
Abstract
Crohn's disease (CD) is a pan-intestinal disease of the gastrointestinal tract characterized by inflammatory, penetrating, and fibrostenotic phenotypes. Fibrostenotic stricture formation, without inflammatory or penetrating disease, is a common complication in CD, primarily affecting the small intestine and leading to small bowel obstruction. Because there is no medical therapy that prevents or reverses stricturing disease, endoscopic and surgical treatments are the mainstays of treatment, indicated to palliate symptoms and treat the complications. Endoscopic approaches include dilation, stricturotomy, and endoscopic stenting. Surgical options include resection, intestinal bypass, and various strictureplasty techniques. In this article, we will focus on the treatment of stricturing CD: specifically, the considerations important in choosing between different treatment options and technical tips to deal with complicated disease.
Stricturing Crohn's Disease
Crohn's disease (CD) is a chronic unremitting and, to date, an incurable inflammatory disorder of the alimentary tract, affecting any part of the gastrointestinal tract from mouth to anus, and presenting with one of three phenotypes: (1) nonpenetrating/nonstricturing disease characterized by inflammatory masses; (2) penetrating disease characterized by fistulae and abscesses; or (3) fibrostenotic disease, characterized by fibrotic strictures. Strictures are defined by the Montreal Classification as “a constant luminal narrowing (endoscopic, radiologic, or surgical) with prestenotic dilation or obstructive signs without penetrating disease.” 1 Strictures can develop early in the inflammatory process or independently of inflammation. Fibrostenotic Crohn's strictures occur in the duodenum (0.5%–4% of patients 2 ) and more commonly in the small bowel. In the terminal ileum and colon, strictures are usually the result of penetrating and nonpenetrating/nonstricturing disease. Colonic “inflammatory” strictures show an underlying malignancy rate of 0.8%–6.8%. 3
Clinical Presentation
Patients with strictures may develop progressive narrowing over time and only become symptomatic when a critical degree of narrowing has been reached. Patients with gastroduodenal strictures typically present with early satiety, postprandial fullness, burping, and vomiting. Patients with strictures of the small intestine initially notice postprandial bloating, crampy abdominal pain, obstipation, and constipation. They consciously or unconsciously learn to compensate with dietary modifications, but occasionally progress to nausea, vomiting, and high-grade intestinal obstructions. Patients with colonic strictures present with bloating, distension, obstipation, constipation, and abdominal pain.
Workup
Evaluation of the inflammatory versus fibrostenotic disease in a patient with CD can be done by measuring inflammatory markers, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and fecal calprotectin. Common noninvasive imaging modalities include computed tomography or magnetic resonance enterography (CTE or MRE). They help in delineating inflammation, fistulas, abscesses, or scarring without surrounding inflammation. CTE and MRE are also particularly useful in preoperative planning showing luminal narrowing, wall thickening and prestenotic dilation to map the number, degree, length, and location of strictures, and also estimate overall small-bowel length. Patients with stricturing disease may develop a single stricture or a series of strictures with intervening healthy intestine, but the most critical stricture is the one that drives the symptoms and is characterized by upstream dilation on imaging. Invasive diagnostic modalities, including endoscopic evaluation with or without biopsy, are important to evaluate for malignancy, but may be hindered by limited endoscopic accessibility in the presence of tight strictures or luminal narrowing secondary to angulations caused by adhesions from previous surgical procedures or localized sepsis.
Management
Initial management of patients with CD who present with an acute bowel obstruction includes bowel rest, intravenous (IV) hydration, and nasogastric decompression in the presence of vomiting. If imaging demonstrates an abscess, antibiotics treatment is instituted for small abscesses (<3 cm) or abscesses located in a difficult location to access; otherwise, percutaneous drainage is indicated and facilitate the resolution of the obstruction. If the obstruction is completely due to a fibrostenotic or inflammatory stenosis without an abscess, most resolve with bowel rest within 24–72 hours with or without the addition of IV steroid therapy. If symptoms do not resolve, a fixed obstruction, that is, a malignant obstruction, rather than an inflammatory obstruction, must be considered and surgery should be pursued.
