
Abstract
Laparoscopic total abdominal colectomy (TAC) is the optimal operative approach for patients with medically refractory inflammatory bowel disease and other benign colon conditions. Minimally invasive techniques for TAC are safe, appropriate, and associated with faster recovery than open surgery. This may be of particular importance in patients who ultimately undergo proctectomy with or without intestinal pouch reconstruction. We describe approaches to the laparoscopic TAC.
Introduction
Total abdominal colectomy (TAC) or total proctocolectomy (TPC) is the mainstay of surgical management for ulcerative colitis (UC) and colonic Crohn's disease (CD) when the disease becomes refractory to medical management or associated with complications. 1 In both situations, patients commonly suffer severe physiologic compromise, poor nutrition, and potentially higher surgical risks for anastomotic leak, wound infection, or other worrisome perioperative complications. Additional indications for surgery in patients with UC or CD include malignancy, dysplasia, medically refractory disease, intolerance to medications, steroid dependence, and failure to thrive in children and adolescents. 1 Once the decision for surgical treatment is made, the surgical options of a single-stage TPC or a staged approach with TAC followed by proctectomy with or without intestinal pouch reconstruction must be considered. 2 Factors for consideration of one-stage TPC versus staged TPC with or without intestinal reconstruction may depend on patient sphincter integrity, prior perianal disease, nutritional status, immunosuppression and steroid use, and overall comorbid health conditions. 3
TAC with end ileostomy is an appropriate initial surgical approach for many patients with medically refractory UC or CD.3,4 The proctectomy portion of the TPC surgery is often performed as a delayed second stage in patients with medically refractory disease due to increased rates of pelvic complications, wound healing, and infectious processes when performed during the initial TAC for medically refractory disease. Other patients may pursue elective TAC instead of TPC because of concerns about fecundity after proctectomy or concerns about quality of life with an ileostomy versus an ileal pouch–anal anastomosis (IPAA). 5 Minimally invasive TAC across these settings is safe, effective, and often associated with improvements in postoperative recovery over open surgery.6,7 In patients wherein restoration of intestinal continuity is a suitable future option, leaving the rectum in place preserves the anatomic planes for future proctectomy. In one study of 108 patients undergoing TAC for severe colitis at an academic medical center, the majority of patients (65.7%) subsequently underwent proctectomy with IPAA creation. 5 However, national data including >140 academic medical centers and their affiliates suggest that only one-third of patients may undergo IPAA creation after proctectomy. 8 Whether the patient eventually undergoes a restorative IPAA or not, the initial approach with minimally invasive TAC is critically important to the treatment of UC.
We aim to describe our technique for the totally laparoscopic incisionless TAC, most often performed for surgical therapy in the setting of UC. Although laparoscopic TAC with a utility incision for specimen extraction is common either through a hand-assisted laparoscopic approach or creation of the utility incision after laparoscopic mobilization, we share our experience with the totally laparoscopic incisionless TAC. This approach may offer benefit to select patients to reduce pain and rates of wound infection.
Preoperative Phase
Enhanced recovery protocols (ERPs) are incorporated into the care of all elective and urgent colon and rectal surgery patients. For patients in the elective setting, medical optimization, smoking cessation, alcohol cessation, and nutritional prehabilitation are employed as feasible. 9 We prescribe a protein-rich diet for 1 week before surgery and a carbohydrate-loading beverage the night before and the morning of surgery. Patients can intake clear liquids until 2 hours before surgery. Preoperative antibiotics, chemical venous thromboembolism prophylaxis, postoperative nausea and vomiting prophylaxis medications, and preoperative multimodal analgesia including the use of a nerve block or intrathecal opioid injection are also employed. A close and collaborative relationship during surgery with the anesthesiologists helps to ensure optimal fluid administration intraoperatively.
Positioning and Trocar Placement
The patient is placed supine on a “pink pad,” or other material to prevent sliding on the operating room table, and a securing strap or tape is placed across the chest. A Foley catheter and orogastric tube are placed. Both arms are tucked, and the legs are in the modified lithotomy position with knees flexed. Ports are placed in the right lower quadrant, left upper quadrant, left lower quadrant, suprapubic, and supraumbilical areas. All ports can be 5 mm in diameter except for one 12-mm port for the endoscopic stapler in either the right-sided or supraumbilical ports. Our preference is to use the right lower quadrant port for the stapler, positioned at the site marked for the end ileostomy. Figure 1 demonstrates the placement of the laparoscopic trocars.
