demographic data of the recipients according to the surgical technique is presented in Table 1.
The basis of kidney failure in the S-LLDN recipient population was most commonly diabetes mellitus with 21.8%, followed by 18.2% hypertension and 12.7% idiopathic etiology patients. 9.1% had glomerulonephritis, 6.7% of the patients had kidney stones, and 6.1% had polycystic kidney disease as an etiology for kidney transplantation. 6.7% of patients additionally had a secondary etiology for end-stage renal disease. In this group, the mean of the discharge SCr levels were 1.5 ± 0.5 mg/dL. Delayed graft function was seen in 1.8% and 13.3% had experienced acute rejection. 10.9% of these acute rejection cases were diagnosed clinically and 2.4% of them were diagnosed according to the pathological evaluation of the kidney biopsy specimen.
The most common etiologies for kidney transplantation among LLDN-VE patients were idiopathic causes with 22.8% and hypertension with 17.5% of the patients. Diabetes mellitus, familial Mediterranean fever, glomerulonephritis, kidney stones, and polycystic kidney disease each accounted for the etiologies of 8.8% LLDN-VE recipients. 12.3% of the patients additionally had a secondary etiology. The mean of the discharge SCr levels was 1.3 ± 0.5. Lower discharge SCr levels of LLDN-VE recipients were found to be statistically significant (P = .049) when compared with the S-LLDN recipients as shown in Table 2. Delayed graft function was seen in 1.8% of the recipients and 8.8% had acute rejection, diagnosed according to the clinical presentation.
Postoperative and Long-Term Outcomes of Standard Laparoscopic Living Donor Nephrectomy and Laparoscopic Living Donor Nephrectomy with Vaginal Extraction
Value in bold text indicates a P value of <.05.
Mann–Whitney U test.
Fisher's exact test.
LLDN-VE, laparoscopic living donor nephrectomy with vaginal extraction; S-LLDN, standard laparoscopic living donor nephrectomy; SD, standard deviation.
Donor parameters
The most common S-LLDN donors were mothers with 35.2%, closely followed by spouses with 33.9%. The mean donor age at the time of transplantation surgery was 50.9 ± 13.9 years and the mean donor BMI was 30.0 ± 4.9. 80.6% of the donated kidneys were from the left side and 37.6% of them were from the right. There were several anatomical variations in the renal artery and vein numbers in the kidney donor population. 19.4% of the donors had renal artery duplication and 4.8% had renal vein duplication; 1.8% of them carried both variations at the same time. The donor operation duration mean was 147.4 ± 24.0 minutes. The mean donor blood loss was 76.8 ± 74.5 mL. Warm ischemia time (WIT) had a mean of 165.1 ± 53.9 seconds and a CIT of 48.8 ± 23.1 minutes. One donor had a post-op complication that was incisional hernia developing from the abdominal port site lateral to the umbilicus at post-op 6-months. Perioperative donor features according to the surgical technique are presented in Table 3.
Perioperative Donor Features According to the Surgery Technique
Value in bold text indicates a P value of <.05.
Mann–Whitney U test.
CIT, cold ischemia time; LLDN-VE, laparoscopic living donor nephrectomy with vaginal extraction; SD, standard deviation; S-LLDN, standard laparoscopic living donor nephrectomy; WIT, warm ischemia time.
Among the LLDN-VE population, the most common recipient–donor filiation was spouse with 38.6%, followed by mother with 31.6%. The mean donor age at the time of transplantation surgery was 49.3 ± 12.1 years in this group. LLDN-VE donor BMI mean was 29.4 ± 4.6. 91.2% of the donated kidneys were from the left side and 8.8% of them were from the right. 10.5% had renal artery duplication. There were neither variations in the renal vein anatomy nor a post-op complication in the LLDN-VE donor population. The donor operation duration mean was 149.4 ± 19.3 minutes. The mean donor blood loss was 77.2 ± 53.3 mL. WIT had a mean of 193.0 ± 51.3 seconds and CIT had a mean of 45.1 ± 17.0 minutes. WIT was found to be statistically longer (P = .0001) in LLDN-VE than S-LLDN.
Long-term outcomes
The main determinants of long-term outcomes with surgical techniques comparison in this study were the SCr levels, DCGS, and recipient survival at the end of the post-op 5th year. The mean 5th-year SCr levels of S-LLDN recipients were 1.7 ± 1.2 mg/dL and the mean of the LLDN-VE group was 1.6 ± 0.7 mg/dL without any statistical significance. Fifth-year DCGS rates were similar between the two surgical groups with 93.8% for the S-LLDN recipients and 93.3% for the LLDN-VE patients. Recipient survival rates at the 5-year follow-up showed no statistical difference; 91.6% for S-LLDN and 93.3% for LLDN-VE recipients, respectively. Statistical comparison of the long-term survival outcomes of both surgery types is represented in Table 4.
Survival Outcomes of Standard Laparoscopic Living Donor Nephrectomy and Laparoscopic Living Donor Nephrectomy with Vaginal Extraction
Kaplan–Meier survival analysis, log-rank test.