Following resolution of the acute obstruction, up to 75% of patients eventually require endoscopic or surgical treatment of the underlying stricturing disease or recurring obstructive symptoms occur as there is no current medication that can reverse fibrosis in the intestinal wall. Endoscopic techniques include dilation, stricturotomy, and stent placement; surgical interventions include strictureplasty techniques, intestinal resections, and bypass. Whether endoscopic or surgical, intervention can often be delayed until inflammatory, infectious, and nutritional concerns have been addressed.
Nonsurgical endoscopic techniques
Endoscopic approaches include dilation, stricturotomy, and endoscopic stenting. Endoscopic approaches are limited to areas that are endoscopically accessible—gastroduodenal, colonic, terminal and neo-terminal ileal, and anastomotic strictures. 4 Most small bowel strictures are not endoscopically accessible. Endoscopic outcomes are measured by immediate technical success (the ability to pass the endoscope through the strictured bowel) and long-term success (endoscopy and surgery-free survival).
Endoscopic balloon dilation can be performed on single short (<5 cm) fibrotic strictures with little inflammation and without prestenotic dilation.5–8 Complications of endoscopic balloon dilation include hemorrhage (2%–3%) and perforation (1%–5%). 9 Technical success is achieved in 90% of cases, but fewer (70%–80%) report short-term improvement in symptoms, 73.5% require repeated dilations, and 43% require surgery within 2 years. 10 In few patients, balloon dilation may spare patients from surgical resection or re-resection; in the majority, the benefit of balloon dilation may only be to postpone the time to surgery.11,12
In contrast to the blunt force applied with balloon dilation, endoscopic electroincision allows for precise stricturotomy using an endoscopic needle knife. Early series have demonstrated a lower rate of subsequent surgery as compared with endoscopic balloon dilation. For anastomotic strictures endoscopic stricturotomy showed 100% immediate technical success, higher symptomatic and endoscopic improvement rates as compared with balloon dilation, and <10% of patients requiring surgery within 1 year. Precise electroincision has a lower risk of perforation (1%), but a higher risk of bleeding (6%–10%) than endoscopic balloon dilatation.9,13 Bleeding typically occurs within 4 days of the procedure, a time usually associated with the falling off of any eschar on the stricturotomy. Stricturotomy is a promising new development in the endoscopic treatment of strictures, performed in few specialized centers, reporting lower rates of progression to surgery on short-term follow-up, but longer term data are still needed.13,14
There are limited case reports and case series describing the use of endoscopic stenting in ileocolonic and colonic CD strictures, with the majority of stents used to address anastomotic strictures.15–17 Durable success has been limited by the occurrence of stent migration, impaction, perforation, and fistulization. To address these risks, the use of different stent types, including lumen apposing metal stents, fully covered stents, and biodegradable stents, and the appropriate stricture length and duration of stenting are being better understood.
Surgical techniques
Bowel sacrificing techniques
Resection remains the more common approach for patients undergoing operative treatment for obstruction due to Crohn's stricture. Terminal ileitis, the most common feature and location for intestinal CD, is best addressed with ileocolic resection. Resection can be performed with primary anastomosis and immediate reconstruction of intestinal continuity. Stoma creation should be considered in malnourished patients, in patients on chronic high-dose steroids, or in a situation where the anastomosis would be located in an anatomical location with residual inflammation or infection. If there is a concern for malignancy, resection should be performed following oncologic principles.
