
Abstract
Background:
Fetoscopic endoluminal tracheal occlusion (FETO) improves lung maturation in severe cases of congenital diaphragmatic hernia (CDH) but it does not ameliorate lung compression by herniated abdominal organs. Surgically opening the fetal abdomen (abdominal decompression [AD]) reduces the intrathoracic pressure by diverting the abdominal organs into the amniotic cavity—a probable causal therapy for lung hypoplasia and pulmonary hypertension in CDH. Open surgical abdominal decompression has been reported: we describe a minimally invasive approach in an ovine model of CDH as a probable fetoscopic intervention.
Materials and Methods:
Eight fetuses were included, 2 were kept as HEALTHY controls. A CDH (left side, liver down) was created by open fetal surgery at midgestation in 6 fetuses, 2 were taken as CDH controls. Fetoscopic abdominal decompression (fAD) was performed 21 days later in 4 animals. The fetuses were retrieved at the end of gestation and evaluated by lung stereology.
Results:
fAD led to a near total evacuation of the thoracic cavity in 2 of the 4 animals. Fetuses with CDH had a lower total volume and fraction of alveolar air space, a lower volume fraction of the parenchyma, and an increase of the volume fraction of the alveolar septa and atelectasis, as well as an increased mean thickness of alveolar septa compared with HEALTHY fetuses. Fetuses treated with abdominal decompression showed an improvement of stereological parameters.
Conclusions:
In spite of relevant limitations (pilot study, small groups, spontaneous closure of the abdominal incision) we were able to demonstrate that abdominal decompression for CDH can be performed by fetoscopy. Our results support the hypothesis of causally improving lung development by abdominal decompression, thus implying increased survival in extreme cases of CDH. A refinement of the fetoscopic techniques and direct comparison to FETO appears warranted.
Introduction
The herniation of abdominal organs into the thoracic cavity is associated with compression and subsequent underdevelopment of the lungs resulting in pulmonary hypoplasia and postnatal respiratory failure with survival rates of <10% in extreme cases of congenital diaphragmatic hernia (CDH).1–4 Research focusing on a prenatal intervention to reduce subsequent lung damage led to the development of fetoscopic endoluminal tracheal occlusion (FETO).5,6 Although FETO reduces lung hypoplasia, it does not decrease lung compression by herniated abdominal organs.3,4
Based on incidental findings of fetuses with almost no pulmonary hypoplasia in CDH and concomitant gastroschisis, the hypothesis evolved to surgically create an abdominal defect similar to a gastroschisis to let the abdominal contents escape into the amniotic cavity (abdominal decompression [AD]). 7 Improved lung development could be demonstrated in a fetal rabbit model of CDH treated with abdominal decompression and decreased pulmonary hypoplasia could also be demonstrated after abdominal decompression in a fetal sheep model of CDH.8–11 In 1994, a human case of CDH managed with abdominal decompression was reported, which survived without any damage to the exteriorized bowel. 12 However, all procedures have been performed by open fetal surgery, which is associated with relevant maternal and fetal morbidity and precludes the application of abdominal decompression. A reduction of the procedure-related risks may be achieved by an endoscopic approach.13–15 As previous studies have demonstrated, fetoscopic creation of an abdominal defect to simulate a gastroschisis could be performed safely in a fetal sheep model.16–18 Therefore, the aim of this pilot study was to establish a de novo model of fetoscopic abdominal decompression (fAD) in fetal sheep to reduce the intrathoracic pressure and improve fetal lung development in surgically created CDH.
Materials and Methods
All experiments were approved by the State Administration for animal research, Authority for Health and Consumer Protection, Chairman: Dr. Christiane Soltau, Billstrasse 80, 20539 Hamburg, Germany (project 78/12—FETAL-CDH I) and conducted in accordance with the Institutional Animal Care and Use Committee.
