
Abstract
Background:
Management of bile duct stones is variable. Selection of the appropriate treatment modality based on identifiable risk factors can increase the chances of a successful outcome. The aim of this study is to identify factors affecting outcomes of a laparoscopic bile duct exploration.
Methods:
Retrospective data analysis of consecutive laparoscopic bile duct explorations over a period of 13 years at a district general hospital.
Results:
The total number of patients in the study was 85. Elective explorations were 56 while 29 were emergency procedures. The mean operative time was 154 minutes. The conversion rate was 14% with failure to extract stones being the most common reason. Forty-two percent of conversions were in nonelective procedures and 17% in previous endoscopic retrograde cholangiopancreatography (ERCP) failures. Eleven percent patients had a transcystic clearance of bile duct and the largest stone removed transcystic was 5 mm. The largest stone removed by a laparoscopic choledochotomy was 15 mm and stones >20 mm were removed on conversion. Seven patients (8%) had a postoperative bile leak, 4 of these required a postoperative ERCP stent and radiological drainage while 3 required a reoperation. Three patients had retained stones treated by postoperative ERCP.
Conclusion:
Emergency procedures, increasing number and size of stones, previous failed ERCP are factors that contribute to the outcomes of a laparoscopic bile duct exploration. The chances of a successful exploration can be improved by appropriate patient and procedure selection and preparation based on identification of these factors.
Introduction
The role of laparoscopy in management of gall stone disease is firmly established. Laparoscopic cholecystectomy is the gold standard treatment for symptomatic gallstones.
Application of benefits of laparoscopy to the management of bile duct stones should have followed but the suitability/application of laparoscopic bile duct exploration is not universal.
The debate centers on the use of endoscopic retrograde cholangiopancreatography (ERCP) with endoscopic sphincterotomy (ES) and stone removal as an alternate route for the clearance of the common bile duct (CBD) and, due to its nonsurgical nature, it is more acceptable, especially, in postcholecystectomy patients. A randomized clinical trial comparing laparoscopic bile duct clearance during laparoscopic cholecystectomy versus postoperative ERCP demonstrated a similar success rate and morbidity, but a significantly shorter hospital stay in the laparoscopic group. ERCP/ES association with papillary stenosis (10%–33%), recurrent stone formation, and subsequent cholangitis especially in the younger population favors the use of the surgical approach to remove ductal calculi.1,2
The role of surgery in the removal of bile duct stones is not controversial, and it is the option resorted in case of an ERCP failure. Giving patients the benefits of the laparoscopic approach and making results similar, if not better than ERCP, requires careful preoperative planning, use of available resources, appropriate patient selection, and a skilled surgeon. The benefits of the laparoscopic approach are appreciated if conversion to an open procedure and major postoperative complications such as bile leaks and retained stones can be kept to a minimum.
Laparoscopic CBD exploration can be safely executed in elderly patients. 3 The aging population with multiple comorbidities stand to benefit from a single laparoscopic procedure. The option of using the transcystic route to clear the CBD further reduces the operative time, blood loss, procedure-related morbidities, hospital stay, and eventually the cost. It has the same efficacy and outcomes as a traditional laparoscopic cholecystectomy. 4
Avoidance of routine use of T-tubes with primary closure of the choledochotomy improves surgical outcomes. It is now the standard in laparoscopic CBD exploration and considered safe in use. 5
Updated guidelines on the management of CBD stones 2017 recommend research to define minimum standards/key performance indicators for services offering surgical CBD stones clearance and studies to establish the optimum treatment algorithm for removal of large CBDs. 6 Aim of the current study is to look at the outcomes of laparoscopic exploration of bile duct and identify predictors of a difficult procedure and postoperative complications.
Methods
The study is a retrospective data analysis of 85 consecutive patients who underwent laparoscopic bile duct exploration at a district general hospital from 2005 to 2018. The patients with suspected CBD stone followed the referral pathway as shown in Figure 1.