Postresection recurrence continues to be a concern. After surgery, endoscopic recurrence rates are estimated between 35%–93% at 1 year and 85%–100% at 3 years, symptomatic recurrence rates are estimated between 10%–38% at 1 year, 28%–47% at 5 years, and 36%–61% at 10 years, 18 and, most importantly, there is a 15%–40% reoperation rate after 10 years from the index procedure. 19 Antitumor necrosis factor agents have been used to prevent postoperative endoscopic recurrence rates in patients with CD; 20 however, they have not demonstrated a benefit in lowering the clinical and surgical recurrence rates. 21
Surgical resection techniques have been investigated in an attempt to reduce recurrence. The anastomosis seems to be an area at particular risk as recurrences most commonly occur perianastomotically. 22 Extending the margins of resection proximally and/or distally or attempting to achieve microscopically negative margins have not been shown to reduce the risk of recurrent disease, and dangerously increase the risk of short gut with more extensive resections. 23 The role of anastomotic configuration has also been evaluated as a means to decrease the risk of recurrence. When compared with handsewn end-to-end anastomoses, stapled side-to-side anastomoses have been promoted with the theoretical advantage of the wider anastomotic diameter. 24 Although some studies have shown lower rates of recurrence25,26 and reoperation,25–28 other studies have shown that no anastomotic configuration seems to offer better protection against recurrence.29,30
More recently, Kono et al. have proposed an antimesenteric handsewn functional end-to-end, the Kono-S, anastomosis (Fig. 1). 31 In brief, the mesentery is divided along the bowel wall to avoid devascularization and denervation of the bowel (Fig. 1A). The diseased segment of bowel is then divided with a linear stapler such that the mesentery is located at the midpoint of the staple line at a 90° angle (Fig. 1B). Each staple line is oversewn and then sewn to each other to create the supporting column (hence the “S” in Kono-S) as the backbone of the anastomosis (Fig. 1C). On each side, a longitudinal enterotomy is made 0.7 cm from the supporting column on the antimesenteric side of the intestine (Fig. 1D) and then the anastomosis is constructed by sewing together these two enterotomies in a side-to-side manner, producing a very wide anastomotic lumen (Fig. 1E, F).
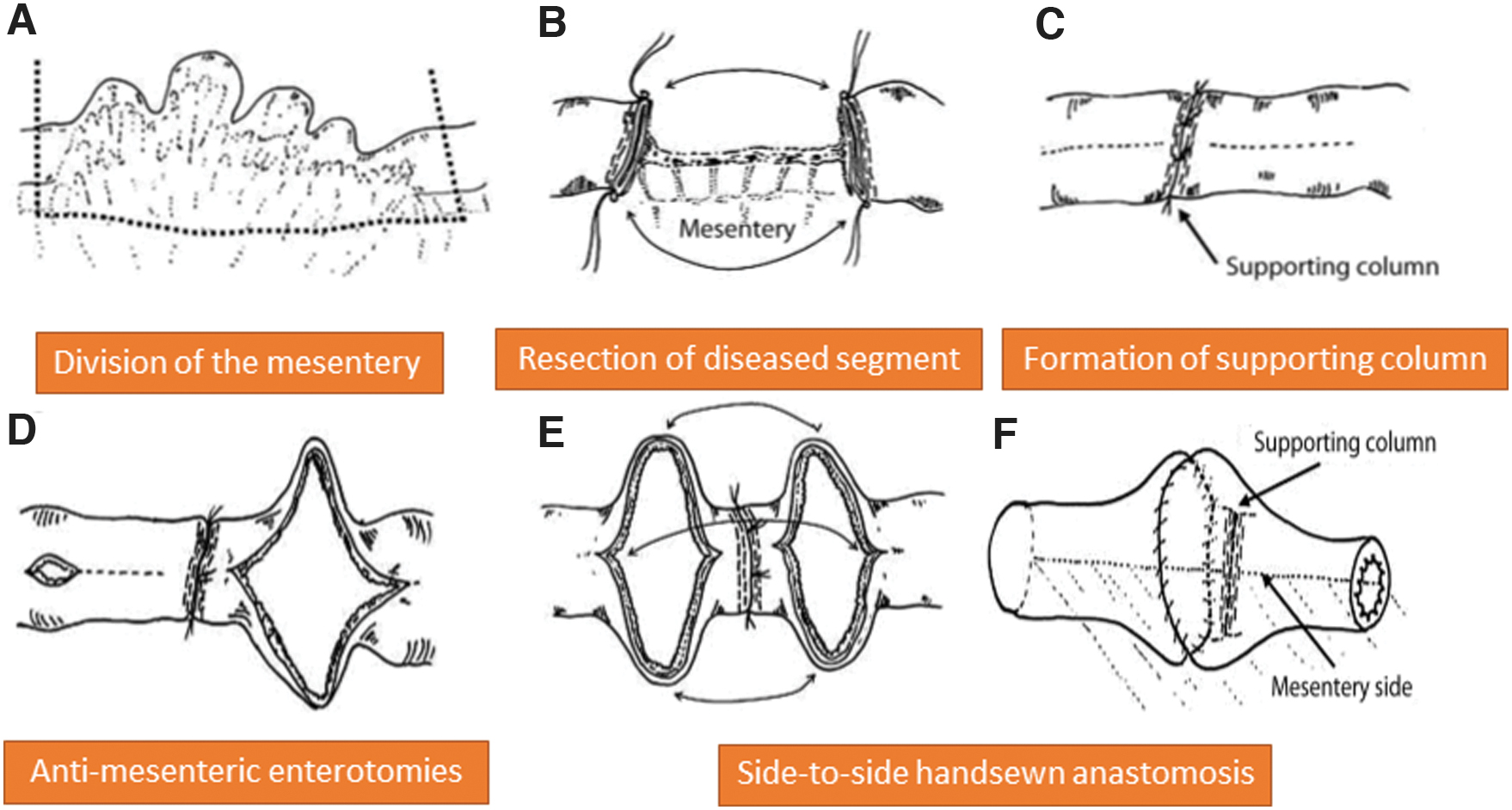
Kono-S Anastomosis. The antimesenteric handsewn functional end-to-end, Kono-S, anastomosis is created by dividing the mesentery along the bowel wall