Fourteen singleton ewes (Ovis aries) were planned for this study. In 6 ewes, fetuses were lost during the course of the study with infections relating to a European wide outbreak of a new Shamonda-Sathuperi reassortant orthobunyavirus provisionally named Schmallenberg virus and chlamydophila abortus or unsuccessful creation of CDH. Those animals were excluded and the supplying herd and all local ewes had then to be exchanged to eliminate the infectious confounders. 19
Surgical procedures
Eight fetuses were therefore included. Two fetuses were kept as healthy controls (HEALTHY). In the remaining 6 fetuses, the diaphragmatic hernia was created by open fetal surgery at day 75 of gestation (Fig. 1). The perioperative, anesthetic, and general surgical protocols were used as reported earlier.16,17

Schematic representation of the pilot study. Color images are available online.
The diaphragmatic defect was surgically created on the left side without herniation of liver and therefore resembling a left-sided CDH with liver down. The maternal abdomen was accessed through a midline laparotomy, the uterus opened, and the fetus extracted from the head to umbilicus. A fetal thoracotomy was performed in the third lower intercostal space on the left side. The diaphragm was exposed and incised at its apex extending dorsolaterally for 1 cm. Omentum or small intestine were pulled through this defect as a placeholder or herniated spontaneously (Fig. 2). The fetal thoracotomy was closed with nonabsorbable sutures, the fetus repositioned and the uterine wall and amniotic membranes were closed by a running absorbable suture.

Creation of the CDH. The left thorax is opened by thoracotomy. The view is directed from cranial onto the left diaphragm. The ribs are retracted with a hook. A defect has been created in the apex of the diaphragm and an intestinal loop is spontaneously protruding into the thoracic cavity. The lung is held apically by the forceps. CDH, congenital diaphragmatic hernia. Color images are available online.
Two fetuses with CDH did not undergo fAD and were thus evaluated as CDH controls without fetal intervention (CDH).
fAD was performed 21 days later in 4 fetuses.16,17 Amnioinfusion and placement of the first port were performed under sonographic guidance, one or two additional ports were placed under fetoscopic guidance. The fetal incision was created in the left lower quadrant by monopolar hook cautery and the opened fetal abdomen was inspected with the endoscope.
Fetal harvest was performed on day 135 through a median laparotomy and hysterotomy. The fetus was extracted, euthanized under anesthesia applying an intracardial injection of 7.45% potassium chloride, and evaluated. The ewe was allowed to recover.
Lung stereology
Lung stereology was used to objectively quantify and describe the structural changes in the fetal lung tissue.20–22 The fetal lungs were placed in a basin and a silicon tube was inserted into the trachea. A fixation solution containing 4% paraformaldehyde, and 0.1% glutaraldehyde in 0.2 M Hepes buffer was infused into the fetal lungs through the tube at a constant pressure of 25 cm H2O over a period of 60 minutes. After fixation, the lungs were subjected to systematic uniform random sampling and the resulting samples were subsequently postfixed with osmium tetroxide, stained en bloc with uranyl acetate, dehydrated in an ascending acetone series and embedded in Technovit 7100 (Glycol Methacrylate). From 3 to 4 samples, sections of 1.5 μm thickness were cut using a rotational microtome.
The sections were placed on microscope slides and stained with Toluidine Blue. A light microscope (Olympus BX51, Hamburg, Germany) equipped with an Olympus DP72 digital camera connected to a computer with the newCAST (Computer-Assisted Stereological Tool) Software (Visiopharm, Horsholm, Denmark) was used for the stereological analysis.
The following parameters were estimated: The volume of parenchyma and volume of nonparenchyma were estimated at a magnification of × 10. At × 40 objective lens magnification, the volume of alveolar air space, the volume and arithmetic mean thickness of alveolar septa, as well as the surface area of alveolar septa were estimated. All test fields were gathered by systematic uniform random sampling and appropriate point and line grids were applied to count the interaction between the test probe (points hitting certain structures, lines intersecting with septal surface). The resulting raw counts were used to calculate the volume density (volume of a structure per unit of reference volume) and the surface density (surface area per unit of reference volume) of the parameters mentioned above according to basic stereological formulas. 22 These densities were then multiplied by the reference volume to receive absolute volumes or surface areas. The mean thickness of the alveolar septa was calculated by dividing twice the volume of septa by their surface area.