DCGS, death-censored graft survival; LLDN-VE, laparoscopic living donor nephrectomy with vaginal extraction; S-LLDN, standard laparoscopic living donor nephrectomy.
The mean follow-up duration was 73.0 ± 25.4 months for S-LLDN and 69.8 ± 20.4 months for LLDN-VE recipients. The means of the SCr values were 1.5 ± 0.7 mg/dL for S-LLDN and 1.4 ± 0.6 mg/dL for LLDN-VE patients at the post-op 1st year; later they were 1.6 ± 0.9 mg/dL and 1.4 ± 0.5 at the 3rd year. Kaplan–Meier analysis regarding patient survival and DCGS was not significant in the two groups.
Cox proportional hazards regression analysis of the complete study population of 222 patients showed significance for donor age (P = .010) with the application of 17 parameters, indicating better graft survival outcomes for kidney recipients with younger donors. Cox regression analysis for the S-LLDN group with 16 parameters (surgery type excluded) demonstrated significance for donor age (P = .007) and donor bleeding volume (P = .047); supporting the previous statement for better survival outcomes for kidney transplantations with younger donors and further pointing out the importance of lower donor bleeding volume during S-LLDN on DCGS.
Discussion
Kidney transplantation is the gold standard treatment for end-stage kidney disease with a superior post-transplant patient survival when compared with the survival during the dialysis treatment program. 8 Living donor transplants stand as a better option for recipients when a valid donor is available. Patient and kidney allograft survivals are typically better with a living donor, and surgery can be scheduled at a convenient time. As living kidney donation represents a particular situation necessitating maximum effort to minimize the surgical risk and morbidity of the donors, a radical transformation in the surgical approach of graft nephrectomy evolved for the past two decades.9,10
In the transplantation field, which might be considered as one of the most maximally invasive branches of surgery, laparoscopic approaches have started to be adopted. Even more minimal approaches are now emerging in the 21st century, the first use of laparoscopic live donor nephrectomy with transvaginal extraction of the kidney being in 2009. 2 Outcomes, especially the long-term results of this newly emerging minimal invasive approach have not been reported yet. Transplantation recipients require a long follow-up period and accordingly, new surgical techniques obligate a long duration of follow-up before becoming a standard approach in the algorithms. The mean follow-up duration in our study was 76.20 months, ∼6.3 years, which is longer than the current long-term follow-up standard of 5 years.
The discharge SCr is the best parameter that indicates the allograft function. 11 In the short-term postoperative period, discharge SCr was found to be statistically significant in favor of the LLDN-VE kidney recipients (P = .049) showing that LLDN-VE provides a better fit for the donor's kidney to the recipient. Creatinine levels at the postoperative 1st, 3rd, and 5th years are found to be lower in the LLDN-VE recipient group, although statistically insignificant. WIT seemed to be longer with statistical importance (P = .0001) in LLDN-VE when compared with S-LLDN. Longer WIT may be a risk factor for ischemia-reperfusion injury; however, the acute rejection (8.8%), 5th-year recipient (93.3%) and graft survival (87.4%) rates of LLDN-VE patients were superior to the ones of S-LLDN patients with 13.3%, 91.6%, and 86.3%, respectively; implying no quantifiable negative effect was present in this study. The 5th-year DCGS rate was .5% higher in the S-LLDN group than the LLDN-VE population, although insignificant (P = .901). Donor operation time and bleeding volume seem to be in proportion between the two groups. Cox proportional hazards regression analysis with 17 parameters showed lower donor age's significant effect on DCGS. Cox regression analysis for the S-LLDN group with 16 parameters (surgery type excluded) also demonstrated significance for donor age (P = .007), with the addition of donor bleeding volume (P = .047); indicating better survival outcomes for kidney transplantations with younger donors and showing the significance of lower donor bleeding volume in LLDN-VE on DCGS.
Allaf et al. first attempted LLDN with vaginal extraction in 2009, indicating the necessitation of larger patient cohorts and longer follow-up periods for defining the ultimate role of this approach in their case report. 2 This study has aimed to compensate for this established requirement. S-LLDN requires an additional incision for the retrieval of the donor's kidney, on the contrary, LLDN-VE does not. Thus, resulting in one less incision and a cosmetically superior approach. In addition, when compared with S-LLDN intraoperatively, LLDN-VE appears to cause less donor blood loss with minimal risk of infection transmission due to vaginal preparation, usage of endobag, and prophylactic antibiotics without an effect on the sexual function when compared with S-LLDN.12,13 Donors experience minimal abdominal discomfort, no vaginal pain, and require less postoperative analgesia with quick recovery time allowing discharge on the postoperative days 1–2. 14
Limitations of this study consist of its retrospective nature. Ideally, prospective randomized trials must be conducted to generalize the results to all clinics.
Conclusion
To our knowledge, this study stands as the first to compare the long-term results of S-LLDN with and without vaginal extraction. When compared with the standard method, the long-term results of LLDN-VE are in accordance or could even be more advantageous in certain aspects. LLDN-VE appears to be a feasible, safe, and cosmetically superior approach with no negative postoperative sexual or morbid effects on the donor.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.