Nonrandomized observational studies have reported a significantly lower rate of surgical recurrence.31,32 In addition to the wide anastomosis, possible explanations for the decreased rate of surgical recurrence include (1) the construction of the supporting column that maintains the diameter and the orientation of the anastomosis and prevents distortion of the anastomotic lumen; (2) the antimesenteric location of the anastomosis, away from the mesenteric side that is commonly observed to be the location of the recurrent disease. Another advantage of this anastomosis is the ease of endoscopic instrumentation: the functional end-to-end configuration of the Kono-S anastomosis makes it particularly amenable to endoscopic surveillance and treatment (i.e., balloon dilation and stricturotomy).
Patients with CD are at risk of short gut either after a massive intestinal resection or multiple resections. The length of the recurrence is frequently very similar to the length of the index disease. 33 Hence, patients who present with extensive disease are the ones at highest risk of short gut after multiple sequential resections. Extensive disease should be handled with bowel preserving procedures (see Non-Bowel Sacrificing Techniques). Fortunately, the small bowel has a remarkable capacity to adapt structurally and functionally. Yet, bowel resections of multiple segments or long segments of small intestine, particularly the terminal ileum, can lead to significant nutritional deficiencies, even before a full-blown short gut syndrome. Decreased absorption, specifically of bile salts, fats, and vitamins A, D, E, K, and B12, can lead to diarrhea and decreased nutritional status. With more severe forms, patients may require resuscitation with IV fluid or eventually sustenance with parenteral nutrition. Patients with short gut syndrome have a decreased life expectancy.
Nonbowel sacrificing techniques
Intestinal bypass
Bypass is only indicated in the treatment of gastroduodenal strictures that are not amenable to strictureplasty or endoscopic dilation because resection with pancreaticoduodenectomy carries an unacceptably high risk of morbidity and mortality for nonmalignant pathology. Bypass with gastrojejunostomy is complicated by bile reflux gastritis, dumping syndrome, marginal ulceration, or blind loop syndrome. 34
Strictureplasty techniques
Owing to the risks of short bowel syndrome, nonresective options have been pursued as an alternative to increase the lumen of the bowel while maintaining the absorptive function of the intestine especially in patients who would otherwise require a massive intestinal resection or multiple sequential lengthy intestinal resections.
