
Abstract
Background:
There are several reconstruction options described in the literature after total gastrectomy for gastric cancer. The most common laparoscopic jejunal pouch technique involves evisceration of the small bowel and extracorporeal pouch formation.
Methods:
We describe a completely intracorporeal technique for the Hunt–Lawrence J-pouch Roux-en-Y reconstruction. After gastrectomy and formation of the Roux limb, we create the esophagojejunal anastomosis using an end-to-end anastomosis (EEA) stapler threaded 6–7 cm into the Roux limb to leave a tail of jejunum for the pouch. Next we form the jejunal pouch with a linear stapler and close the common enterotomy with suture or stapler.
Conclusion:
Our technique offers a streamlined and efficient approach to the Hunt–Lawrence reconstruction and can be effectively performed both laparoscopically and robotically.
Introduction
Total gastrectomy is an abdominal operation with long-term sequelae for patient quality of life. There are many different surgical reconstruction options after total gastrectomy, with the main goal to restore intestinal transit to support nutrition intake. Unfortunately, esophagojejunostomy reconstruction is plagued by severe dumping syndrome and poor food tolerance that can severely diminish quality of life. Therefore, the creation of a gastric reservoir has been proposed as a remedy for poor nutritional outcomes.1–3
Numerous randomized controlled trials have evaluated the risks and benefits of reconstruction with a jejunal pouch Roux-en-Y (J-pouch RNY) versus standard no-pouch esophagojejunostomy Roux-en-Y (EJ RNY).2–8 In theory, both reconstructions avoid complications of bile reflux by maintaining a length of Roux limb separate from the biliopancreatic limb. However, it was long believed that the more complex reconstruction of a jejunal pouch may carry a higher rate of postoperative complications, specifically anastomotic leak. 2 However, multiple randomized controlled trials have demonstrated that both J-pouch RNY and EJ RNY carry equivalent postoperative complication rates, with improved food tolerance and reduced dumping syndrome for J-pouch RNY.2–8
With the increased use of laparoscopic and robotic techniques for total gastrectomy, we describe the Hunt–Lawrence pouch creation technique that we have employed for laparoscopic esophagojejunostomy.
Methods
When preparing for a laparoscopic/robotic total gastrectomy with Hunt–Lawrence jejunal pouch reconstruction, we discuss the indications, risks, and benefits with patients, and quote an anastomotic leak rate of ∼2–5%.3,8 The most common indication for total gastrectomy is gastric cancer, including gastric adenocarcinoma, gastrointestinal stromal tumor, gastric carcinoid type III, and signet ring carcinoma. Other noncancerous indications include prophylaxis for CDH1 mutation, hemorrhagic gastritis, and intractable symptoms after partial gastrectomy. It is important to counsel patients regarding their postoperative eating habits and vitamin supplements, including a discussion that they will require multiple small meals daily and can expect poor tolerance of large food boluses, even with a J-pouch reconstruction. IRB approval for this technical description was waived.
Our trocar setup is for a laparoscopic total gastrectomy and Hunt–Lawrence reconstruction (Fig. 1). After the total gastrectomy is completed laparoscopically, the specimen is placed in a retrieval bag and extracted through an extended incision of up to 3 cm in the mid abdomen. This same extraction site, whether it be on the left or on the right side of the abdomen, can be used for insertion of the end-to-end anastomosis (EEA) stapler. We typically create the distal jejuno-jejunostomy during the gastrectomy and form a 60 cm Roux limb.