Due to the small amount of animals, the number of analyzed fetuses did not allow statistical testing.
Results
The fetoscopic access to the fetus was difficult, as previous hysterotomy for surgical creation of the diaphragmatic hernia led to chorioamniotic separation and oligohydramnios. In CDH fetuses undergoing fAD, no intestinal loops could be visualized intra-abdominally due to their displacement into the thoracic cavity (Fig. 3). Upon evaluation, spontaneous closure of the defect occurred in 2 of the 4 fetuses undergoing fAD.
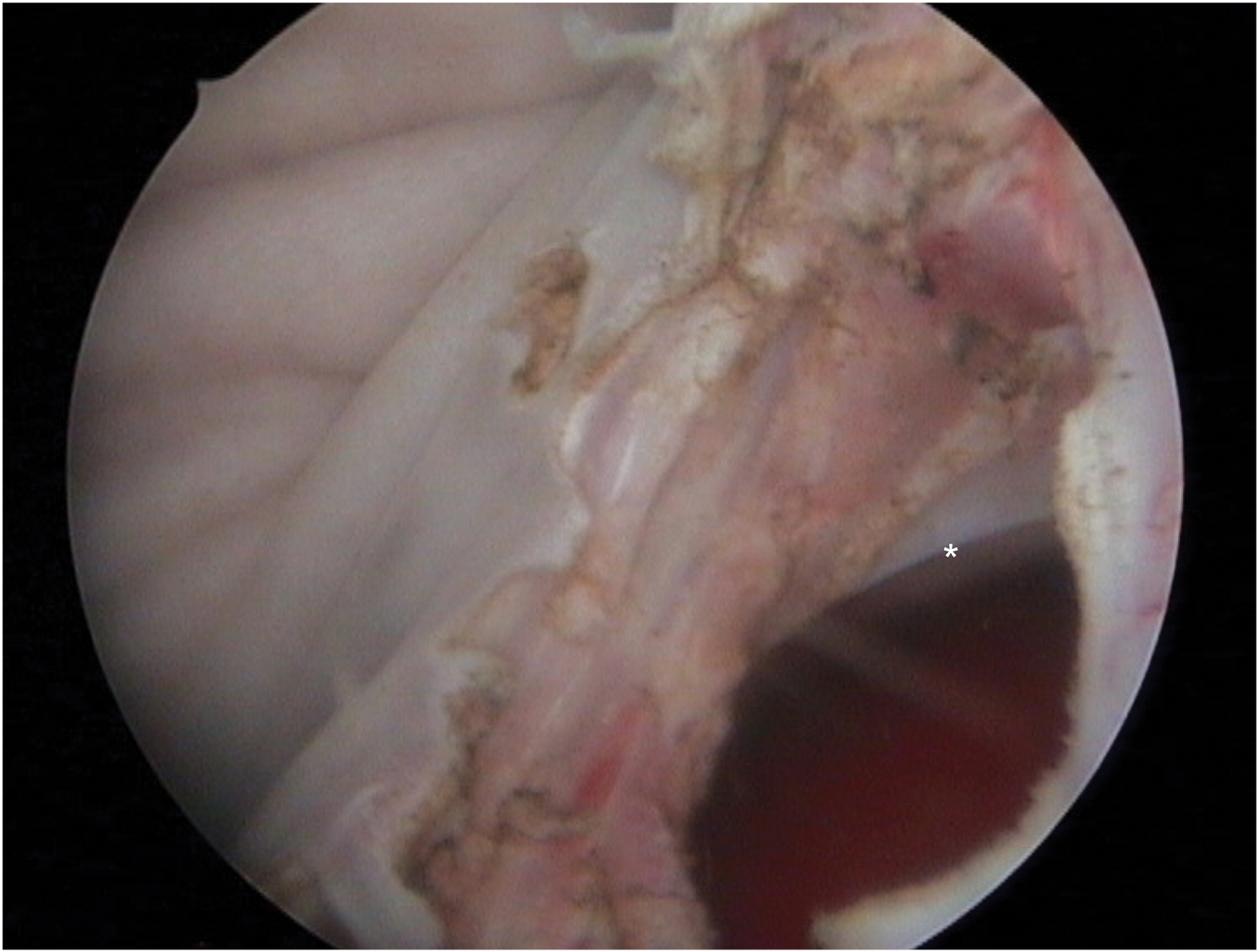
Fetoscopic abdominal decompression. An incision has been made in the left lower quadrant of the fetus. The abdominal cavity is opened and fetal laparoscopy performed: no intestinal loop can be found inside of the fetal abdomen, the asterisk (*) displays the fetal liver. Color images are available online.
