
Abstract
Objective:
To investigate the efficacy and safety of cold snare endoscopic mucosal resection (CS-EMR) and hot snare endoscopic mucosal resection (HS-EMR) for colorectal polyps with diameters of 6–9 mm.
Methods:
Retrospective analysis was performed on the clinical data of 485 patients with colorectal polyps (6–9 mm in size) who were treated with CS-EMR or HS-EMR in the endoscopy center of Hangzhou Third People's Hospital from January 2017 to December 2019. Colorectal polyps were lifted by submucosal injection of normal saline. The CS-EMR group used a cold snare to remove the lifting polyps, while the HS-EMR group used a hot snare. Propensity score matching analysis with 1:1 matching and the nearest neighbor matching method were performed to ensure well-balanced characteristics of the CS-EMR and HS-EMR groups. Matching factors included age, gender, body mass index, blood routine, coagulation indicators, polyp site, size, number, and morphology. This resulted in a balanced cohort of 128 patients per group. Polyp recovery, complications, clipping for disclosure, and length of hospital stay were compared after matching. t-Tests, χ2 tests, McNemar's tests, and Fisher's exact test were used for comparison between the two groups before and after matching.
Results:
There were no differences between the two groups of intraoperative and postoperative bleeding (P > .05), but the CS-EMR clipping rate was lower than the HS-EMR group (P < .01). There was a higher incidence of post-polypectomy syndrome (PPS) (P = .03) and longer hospital stays (P < .01) in the HS-EMR group than the CS-EMR group.
Conclusions:
Compared with HS-EMR, CS-EMR is more convenient to operate, with a low incidence of PPS, clipping rates, and short hospital stays. It is a safe and effective removal method for 6–9 mm colorectal polyps.
Introduction
A colonoscopy is the main screening method for colorectal polyps. Intestinal polyps are responsible for 60% to 80% of colorectal cancer. Therefore, timely removal of intestinal polyps can effectively reduce the incidence and mortality of colorectal cancer.1–3 Polyp resection methods are used, such as biopsy forceps, hot biopsy forceps, snare, endoscopic submucosal dissection, and endoscopic mucosal resection (EMR). Each has advantages and disadvantages. Various polypectomy techniques and devices are available, and their use often vary based on endoscopists' preferences and equipment availability. There is consensus on the optimal endoscopic treatment for 6–9 mm colorectal polyps. The existing studies are single-center randomized controlled studies.4–6
This study collected 485 cases of 6–9 mm colorectal polyps treated by cold snare endoscopic mucosal resection (CS-EMR) or hot snare endoscopic mucosal resection (HS-EMR) in our endoscopy center from January 2017 to December 2019. The data were matched by propensity score matching (PSM), and the relevant indexes after matching were analyzed to compare the safety and efficacy of CS-EMR and HS-EMR. This was done to objectively evaluate the clinical efficacy of the two methods and provide a higher level of evidence-based medical guidelines for patients. PSM can effectively reduce the confounding effect, balance the difference of confounding factors between groups, and improve the statistical efficiency. 7
Patients and Methods
Patients
A total of 485 patients with 6–9 mm colorectal polyps treated by CS-EMR or HS-EMR in the endoscopy center of Hangzhou Third People's Hospital from January 2017 to December 2019 were selected. Inclusion criteria were as follows: (1) age 18–80 and (2) single or multiple colorectal polyps with diameters of 6–9 mm, with Paris classification as 0-Ip, 0-Isp, 0-Is, and 0-IIa (Table 1). Exclusion criteria were as follows: (1) unqualified bowel preparation (Boston bowel preparation scale, BBPS <6); (2) incomplete colonoscopy; (3) platelet (PLT) <80 × 109/L or the prothrombin time (PT) >1.4 times, taking antiplatelet therapy or anticoagulant drugs; (4) polyp diameter <4 mm or >9 mm; (5) inflammatory bowel disease, familial adenomatous polyposis, or identified colorectal cancer before surgery; and (6) polyps not removed by CS-EMR or HS-EMR. There were 162 patients in the CS-EMR group and 323 patients in the HS-EMR group. All patients signed informed consent before surgery. The Medical Ethics Committee of Hangzhou Third People's Hospital approved the study.