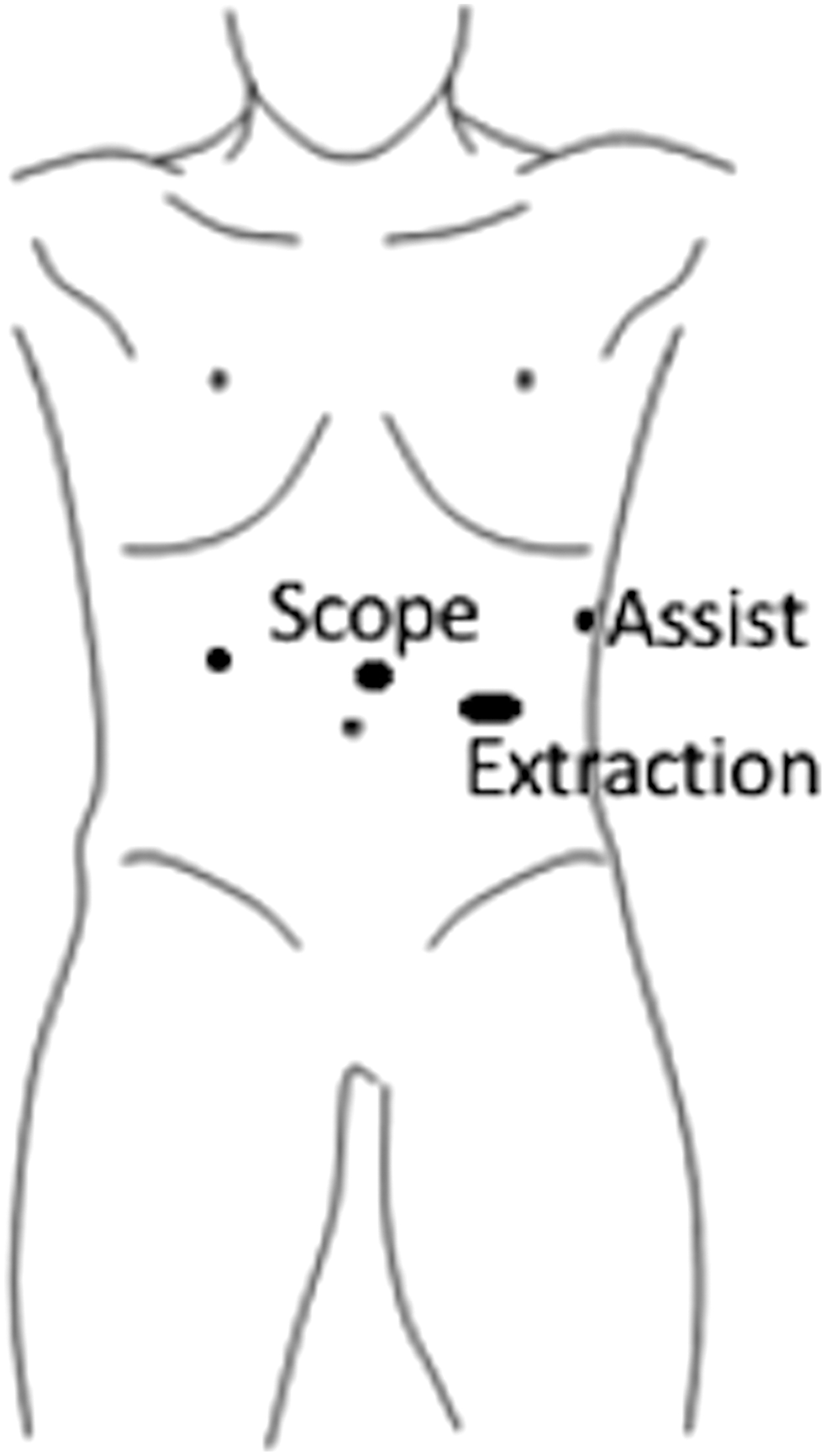
Trocar placement for gastrectomy and jejunal pouch creation. Liver retraction is usually placed in the subxiphoid region. The extended trocar site is used to retrieve the specimen using a specimen bag. A wound protector is placed into the extended trocar site to maintain pneumoperitoneum and insert the EEA stapler. EEA, end-to-end anastomosis.
With the completely intracorporeal approach, the proximal end of the Roux-limb is brought up to the esophagus in a “candy-cane” manner (Fig. 2). We first perform the esophagojejunal anastomosis by excising the jejunal staple line and introducing the 25 mm EEA stapler through the extended 3 cm extraction port. The EEA is then threaded into the opened jejunal end for ∼6–7 cm. The anastomosis is completed, leaving a 6 cm tail of jejunum beyond the esophagojejunal anastomosis. Next, the opening of the jejunal enterotomy is closed with another linear stapler. The redundant 6 cm is juxtaposed to the true Roux limb in side-by-side manner. Enterotomies are created at 6 cm below the esophagojejunostomy and the linear 60 mm stapler is introduced into each barrel of the bowel to form the jejunal pouch. The common enterotomy is then closed with an additional staple load or with suture. We then perform a leak test with endoscopic air insufflation under saline immersion, with inspection of both the esophagojejunal anastomosis and the J-pouch staple lines. We do not typically leave a nasogastric tube at the completion of surgery, but a tube can be inserted under direct observation at this point if the operating surgeon chooses.