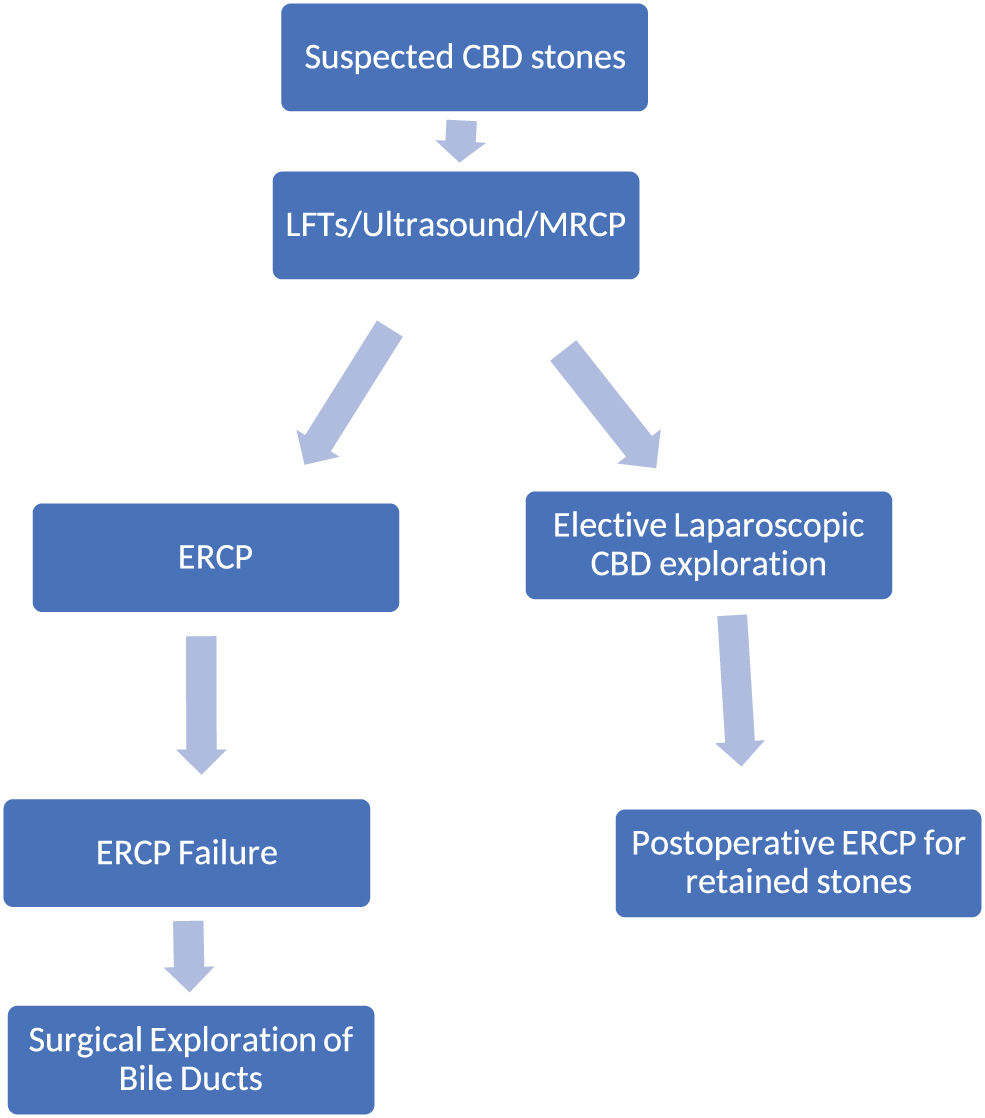
Referral pathway adopted for bile duct stone management. Color images are available online.
The data were prospectively collected by individual surgeons. The patient demographics, preoperative clinical, biochemical, radiological, endoscopic findings, operative findings, and postoperative outcomes were analyzed. The availability of at least 95% of data was set as a minimum requirement for inclusion in the study.
Inclusion criteria
Adult patients diagnosed with bile duct stones.