The Paris Classification of Superficial Neoplastic Lesions
Operation method
CS-EMR group: submucosal injection of normal saline was performed with an injection needle, and positive lifting was observed. The snare was used to trap the polyp to the normal tissues 1–2 mm around the polyp. The snare was tightened slowly and gently pressed against the intestinal wall to remove the lesions mechanically. The lesion was recovered through suction channels and sent for histopathological examination.
HS-EMR group: submucosal injection of normal saline was performed with an injection needle, and positive lifting was observed. The polyp was trapped by a hot snare and gently pulled away from the intestinal wall. It was then removed by high-frequency electrocoagulation and electroresection for histopathological examination.
All procedures were performed by one of five experienced endoscopists (having performed >5000 colonoscopies each). Equipment: Colonoscopy (CF-HQ290ZI or CF-H260AI, Olympus, Japan), Injection Needle SU (NET2422–C4, Germany Endo-Flex GmbH), and Disposable polyp entrapment remover (JHY-SG-23-230-30-A1; Changzhou Jiuhong Medical Instrument Co. Ltd., China).
Observation index
Matching factors are the following: gender, age, body mass index (BMI), blood routine, coagulation function, polyp size, site, number, removal method, complications, pathological type, and hospital stay. The mean lesion size of the CS-EMR group and the HS-EMR group was (6.58 ± 0.85) mm and (6.37 ± 0.78) mm, respectively. One case of perforation occurred in the HS-EMR group. No cases of perforation were found in the CS-EMR group.
Statistical methods
SPSS26.0 statistical software was used to analyze the data. The PSM module was selected to match the trend values calculated by logistic regression according to the 1:1 recent matching method, and the caliper value was 0.02. Standardized differences were used to test the balance of the matched variables, and the balance was better when the standardized differences were less than 10%. The measurement data of normal distribution were expressed as x ± s. The comparison between groups was performed by independent sample t-test, and the post-PSM data were compared by paired sample t-tests. The number of cases represented the classified data. The unordered count data sets were compared by χ 2 test, and the post-PSM data were compared by McNemar's test or Fisher's test. P < .05 was considered statistically significant.
Results
Result before PSM
A total of 485 patients were enrolled in this study, including 162 in the CS-EMR group and 323 in the HS-EMR group (Fig. 1). Before PSM, age, white blood cell, PLT, international normalized ratio, activated partial thromboplastin time, BBPS, and polyp sizes of the two groups were statistically significant. Gender, BMI, red blood cells, PT, and thrombin time had no statistical significance (Table 2). After PSM matching, 128 patients in each group showed no statistically significant difference in general data (Table 3).