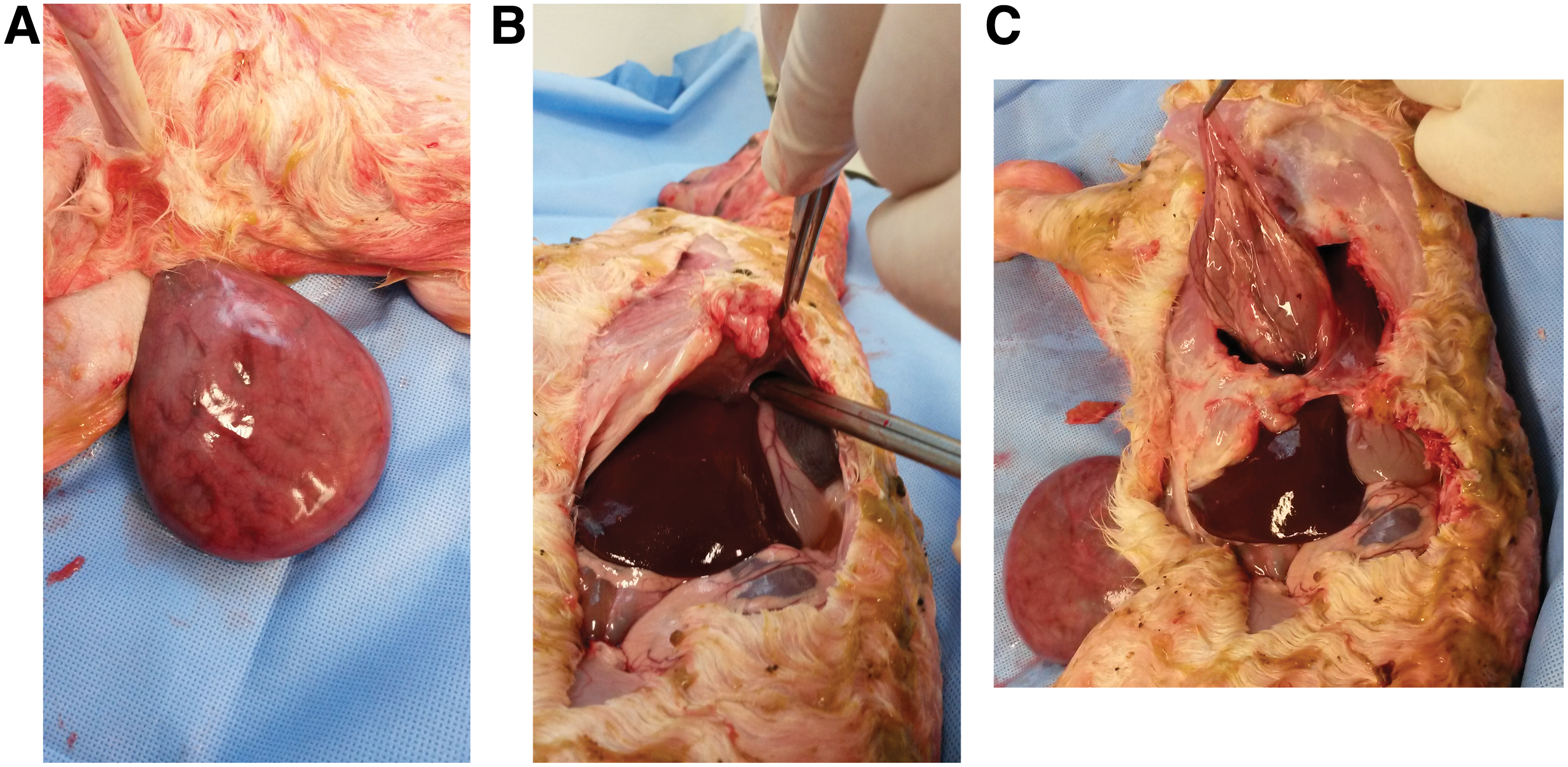
Mean fetal weight was 3681 g (HEALTHY), 3750 g (CDH), and 3744 g (fAD). The bilateral lung weight was 137.1, 68.7, and 68.8 g, respectively. Therefore, mean lung to fetal weight ratio was 3.71%, 2.02%, and 2.25%. In untreated fetuses with CDH, the left thoracic cavity was filled with loops of small and large bowel (Fig. 4A, B). fAD resulted in nearly complete extra-abdominal herniation of major parts of bowel with only small segments of stomach fixed inside the thoracic cavity (Fig. 5A–C).

Lung stereology demonstrated a decrease in parenchymal and increase in nonparenchymal parameters in the right and left lung in CDH compared with HEALTHY fetuses, whereas fetuses after fAD appeared to show an improvement of these findings (Table 1). The results of the surface area of alveolar septa for the left lung were ambiguous.
Lung Stereology
Healthy (n = 2): healthy fetuses without any surgical intervention. CDH (n = 2): fetuses with a surgically created left-sided diaphragmatic hernia. fAD (n = 2): fetuses with a diaphragmatic hernia after fAD. Values given as mean. The volume fraction is related to the lung volume (a) or volume of parenchyma (b) and nonparenchyma (c).
CDH, congenital diaphragmatic hernia; fAD, fetoscopic abdominal decompression.
Discussion
Although without statistical significance, our results are concordant with open abdominal decompression of CDH demonstrated in several animal models and one human case and therefore demonstrate the technical feasibility of the fetoscopic procedure.8–12,23 Accordingly, the theoretical advantage of fAD over FETO is the causal treatment of lung hypoplasia by spontaneous decompression of the herniated abdominal viscera with consequent adequate lung development. 11