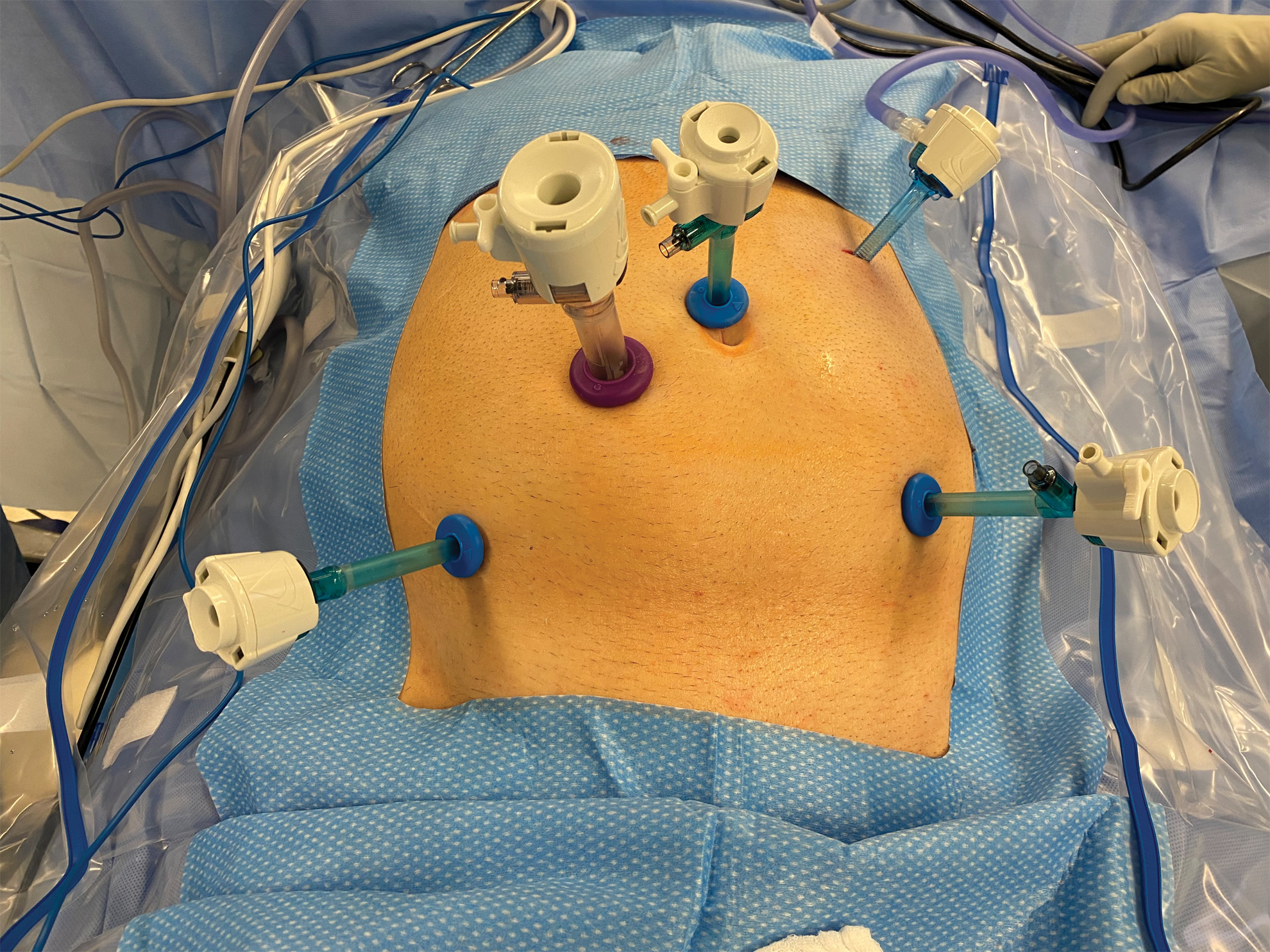
Placement of trocars. An additional suprapubic trocar or right upper quadrant trocar may be placed if needed. Color images are available online.
Surgical Technique and Operative Steps
With the patient in steep Trendelenburg and right tilt, the surgeon stands on the patient's right side. We begin with lateral mobilization of the left colon as long as no heightened suspicion exists for malignancy elsewhere based on preoperative colonoscopy or imaging. To adequately visualize the left colon mesentery, the omentum of the transverse colon is swept cranially, and the small bowel is moved to the patient's right side. We mobilize the white line of Toldt laterally starting at the distal descending colon and sigmoid colon, moving proximally toward the splenic flexure. Providing adequate tension proximal to your energy source is immensely helpful for exposing the proper plane that is usually closer to the colon than one thinks. After dividing the lateral attachments, the mesentery is entirely medialized to the midline in this lateral to medial manner. Next, to fully mobilize the splenic flexure, we continue by entering the lesser sac from behind the splenic flexure if possible. In addition, the omentum is splayed anteriorly above the midtransverse colon and an energy source is used to enter the lesser sac more proximally, being careful to not divide the omentum full thickness. Once the posterior wall of the stomach is identified, the omentum is detached from the distal transverse colon to the splenic flexure and the distal dissection plane is met. Any remaining attachments to the retroperitoneum by the splenic flexure are now divided, being careful to stay anterior to the pancreas. Less steep Trendelenburg patient positioning and surgeon positioning between the legs are often necessary as one approaches the splenic flexure mobilization.