Preoperative radiologically confirmed ductal stones operated in elective settings.
ERCP with failure to clear duct referred for surgical clearance.
Incidental ductal stones discovered on an intraoperative ultrasound/cholangiogram in both elective and acute laparoscopic cholecystectomy.
Exclusion criteria
Open bile duct exploration.
Outcome parameters
The outcomes measured:
Operative time in minutes Elective or emergency setting of a procedure Previous attempted and failed ERCP Route of CBD clearance (transcystic or choledochotomy) Conversion rate Postoperative complications Hospital stay
The numerical data will be presented as percentages and mean.
Postoperative complications will be classified according to the Clavien–Dindo grading system. 7 Comparative data were used to determine statistical significance.
Results
Eighty-five patients were included in the study. Twenty-six percent were males while 74% were females. A mean BMI of 27 was calculated in the study group. The mean age of patients in the study was 59 years with a range of 17–86 years.
Fifty-six elective cases were included in the study, while 29 patients underwent an exploration of the bile duct in acute settings. The operative time ranged from 75 to 400 minutes. The mean operative time in female patients was 152 minutes (75–400 minutes), while the mean operating time in male patients was 149 minutes (75–330 minutes). Mean operative times in transcystic exploration, choledochotomy, and conversion to open procedure are shown in Figure 2.
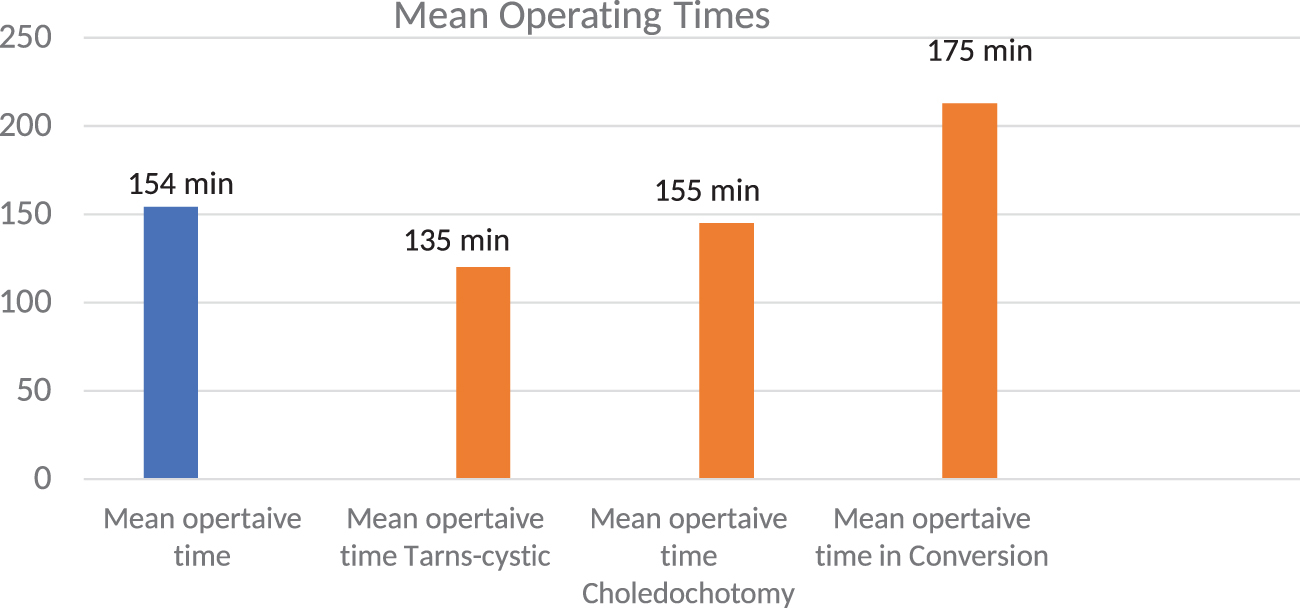
Mean operating time. Color images are available online.