Up to our study, abdominal decompression was only performed by open fetal surgery, which is associated with an increased maternal and fetal morbidity compared with the minimally invasive endoscopic approach in FETO. 24 Recently, a hybrid technique combining a maternal laparotomy, uterine exposure, and chorioamniotic plication with fetoscopic intervention was able to noticeably reduce the morbidity in fetoscopic management of myelomeningocele in humans. Thus, fetoscopic or hybrid fetoscopic procedures appear promising techniques for prenatal treatment of congenital malformations and so render fetoscopic application of abdominal decompression worth investigating with the potential of lower rate of uterine-related morbidity as chorioamniotic separation, premature preterm rupture of membranes, or the exclusion of vaginal delivery after open fetal surgery.13,14
Limitations
First and foremost, the small amount of animals per group precluded statistical analysis. As this study was conducted as a proof of principle and technical pilot study, the overall amount of planned animals was small (n = 14). Infection with a new Schmallenberg virus and Chlamydophila abortus led to exclusion of 6 fetuses with additional malformations or unsuccessful creation of CDH, leaving 8 fetuses for inclusion in this study. 25 Interestingly, its outbreak in Europe coincided with our experiments. 26 Our ewes were routinely tested for infectious pathogens before commencing the study, but not this virus, as it was hitherto rarely found in Europe.19,27 We agree that fetal loss may have been triggered by the fetoscopic procedures. But as those aborted fetuses showed severe additional malformations related to and tested positive for the Schmallenberg virus or Chlamydophila abortus, they were excluded. Nevertheless, our results are in concordance with the reports after open fetal surgery. Additionally, stereological analysis suggests improved lung parameters after fAD. But any conclusion may only be drawn after larger studies, preferably comparing FETO with fAD, have been conducted.