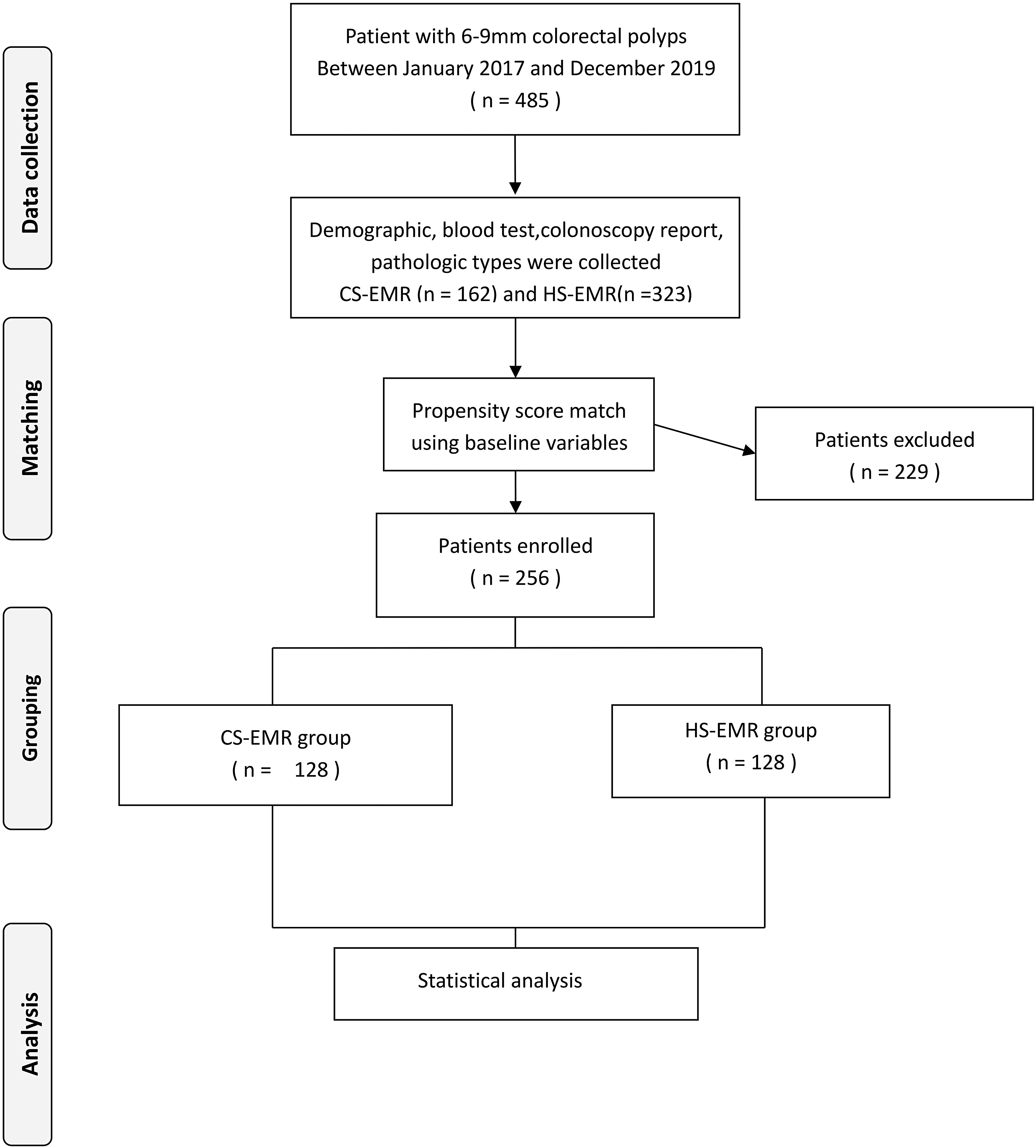
Flow diagram. CS-EMR, cold snare endoscopic mucosal resection; HS-EMR, hot snare endoscopic mucosal resection.
Demographical Characteristics and Clinical Data of the Patients
0-Ip, Pedunculated polyp; 0-Is, sessile polyp; 0-Isp, semipedunculated polyp; 0-IIa, Slightly elevated polyp; APTT, activated partial thrombin time; BBPS, Boston bowel preparation scale; BMI, body mass index; INR, international normalized ratio; PLT, platelet; PPS, post-polypectomy syndrome; PT, prothrombin time; RBC, red blood cells; TT, thrombin time; WBC, white blood cells.
Demographical Characteristics and Clinical Data of the Patients After Propensity Score-Matching
0-Ip, Pedunculated polyp; 0-Is, sessile polyp; 0-Isp, semipedunculated polyp; 0-IIa, Slightly elevated polyp; APTT, activated partial thrombin time; BBPS, Boston bowel preparation scale; BMI, body mass index; INR, international normalized ratio; PLT, platelet; PPS, post-polypectomy syndrome; PT, prothrombin time; RBC, red blood cells; TT, thrombin time; WBC, white blood cells.