Operative time in relationship to patient age showed mean of 158 minutes for patients aged (17–59) years, while 150 minutes for patients aged 60–86 years. The two-tailed p-value for age-related operative times was 0.54.
Fourteen patients (16%) underwent a laparoscopic bile duct exploration after a failed attempt at ERCP to remove stones preoperatively. Twelve laparoscopic CBD explorations were converted to open 14%. Five of these patients were operated acutely; 42% of conversions, while 2 were post-ERCP failure (17%). Four of the conversions (33%) were in male patients.
The transcystic approach was successful in 11% of cases, and the largest stone removed via the cystic duct was 5 mm. The average size of stones that required conversion was 15 mm, while stones as large as 20 mm were removed on conversion. Sixteen patients were identified with postoperative complications as shown in Table 1.
Postoperative Complications
CBD, common bile duct; CT, computed tomography; ERCP, endoscopic retrograde cholangiopancreatography.
The median hospital stay was 6 days with single-day stay for transcystic procedures. The mean hospital stay after conversion was 12 days.
Discussion
About 10%–15% of patients with gallstones concomitantly have ductal stones. The number of patients with ductal calculi and their related complications such as cholangitis and pancreatitis are high. The associated morbidity and mortality are significant and need addressing in a satisfactory, safe, and cost-effective manner.
Management of ductal calculi is multimodal and the published literature lacks strong evidence to end the debate regarding the ideal approach to clear bile duct of stones. 8 Laparoscopic exploration of bile duct is as an advanced laparoscopic procedure which demands attention to details combined with the right equipment. It offers the benefits of minimal access surgery and the advantage of a single therapeutic procedure.
This study collected and analyzed data from a district general hospital and describes the surgical management of bile duct stones looking at factors that influence outcomes. The limited number of patients (n = 85) identified for inclusion over a time period of 13 years points to the possible underutilization of the surgical modality. The settings are of a district hospital without a specialist hepatobiliary resection unit but an equipped and functioning endoscopy department and the availability of benign upper gastrointestinal surgeons.
The male to female ratio of (3:1) was seen in patients recruited and their mean BMI was 27.
The difficult access to an operating suite with a trained surgeon in attendance was the prime factor in not opting for a primary surgical clearance of bile ducts even in otherwise good surgical candidates. Endoscopic (ERCP) clearance of ducts was set as the default procedure even though the patient admitting and managing team was surgical.
The preferable route for the laparoscopic removal of CBD stones is transcystic as the outcomes of a successful transcystic clearance matches those of a laparoscopic cholecystectomy and the advantages include a shorter operating time, less blood loss, and a shorter hospital stay. 4 The reduced operating time for the transcystic approach by a mean of 20 minutes was recorded in our study; further, the hospital stay for transcystic exploration was expectantly less compared to choledochotomy patients.
The patient selection for a transcystic exploration was based on preoperative and intraoperative imaging. A duct size of 7–9 mm with ductal stones 3–5 mm distal to CBD-cystic duct junction without any impaction was considered for a transcystic retrieval.
It was possible to clear the bile ducts of only 11% of the study population through the transcystic route. The explanation is multifactorial. Initially the inherent shortcomings of the transcystic route require that the stones extracted via the cystic duct to be comparable in size to its diameter, that is, 3–5 mm. Further, the greater the number of stones and the more tightly they are packed in the CBD, the chances of successful outcome diminish. On top of this, the position of the stones in relationship to the cystic duct-CBD junction and anatomy of the cystic duct itself, especially the take off angle at the confluence with the common duct, affect its instrumentation and withdrawal of stones via this route.
Transcystic exploration was also done in incidental CBD stones diagnosed on laparoscopic intraoperative ultrasound during a laparoscopic cholecystectomy in both elective and acute settings. The lower frequency of transcystic success in our patients (11%) was also secondary to the fact that laparoscopic removal of CBD stones was not considered as an option in patients with stones (<5 mm) on preoperative imaging and most of them were subjected to an ERCP followed by a laparoscopic cholecystectomy. The largest stone retrieved via the transcystic route in our study was 5 mm.