Strictureplasty techniques in the small bowel are indicated for fibrotic strictures without inflammation, particularly if multiple strictures are present with intervening segments of normal intestine or when recurrent strictures develop in a patient with previous bowel resections at risk for short bowel syndrome.35–39 Contraindications to strictureplasty include malnutrition, a stricture within an inflammatory mass, a stricture involved in the inflammatory reaction caused by a perforation, abscess or fistula, or the presence of dysplasia or malignancy at the site of the intended strictureplasty. For technical reasons, a strictureplasty cannot be performed in long strictures with thick unyielding intestinal wall and should be discouraged if the stricture is the presumed site of occult bleeding causing chronic anemia. In addition, if a stricture is next to a planned segment of resection, the stricture should be included in the resection in favor of the overall economy of the surgical procedure unless the patient is at risk for short gut (Tables 1 and 2).
Indications for Strictureplasty
Contraindications for Strictureplasty
Although resection of asymptomatic strictures is not performed due to the risk of short bowel syndrome, asymptomatic strictures that are amenable to strictureplasty may be addressed to prevent future symptom recurrence. Before performing a strictureplasty, careful examination of the stricture with biopsies of suspicious areas must be performed to rule out malignancy. 40
Although there are many variants of strictureplasty techniques, they can be classified in three main groups. In the next few paragraphs, the technical details are briefly described.
Heineke-Mikulicz strictureplasty
A longitudinal enterotomy is made over the stricture on the antimesenteric side of the bowel, extending 1–2 cm beyond the length of the stricture proximally and distally (Fig. 2A). The enterotomy is then closed transversely with interrupted seromuscular absorbable sutures. The closure may be performed in one or two layers. The Heineke-Mikulicz strictureplasty is appropriate for strictures up to 3–5 cm.

Finney strictureplasty
The strictured segment is folded on itself, creating a U-shape loop (Fig. 2B). The two loops of the “U” are sutured together with interrupted Lambert sutures placed close to the facing mesenteric border (posterior outer layer), extending 1–2 cm beyond the length of the stricture proximally and distally. A longitudinal enterotomy is created just above the stitches. The anastomosis is constructed with an inner layer of running absorbable suture, reinforced by an anterior outer layer of interrupted Lambert sutures. The Finney strictureplasty is appropriate for strictures 5–12 cm in length. Long rigid strictures that lack the pliability to fold onto itself may require folding normal bowel on diseased bowel.
Michelassi strictureplasty or side-to-side isoperistaltic strictureplasty (SSIS)
The bowel and the mesentery are divided at the midpoint of the segment of bowel intended for the strictureplasty (Fig. 3). The proximal and distal loops of the diseased bowel are brought alongside each other in a side-to-side isoperistaltic manner, lining up the stenotic areas of one loop against the dilated areas of the other loop. The two limbs are approximated with interrupted Lambert sutures before making the longitudinal incision along the length of each of the two intestinal loops. The ends of the bowel are spatulated to avoid creating blind ends. Luminal hemostasis is obtained with suture ligation and electrocautery. The inner layer of running full thickness absorbable sutures starts at the middle of the posterior sutureline and progresses anteriorly as a running Connell stitch. An anterior outer layer of interrupted seromuscular sutures completes the two-layered closure. Thick and friable mesentery may restrict the ability to transect and slide the proximal intestinal loop alongside the distal intestinal loop and precludes adapting a side-to-side isoperistaltic strictureplasty (SSIS).