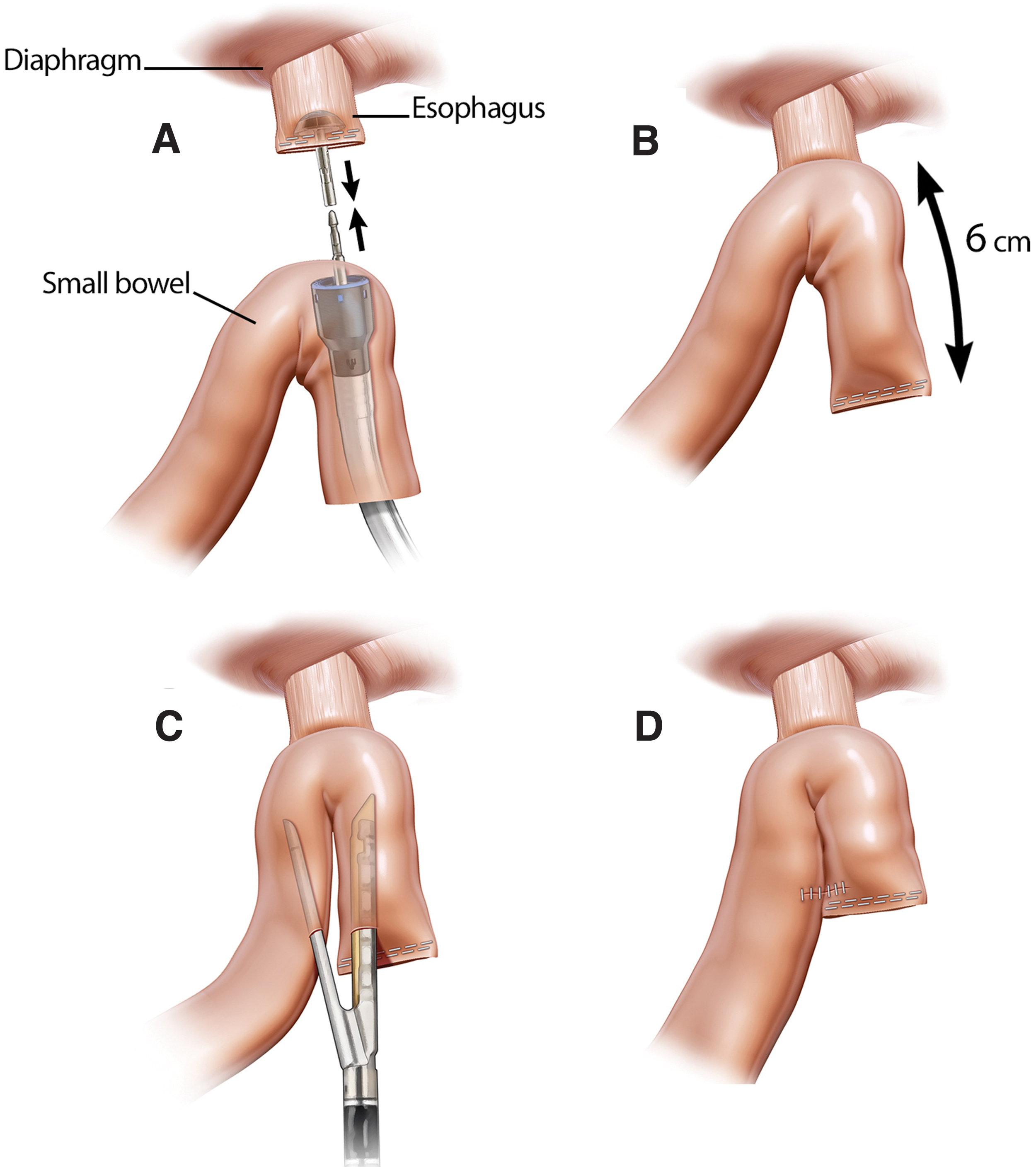
Formation of the Hunt–Lawrence pouch.
The extended fascia site of the abdominal wall is closed. The individual surgeon can choose to leave a drain around the anastomosis.
Oral feeding can commence 3–5 days after surgery. If a patient has a jejunostomy tube placed at the time of surgery, enteral feeds can be started on the first postoperative day and slowly advanced as tolerated. Contrast radiographic swallow study can be used to evaluate for anastomotic leaks if indicated. Oral diet can then be started with clear liquids and advanced to pureed liquids over the following 24–48 hours. We start with 30 mL per hour and add an additional 30 mL per hour until the patient has reached 240 mL per hour before adding thicker pureed liquids, similar to a bariatric diet. In general, our approach to diet advancement will depend on patient tolerance and preoperative nutritional status, which can vary greatly based on the presentation of the patient's gastric cancer—many of these patients have severe nutritional deficiencies preoperatively along with the added stress of chemotherapy. The patient should be advised to take in high protein and low fat meals, and to limit simple carbohydrates to avoid dumping syndrome. Ultimately, the aim is to take in six small meals a day and patients should be counseled to expect this in the long term. We have found that close involvement of a bariatric surgery dietitian for patient counseling has helped our patients tremendously.