The technicalities of the laparoscopic procedure include the ability to perform an intraoperative cholangiogram and or a laparoscopic ultrasound to look for ductal stones. A choledoscope for visualization and clearance of the bile ducts is an essential tool. Access and availability of stone retrieval equipments such as baskets, nets, and balloon catheters are part of the laparoscopic stack that should be present at the time of surgery. The familiarity and usage of the various gadgets available increase the chance of having a successful outcome and at the same time require special training not only of the surgeon but also of the whole scrub team.
The success rates reflect in the results from centers, which routinely use these resources. It is worth mentioning that laparoscopic bile duct clearance is not a procedure which cannot be managed at district level hospitals provided the expertise and equipment are available and undoubtedly if conducted locally will reduce the burden on referral centers. 9
Patient selection is critical in planning the appropriate approach to remove CBD stones as already mentioned. It depends on preoperative and intraoperative imaging identifying the size of the CBD, the number and size of stones with the possibility of impaction. A laparoscopic choledochotomy was done in 86% of patients based on these findings. The presence of multiple ductal stones, CBD diameter >9 mm, history of cholangitis and or pancreatitis, unsuccessful ERCP, and failed transcystic approach in an appropriate size duct lead to removal of stones via a vertical choledochotomy. The incision finally closed with a running intracorporeal suture and the subhepatic area drained as required. The largest stone removed using this approach was 15 mm in size.
The mean operating time was 135 minutes for a transcystic approach, while the average time to complete a laparoscopic choledochotomy was 155 minutes.
This study has a conversion rate of 14%, which is higher than the rates reported in literature. Wang and colleagues report conversion rates of 4.2%, while Pan et al. in a recent meta-analysis report it up to 7%.10,11 The majority of procedures in the study were converted due to the inability to disimpact ductal stones and not getting clear views on choledoscopy. This is vital to ensure safe instrumentation and clearance of the duct. Bleeding and a large number of stones in a limited sized duct can limit choledoscopic views. Unguided instrumentation predisposes to future stricture formation due to trauma. Failure to disimpact distal stones and suspected residual stones contributed to the high conversion rates.
This difference in conversion rates is also explained when we look at the characteristics of the patient cohort subjected to surgery. Twenty-nine of the 85 procedures were carried out in the acute settings, which was 34% of the total cases. Five of the 12 conversions (42%) occurred in procedures carried out acutely.
The commonest reason for conversion was related to larger size and the increased number of stones. Both of these increased the risk of stone impaction and hence conversion. The largest stone extracted via the laparoscopic choledochotomy in this series was 15 mm, while on conversion larger stones up to 20 mm were delivered.
The results of using surgery as an option after an unsuccessful endoscopic approach are obvious when we look at the data. Fifteen percent of patients referred for surgical clearance were ERCP failures adding to the complexity of the surgical candidates and limiting options for the surgical team, leading to high conversion rates. Seventeen percent of conversions were in patients in a previously failed ERCP. The majority of ERCP failures of 58% were due to large stone size and stone impaction.
Fragmentation using lithotripsy of ductal stones size >20 mm before endoscopic retrieval is recommended, if this fails to retrieve stones endoscopically, the fragmented stones stand a better chance to be removed laparoscopically. 12 Lithotripsy unfortunately failed to fragment stones in the majority of patients during ERCP before they were referred for surgical removal adding to complexity of surgery.
The mean operating time for the converted procedures was 175 minutes, while the mean length of stay in the hospital for patients who underwent a conversion was 12 days.
This patient series also reveals a move away from the regular use of T-tubes in CBD exploration unless otherwise indicated, for example, with a difficult disimpaction of a distal CBD stone, edematous duct, or any reason suspected to obstruct smooth onward flow of bile. 13
The postoperative complications were stratified using the Clavien–Dindo classification.
The Clavien–Dindo Grade I cases included:
Three superficial wound infections, which responded to local treatment.