Results after PSM
After matching, there were no differences in bleeding, perforation, and recovery between the CS-EMR group and HS-EMR group. Patients in the CS-EMR group had lower wound clipping rates, lower incidences of post-polypectomy syndrome (PPS), and shorter hospital stays than patients in the HS-EMR group.
Discussion
Colorectal cancer is the third leading cause of cancer-related mortality. 8 Colonoscopic polypectomies can remove precancerous lesions that might progress to colorectal cancer. Aldridge et al. 9 found that patients with 6–9 mm colorectal gland polyps had a higher risk of developing cancer than patients with <6 mm colorectal polyps, and 10%–27% of colorectal cancers occur at the site of incomplete polyp resection. The Japanese Digestive Endoscopy Association strongly recommends adopting appropriate enhanced endoscopic therapy strategies for 6–9 mm polyps to ensure complete resection rate.
However, there are many views on the resection of 6–9 mm colorectal polyps. The European Society of Gastrointestinal Endoscopy (ESGE) published clinical guidelines for colorectal polypectomies and EMRs in 2017. It suggests cold snare polypectomy (CSP) for sessile polyps 6–9 mm in size because of its superior safety profile, although evidence comparing efficacy with hot snare polypectomy (HSP) is lacking. It does not recommend the use of biopsy forceps for such polyp resections because of the high rates of incomplete resection. It also recommends HSP for pedunculated polyps. 10 Joon Sung Kim et al. showed that compared with CFP, CSP was more effective in completely eradicating adenomatous polyps ≤7 mm in size. 11 Other studies showed that CSP and HSP were similar in the complete resection rate among polyps ≤5 mm, HSP has a higher total resection rate than CSP for colorectal polyps (6–10 mm).12,13 It is more difficult to obtain and recover specimens when using CSP instead of HSP.14–16 However, abdominal symptoms, such as abdominal pain, discomfort, or abnormal defecation, increase significantly after HSP polypectomy, and the recovery time is longer. 17
A retrospective study by Takeuchi et al. confirmed that CSP had no delayed bleeding or perforation complications, and the intraoperative bleeding requiring endoscopic intervention was 3.4%, which was a safe and effective treatment for colorectal polyps <10 mm. 18 Other studies believe that CSP is a relatively common treatment for intestinal polyps and has a high intraoperative bleeding rate.19–20 Humphris et al. reported that four biopsies were performed immediately from the ulcer after removal of polyps using CSP, and the incomplete resection rate was 11%. 21 Suzuki et al. 22 conducted several years of relevant studies. These found that the complete resection rate of CSP ranged from 47.3% to 96%, suggesting that the complete resection rate needs further verification. Lee et al. proved that polyp size (≥4 mm) is an important predictor of incomplete cold resection, and histological type is not significantly correlated with incomplete resection. 23 Zhang et al. 24 showed that the incomplete resection rate (8.5%) of polypectomy defect edges and basal biopsies were higher than injected HSP (1.5%), and EMR was significantly better than CSP in the complete resection of 6–9 mm colorectal polyps. Tutticci et al. 25 found that the pale convex residues after cold trap polyp resection were common in polyps with a diameter of >6 mm, which were mainly composed of submucosal and mucosal muscular tissue and did not contain residual polyp tissues or large vascular structures. However, some experts believe that such protrusions are related to “trap stall” and may hide residual polyps or tumors.26,27 They suggest strengthening the cold trap stall technique28,29 and pay attention to the risk of mucosal defect residue and nonintegrity resection.