Discussion
There is substantial evidence supporting the routine use of J-pouch Roux-en-Y reconstruction after total gastrectomy for gastric cancer. Multiple randomized controlled trials have confirmed equivalent rates of complications with J-pouch RNY versus EJ RNY.2–8 A recent meta-analysis by Syn et al. pooled data from 17 randomized trials and 8 observational studies, to include 1621 patients, and confirmed that pouch creation improves functional and nutritional outcomes in the long term, without increased perioperative morbidity. 3 Specifically, this study noted a marked reduction in dumping syndrome both at 3–6 months (8.1% versus 32.4%, relative risk 0.36, 95% confidence interval [CI]: 0.21–0.60) and 12–24 months (2.8% versus 23.6%, relative risk 0.27, 95% CI: 0.16–0.46) postoperatively for pouch versus no-pouch reconstruction. In addition, they noted a 63% relative reduction in esophagitis and heartburn and 50% relative reduction in food intake disturbance. The only disadvantage of pouch reconstruction in this comprehensive meta-analysis was increased operative time (259 versus 235 minutes). 3 In long-term follow-up of a randomized controlled trial, Iivonen et al. reported results on 12 patients 8 years postoperatively that supported J-pouch RNY reconstruction compared with EJ RNY, noting decreased dumping syndrome and early satiety, increased eating capacity, and reduced weight loss. 6 Fein et al. specifically studied patient-rated quality-of-life outcomes, and although quality of life was similar at 1 year postoperation, at 3–5 years patients with J-pouch RNY rated their quality of life better than patients with EJ RNY. 8 Thus, we prefer J-pouch RNY reconstruction after total gastrectomy whenever feasible.
Multiple techniques have been described for J-pouch construction and, in our experience, we have found the technique described to be a safe, effective, and efficient modification of the Hunt–Lawrence. Historically, many different reconstruction options have been proposed. Gastric replacement procedures that maintain continuity to the duodenum include colon interposition or jejunal interposition with or without a reservoir construction. 9 These procedures, in general, have been found to be time consuming and complicated. Many different small bowel reconstructions have been proposed to limit transit time and bile reflux, but, again, these are relatively difficult and have not been widely adopted. 9 Steinberg, in 1949, first described a J-pouch enteroenterostomy pantaloon technique with the duodenum and jejunum in continuity, bringing up a jejunal limb and performing an enteroenterostomy. This technique, however, puts patients at high risk of bile reflux and afferent loop syndrome. Hunt in 1952 proposed a modification of this with a double plicated pouch and a Roux-en-Y anastomosis. 10 Lawrence later modified the Hunt technique with a long enteroenterostomy, and this technique was then simplified by using stapling devices. 11
In the modern era, with improved technology including robotic approaches, we can offer our patients a gastric reconstruction with limited increase in operative time and complexity. We believe our technique, starting with the creation of the EJ RNY anastomosis and then completing the enteroenterostomy in situ, is more efficient than creating the J-pouch extracorporeally and may offer a reduction in operative time. The proposed technique limits handling of the bowel, which could prevent bowel trauma or unnecessary injury as well as promoting bowel recovery. With our technique, the largest incision only needs to be large enough to facilitate stomach extraction as there is no need to eviscerate jejunum for an extracorporeal anastomosis. Moreover, we have used this technique both laparoscopically and robotically.
There are some potential pitfalls and difficult technical points to highlight. Care must be taken to appropriately align the jejunal mesentery before firing the EEA for the esophagojejunal anastomosis to ensure alignment and good blood supply to the enteroenterostomy. Next, we propose one firing of a 60 cm linear stapler to create the enteroenterostomy for the J-pouch, though prior Hunt–Lawrence reconstructions have described a 15 cm J-pouch. Our bias is to avoid the difficulty of firing a second linear staple load that may be cumbersome to do, though this is a possible modification of the technique. The pouch size created with a 6 cm length of jejunum approximates the final pouch of a Roux-en-Y gastric bypass in weight-loss surgery. During the enteroenterostomy, care must be taken to avoid stress tears or undue force on the esophagojejunal anastomosis. A limitation of this technical description is the relative infrequent use of total gastrectomy for oncologic and benign conditions compared with other forms of gastric surgery. This is a combination of declining incidence in true proximal gastric cancers (non-Siewart I and II) in the United States, and the rising incidence of gastroesophageal junction cancers that are treated with esophagogastrectomy. 12 However, the minimally invasive Hunt–Lawrence pouch creation has been our approach for reconstruction whenever a total gastrectomy is performed. Even with the scarcity of cases estimated to be <20, we have only had complications associated with delayed hiatal hernias containing the esophagojejunostomy. We have not had staple-line leaks associated with this technique.
In conclusion, we describe a complete intracorporeal approach to the laparoscopic/robotic Hunt–Lawrence J-pouch Roux-en-Y reconstruction after total gastrectomy. The Hunt–Lawrence technique has previously been described with first evisceration of the jejunum and construction of the J-pouch outside the abdomen. 1 Our technique essentially converts the same open surgical approach to a streamlined intracorporeal reconstruction.
Footnotes
Authors' Contributions
All listed authors made substantial contributions to the conception of this article and are accountable for the integrity of the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.