A delay in hospital discharge due to postoperative pain, which required investigating using a computed tomography (CT) scan, which was normal.
Seven patients had a postoperative bile leak (8%). Four were managed using a postoperative ERCP with stenting and percutaneous radiological drainage was used to remove residual intra-abdominal collections Grade III(a). Three patients had to be returned to the theater Grade III(b).
Seven patients (8%) had significant bile leak after the procedure and a laparoscopic washout was done for 3 of them. Two patients developed an intra-abdominal collection, which was radiologically drained and another 2 required a postoperative ERCP with stenting to control bile leak.
A look into the available literature relates the rates of postoperative bile leaks in the range of 7%–11%. 14 The possible risk factors for postoperative bile leak include the following:
Patient age
Sex
ASA grade
Intra-abdominal infection
Severity of jaundice
Size and number of stones
Size of the CBD
Operative blood loss
Operative time
Choledochotomy size
Type of suture
Type of repair and finally
The experience of the surgeon
It must be emphasized that not all bile leaks require intervention and an expectant leak is quite satisfactorily dealt with a subhepatic drain placed at the time of surgery and the leak gradually settles. Although the reexploration and washout increased the length of hospital stay, none of our patients had a fatal complication in relationship to a bile leak and biliary peritonitis.
Retained stones were seen in 3 patients (4%) in this review. Confirmation of duct clearance was done by choledoscopy and at times supplemented with an intraoperative cholangiogram or a laparoscopic intraoperative ultrasound. Residual stones were still discovered postoperatively. MRCP was used for confirmation of retained ductal calculi in suspected patients. The literature reports varying frequency of retained stones ranging from 2% to 8%. 15 These results were comparable with a 4% frequency of retained stones found in this patient population who had their CBDs cleared via the laparoscopic approach. The retained stones were successfully removed using postoperative ERCP.
Looking at the risk factors mentioned in the CHOLE S cohort 16 for association of preoperative factors and postoperative outcomes in laparoscopic cholecystectomy namely:
Patient age
Sex
ASA grade
BMI
Emergency versus elective settings
CBD dilation
CBD stones
Previous ERCP
It is easy to draw comparisons that these factors can possibly influence the outcomes of a laparoscopic CBD exploration as well. However, our data based on demographics of the patients' age and sex failed to reveal gross discrepancies in the operative time when the study population was compared. The mean operative time in female patients was 152 minutes (75–400 minutes), while the mean operating time in male patients was 149 minutes (75–330 minutes). Similarly, comparing the operative time for patient population was divided into two age groups; up to 59 years and the other 60 years and older, and it revealed an operative time difference of 8 minutes (P > .05).
Emergency settings affect operative outcomes. It is reported to increase operative time, conversion rate, postoperative complications, and 30-day reintervention rates. Twenty-nine patients of this study group were managed in the acute settings and contributed to almost half of the group of patients who needed a conversion (42%). The reasons for conversion were variable from failure to disimpact stones, peroperative bleeding, difficult anatomy, or poor access to CBD.
Preoperative ERCP has been suggested as an independent factor for a difficult laparoscopic cholecystectomy and also contributes to an increase in operative time, conversion rate, and postoperative complications. Seventeen percent of procedure conversions to open were in patients with a failed preoperative ERCP. The procedure failed due to duodenal diverticula leading to failure to cannulate CBD and due to large, impacted CBD stones, which could not be extracted or fragmented endoscopically.
Risk stratification in a small study group may be insufficient, but the need to identify factors that affect operative outcomes cannot be over stressed. Patient selection based on these factors and opting for the appropriate procedure will improve the chances of a successful outcome.
Conclusion
Laparoscopic bile duct clearance is a safe procedure in safe hands. The chances of a successful outcome can be improved by appropriate patient selection and preparation. Developing scoring systems using demographic, clinical, and radiological data can stratify risks and help physicians make a better management decision.
Footnotes
Disclosure Statement
No disclosures to report.
Funding Information
No funding received for the study.