The rate of spontaneous closure of the abdominal defect (2 out of 4) appears too high, which was not documented in other published reports.8–11 Whether this is attributed to the pilot character of the study, where the size of the incision has not been standardized and therefore is of variable length in the 4 animals, or a general limitation of the technique—the incision was set with monopolar hook cautery without a placeholder in the defect—can only be examined in larger series. It appears of interest to note that fetoscopic abdominal incision by monopolar hook cautery led to the formation of a gastroschisis-like defect without any relevant rate of spontaneous closure in ovine fetuses without CDH in earlier studies conducted by us. 17 In the current study, no intestinal loops were found inside the opened abdomen in CDH fetuses, demonstrating the rapid displacement of the intestine into the thoracic cavity 21 days after surgical creation of the defect. This effect of a “low resistance alternate path” for the bowel in CDH was first demonstrated by Montgomery et al. in 1995. 11 In fetuses with CDH, the thoracic cavity exhibits a lower pressure compared with the abdominal cavity. Therefore, the pressure onto the abdominal incision by the growing intestine appears to be reduced in CDH compared with non-CDH fetuses from our earlier reports and may therefore explain the higher rate of spontaneous closure of the defect in CDH fetuses. Nevertheless, after fAD, the lower pressure is in the amniotic cavity, thus leading to the exteriorization of the intestines. Whether any placeholder in the abdominal defect, as suggested by Langer et al., or modification of the incisional length or technique will decrease the rate of spontaneous closure has to be evaluated. Ideally, this placeholder could be combined with a bag to protect the bowel from the amniotic fluid as recently suggested by us.28–36
The severity of the pulmonary hypoplasia generated is variable and may range from mild to severe, mostly depending on the size of the diaphragmatic hole and the state of the liver (up versus down). All hernias created in this study were left sided with liver down and the size of the diaphragmatic incision was 1 cm. Any widening of the diaphragmatic defect during further gestation may lead to different sizes of the hernia, but we anticipated a sufficient standardization of the size of the generated hernia in this pilot study. Furthermore, in all CDH fetuses, the whole intestine was displaced into the thoracic cavity with none left inside of the abdomen.
Nevertheless, another probable limitation of this study is the creation of liver-down CDH compared with liver up, as the cases of CDH with less favorable outcome often present with liver up. Therefore, fetuses which might need prenatal intervention the most are those with liver up. Consequently, an animal model with liver-up CDH will be the most adequate. It was our intention to test the overall technical feasibility and probable effect of fAD in CDH in a step-up model of complexity. We, therefore, sought to use an animal model in which a CDH could be created without relevant morbidity: We did not want any morbidity or complications of liver-up CDH to interfere with the results of the fetoscopic approach. As we tried to keep the CDH creation as reproducible and simple as possible we started with surgical creation of the defect by incising the left diaphragm at its apex and extending dorsolaterally, resulting in a liver-down CDH. In a follow-up study, we plan to compare the effect of fAD and fetoscopic tracheal occlusion between fetuses with liver-down and liver-up CDH.