There are potential complications associated with endoscopic polypectomies,30,31 such as hemorrhage, perforation, postoperative syndrome, and electrocautery injury. 32 The electrocoagulation wound is a type of burning wound. Long-term electrocoagulation can lead to deep tissue damage and further expansion of postoperative wounds, which is a high-risk factor for complications such as delayed hemorrhage and perforation.17,33–37 However, CSP wounds are mechanical cutting injuries. The wounds are caused by pulling and cutting, which will not cause degeneration and necrosis of deep tissues. Wound healing is quick and postoperative complications are few. Suzuki et al. 22 showed in the comparative study on the depth and width of cold and hot snares polypectomy that the wound was further enlarged on the second day after HSP, while the wound was smaller on the second day after CSP. One study reported 53 cases (0.41%) of bleeding and 7 cases (0.05%) of perforation when 13,081 polyps were removed by hot biopsy. 38 Dobrowolski et al. 39 pointed out that the risk of bleeding after polypectomy is 0.3%–6% but could be as high as 24% in large polyps. Perforation is another serious complication with a risk of 1/2000–1/1000 and can be caused by mechanical stress, barotrauma, electrocautery, and deep resection. 40 About 5% of perforations lead to death. 41
Endoscopic polyp resection focuses on selecting appropriate polypectomy methods, controlling complications, reducing lesion residue, improving complete resection, and accurate pathological assessment. Clinically, it is vital to explore a polypectomy method that is simple, cost-effective, and has a low complication rate and high complete resection rate. Our study confirms that CS-EMR is an improvement over the standard cold trap technique. Submucosal injections help to highlight lesion edges and reduce the snare stall, making it easier to snare arbitrage polyps and reduce the mucosal defect central residue.42,43 If the lesion cannot be lifted, it means that the lesion depth may exceed the submucosal layer, suggesting a relative contraindication for endoscopic treatment. 44 There were fewer intraoperative hemorrhages of CS-EMR. This may be due to the increased amount of interstitial fluid caused by the solution injection and the tamponage effect on the submucosal vessels, as well as the separation and compression effect. 45
The study had limitations. It only used normal saline for submucosal injections. It did no comparative analysis of the effects of methylene blue, sodium hyaluronate, and norepinephrine on improving CS-EMR. There was also no comparative analysis of the trap type difference and the effect on the mucosal defect residue. Compared with CSP, CS-EMR increases the cost and operation time. Moreover, submucosal injection requires the operator to have skilled endoscopic techniques, and unskilled endoscopists may fail to lift the lesion or cause puncture bleeding or hematoma. This study was conducted at a single institution, and all procedures were performed by five experienced endoscopists, which is associated with known risks of bias. Further clinical confirmation of the large sample is needed, considering the limitations of the retrospective study method. In addition, a potential benefit of energy is assurance of peripheral destruction of all adenomatous tissue at the periphery, which would lead to lower recurrence/persistence rates at that site, however, our study did not assess this potentially differentiating outcome measure.
Conclusion
Compared with the HS-EMR, the CS-EMR wound clipping rate is low. There are fewer incidences of PPS. CS-EMR reduces the mechanical damage to the submucosal artery and tissue caused by the snare, and the low bleeding rate helps to keep the operation visual field clear. It also avoids the complications related to electroexcision and coagulation. The combination of the CSP with EMR preserved the low complication rate of CSP and the high resection rate of EMR. In conclusion, CS-EMR is a safe method for removing 6–9 mm colorectal polyps.
Ethics Approval and Consent to Participate
I confirm that I have read the Editorial Policy pages. This study was conducted with approval from the Ethics Committee of Hangzhou Third People's Hospital. This study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Consent for Publication
All participants signed a document of informed consent.
Availability of Data and Materials
We declared that materials described in the article, including all relevant raw data, will be freely available to any scientist wishing to use them for noncommercial purposes, without breaching participant confidentiality.
Footnotes
Acknowledgments
We acknowledge the hard and dedicated work of all the staff who implemented the intervention and evaluation components of the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.