In the case of oncologic concerns, the initial left colon dissection proceeds in a medial to lateral manner by first identifying the inferior mesenteric vein (IMV) at the ligament of Treitz. With an energy source, the peritoneum parallel to the IMV is scored to develop the potential space between the left colon mesentery and the retroperitoneum. If the correct plane is developed, this blunt dissection should be relatively bloodless. An instrument elevates the IMV and the retroperitoneum can be bluntly pushed dorsally, while dissection continues beneath the colon and toward the splenic flexure. The IMA or left colic artery can be identified and ligated in a similar manner, preserving the ureter and gonadal vein in the retroperitoneum, by scoring the peritoneal and performing blunt dissection to push the retroperitoneal structures posteriorly. The lateral attachments are then released, and the splenic flexure is mobilized as already described.
Next, the remaining omental attachments to the transverse colon are released with the energy source to the level of the falciform ligament or to the most proximal extent of the transverse colon that can be reached with ease. Attention is then turned to the right colon and terminal ileum. The surgeon moves positions to stand on the patient's left side. The table is adjusted to move into Trendelenburg with the right side elevated. The small bowel is swept down into the pelvis to expose the right colon mesentery. The ileocolic pedicle is identified and elevated. The peritoneum just below the pedicle is scored, and the plane between the right colon mesentery and the retroperitoneum is developed. Again, if the surgeon is in the correct anatomic space, this should be relatively bloodless. It is critical to identify the duodenum and ensure it is kept posteriorly during the dissection. This plane is carried out as far laterally and superiorly as possible until reaching the wall of the colon at the ascending colon and the hepatic flexure. To take the ileocolic pedicle, a window is created on either side of the vessel and then ligated with an energy device. For a patient with known calcified vessels, a vascular load stapler can be considered. An endoloop should be readily available when taking a named pedicle with an energy device and a laparoscopic grasper in position to grasp the proximal end of the vessel in the event of a misfire or incomplete seal. The energy source is then used to divide the mesentery of the terminal ileum for 5–10 cm toward the terminal ileum. The small intestine is then reflected cephalad so the lateral attachments of the ileum can be released and the remaining ileal mesentery attachments to the retroperitoneum can be divided. By grasping the appendix, the assisting hand provides persistent tension for easy lateral mobilization of the colon to the hepatic flexure. The hepatic flexure is completely mobilized by continuing the lesser sac dissection plane from the mid transverse colon toward the hepatic flexure. With the colon fully mobilized and the ileocolic pedicle ligated, the energy device divides the mesentery of the hepatic flexure and the proximal transverse colon. Caution should be undertaken to ensure no tension exists on the middle colic vessels during division. These are often ligated initially with the transverse colon reflected anteriorly, and once more mobilized, the transverse colon is retracted caudally, and an assistant hand lifts the mesentery away from the small bowel underneath. The mesentery is further divided working distally to reach the splenic flexure. A window is then created in the distal sigmoid colon mesentery with mesenteric ligation moving from distal to proximal. It is usually prudent to leave the dissection plane of the upper rectum virgin in preparation for subsequent proctectomy.
The sigmoid colon is divided using the endoscopic stapler with 3 to 4 mm staple heights. At this point, it is critical to ensure that the colon is fully divided and mobilized and to ensure hemostasis. Once the operative field is fully inspected for completeness, the distal colon specimen staple line is grasped and locked as shown in Figure 2. Next, the right lower quadrant 12 mm port is removed, and a small wound protector is placed. Using the laparoscopic grasper, the specimen is delivered through the 12 mm port site and transection of the ileum occurs with a stapling device. Next, we reinflate the abdomen and ensure the correct orientation of the ileum without twist. Ports are removed, and the ileostomy is matured. Figure 3 demonstrates the final appearance of the abdomen at the conclusion of the case.