However, we were currently not able to simulate extreme cases of CDH with right-sided hernias and liver up, which are the preferable target for fetal intervention—this model will still have to be established in ovine fetuses. 37
Fourth, a probable uncontrolled herniation of abdominal contents other than bowel through the abdominal incision, which might lead to infarction of spleen or liver resulting in potential devastating complications has to be discussed. 23 Whether this can be prevented by specific incisional lengths, placeholders, or bags has to be evaluated in further animal studies.
Limiting the fetoscopic procedures were oligohydramnios and chorioamniotic separation resulting from open surgical creation of the CDH, which impeded fetoscopic access and manipulation, thereby increasing operating time and the risk for complications in our study. This effect is expected to be reduced in the human fetus and uterus, as it has not been operated on before. Correspondingly, a higher rate of premature rupture of membranes and fetal death has been found in cases with previous uterine surgery and, therefore, a previous hysterotomy was an exclusion criterion in the MOMS-trial. 15
Another limitation of this study is that fAD is not compared with the current standard of experimental fetal treatment for CDH, FETO. We planned this pilot study to test the feasibility of fAD, which has not been performed before. If not technically feasible, any comparison to FETO would not be necessary. But as we were able to demonstrate an effect of successful fAD, our next step is to compare this technique to FETO.
Ultimately, the creation of an abdominal wall defect by abdominal decompression is associated with additional risks, such as strangulation of the protruding organs or their inflammatory damage—similar as seen in gastroschisis—which will add up to the morbidity and mortality of the diaphragmatic hernia as a relevant limitation of this procedure. Although the anticipated mortality of an abdominal wall defect, hypothesized to be comparable to a gastroschisis, is significantly lower than in extreme cases of diaphragmatic hernia, one has to take those into account as any prenatal therapy should put neither fetus nor mother at relevant procedure-related risks.11,16,18 If the survival of <10% in extreme cases of CDH can be significantly increased by fAD, any small increase of the abdominal defect-related morbidity might appear justifiable. Those data will only be obtained by further animal studies. Nonetheless, any abdominal decompression-related fetal loss is inacceptable for human application.
In summary, while our results demonstrate that fAD appears possible, they do not validate an improvement in outcomes of fetuses with CDH. Therefore, drawing any conclusions toward the human application of fAD is obsolete until further data of comparative animal trials are available. Nevertheless, the preliminary results are encouraging and to be developed.
Conclusion
Although with relevant limitations in this pilot study (small groups and spontaneous closure of the abdominal incision after fetoscopic decompression) we were able to demonstrate the technical proof of principle that abdominal decompression for CDH can be performed fetoscopically, leads to near total evacuation of the thoracic cavity, and appears to improve lung development in our model of CDH (left side, liver down).
Depending on the results of the ongoing TOTAL-Trial (FETO) and the development of pharmacologic fetal therapy for CDH, the role of fAD as a causal therapy for lung hypoplasia might have to be discarded or reconsidered.37,38 An animal study comparing fAD with fetal endoscopic tracheal occlusion, pharmacologic fetal therapy, and watchful waiting should be the next step to establish the best possible prenatal treatment for extreme cases of CDH.
Footnotes
Authors' Contributions
R.B. designed the study, conducted the experiments, anesthesia, and surgical procedures and wrote the article. F.F. assisted in the surgical procedures, conducted the stereological examinations, and wrote the article. C.M. designed the stereological examinations and critically revised the article. M.B. assisted in the surgical procedures and critically revised the article. K.W. assisted in the anesthesia and surgical procedures and critically revised the article. B.T. gave veterinarian support, performed the impregnation of the ewes, and critically revised the article. K.R. critically revised the article. T.K. designed the study, conducted the experiments, anesthesia, and surgical procedures and critically revised the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
R.B and T.K. received funding by Karl Storz Company GmbH, Tuttlingen, Germany, in the form of materials (Storz Camera Telepack. Storz 3- and 5-mm laparoscopic instruments).