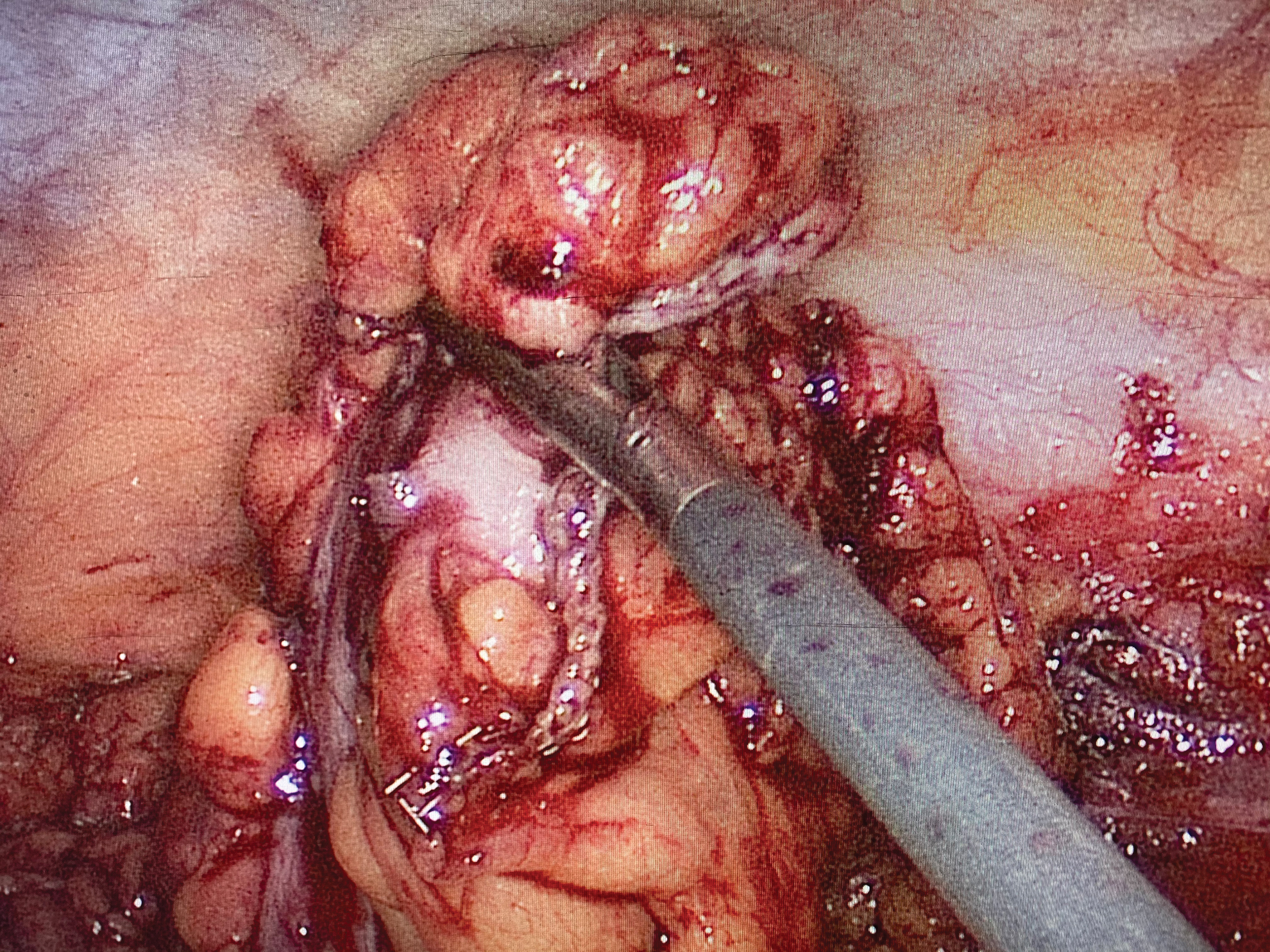
Grasping the distal resection staple line. Color images are available online.

Final appearance with ports closed and matured ostomy. Color images are available online.
Variation for TPC with end ileostomy
For a TPC, the mobilization proceeds in a similar manner, however, continues distally past the sigmoid colon along sacral promontory into the pelvis. After retracting the rectum anteriorly and superiorly, we open the peritoneum laterally on either side opening the presacral space, connecting posterior to the rectum. The superior hemorrhoidal artery is divided. Posterior and lateral dissection moves toward the pelvic floor while preserving the hypogastric nerves, until the presacral fascia joins with the fascia propria. Anteriorly, the rectum is separated from Denonvilliers' fascia. Closer rectal dissection through the mesorectum is an alternative approach, although timelier and with higher potential blood loss due to the vascular mesorectum. Once the rectum is fully mobilized circumferentially, the terminal ileum is divided with an endoscopic stapler. The nonspecimen end of the small bowel is similarly brought through the 12 mm right lower quadrant port for end ileostomy creation as previously described. Next the surgeon begins the perineal approach and performs an intersphincteric dissection until reaching the pelvic dissection plane and removes the entire specimen through the perineal defect. The perineum is closed in multiple layers of absorbable suture; the ileostomy is again checked laparoscopically for appropriate mesenteric orientation, and the operation concludes with pelvic drain placement, port site closure, and ileostomy maturation.
Single incision laparoscopic and robotic TAC
In addition to standard laparoscopic surgery, TAC is also possible using alternative minimally invasive approaches such as single incision laparoscopic surgery (SILS) and robotic-assisted laparoscopic surgery. SILS cholecystectomy and appendectomy were performed by general surgeons as early as 1997; however, technical challenges limited extensive adoption. Advancements in articulating instruments, laparoscopes, and specially designed multilumen ports in the early 2000s helped popularize SILS due to overcoming some of the inherent technical challenges. 10 Fichera et al. describe their approach to SILS TAC using the GelPoint® Advanced Access Platform (Applied Medical, Rancho Santa Margarita, CA). 11 They place three 5-mm ports and one 12-mm port through the GelPoint at the preoperatively marked ileostomy site and proceed with right colon medial to lateral dissection with division of the ileocolic pedicle followed by hepatic flexure, transverse colon, splenic flexure, and descending colon. As with standard laparoscopic approaches, utilizing Trendelenburg, reverse-Trendelenburg, and left-right tilt is imperative to enhancing operative exposure. Also, the GelPoint SILS port can be rotated to adjust the orientation of the trocars and camera depending on the portion of the dissection. Lastly, the division of the sigmoid colon with the EndoGIA stapler allows for extraction of the specimen and extracorporeal division of the terminal ileum. The terminal ileum is matured as an ileostomy at the extraction site, resulting in no visible incisions after colectomy.
Robotic TAC using the da Vinci Si (Intuitive, Sunnyvale, CA) required rotating and redocking the robot to access all four quadrants of the abdomen, adding unnecessary time and complexity. The da Vinci Xi (Intuitive), however, has a rotating boom that greatly facilitates multiquadrant colorectal surgery such as TAC and total abdominal proctocolectomy without repetitive redocking.12,13 In addition, the added feature of pairing the operative table to the robotic platform allows for typical position changes during surgery without the need for redocking the robot. Details for the optimal robot location relative to the patient (left side, between the legs, etc.) and port placement are beyond the scope of this review, and the literature is quickly growing with various approaches to efficient robotic multiquadrant colorectal surgery.
Postoperative Management
Patients in the elective or semielective setting can often be managed with ERPs.9,14 We provide a clear liquid diet immediately postoperatively to all patients and provide early access to easily digestible regular food as soon as ileostomy effluent begins. The Foley catheter is removed on the first or second postoperative day depending on history of urinary retention or prostatic hyperplasia. A transanal drain (such as a Malecot) is left in the rectum for 3 days postoperatively for decompression if the rectum is very inflamed. One month of outpatient venous thromboembolism prophylaxis after TAC for patients with medically refractory inflammatory bowel disease is provided and has been shown to be cost-effective. 15
Complications
After laparoscopic TAC, several complications can occur. The most common complication is ileus, occurring in up to 18% of patients pooled from both open and laparoscopic approaches. 16 Other reasons for slow return of bowel function include twisting of the ileostomy at creation that ultimately causes bowel obstruction. 17 Cross-sectional imaging may reveal bowel obstruction at the ileostomy site with difficulty inserting a flushing catheter (Foley, red rubber, etc.) through the ileostomy. Revision of the ileostomy is mandatory. Other important considerations for patients not progressing as expected include the integrity of the staple line at the proximal rectum and the development of pelvic sepsis. In addition, the risk of venous thromboembolic disease may be higher in patient with inflammatory bowel disease. 18 Patients may have other common postoperative infectious processes such as urinary tract infection and skin and soft tissue infection, which can be minimized by optimal postoperative care.
Conclusions
The laparoscopic approach is highly desirable in patients who are likely to undergo restorative proctectomy with pouch creation, or proctectomy alone, as reoperation after laparoscopic surgery will be less arduous than those with prior open surgery. For patients, recovery from minimally invasive surgery is associated with less pain and shorter hospital stays.
Footnotes
Authors' Contributions
R.A.T. drafted the article, prepared image, revised the article, and gave final approval of the article.
J.H.-M. drafted the article, revised the article, and gave final approval of the article.
A.R.W. prepared image, revised the article, and gave final approval of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding for this paper.