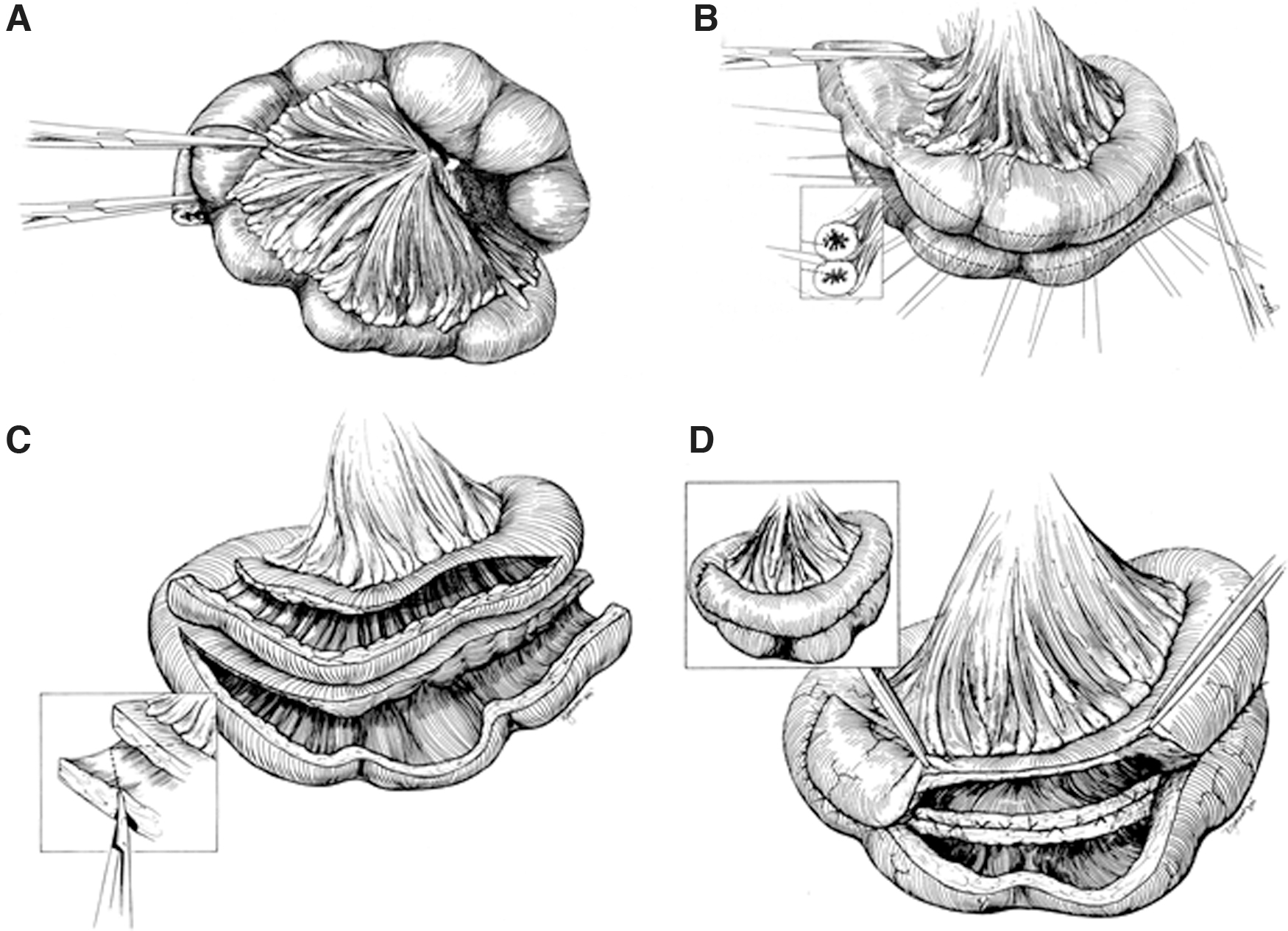
SSIS. The bowel is divided at the midpoint of the diseased segment
There are several variants of the SSIS to address complex situations. If the transection of the intestine and the mesentery cannot be performed at the midpoint of the diseased loop and one loop is shorter than the other, normal bowel can be recruited into the anastomosis when aligning the two limbs. If the middle of the diseased loop is affected by a long rigid stricture, that section can be resected before sliding the proximal and distal loops alongside each other (Fig. 4A). If the severe segment of disease is at one end of the diseased loop, that segment can be resected and a side-to-side-to-end strictureplasty can be performed (Fig. 4B). 41 If a patient presents with three severely fibrotic and deformed bowel loops separated by two diseased segments with sequential strictures, an end-to-side-to-side-to-end strictureplasty (Michelassi II) is performed (Fig. 4C). 39 In this case, after resection of the three severely diseased segments, the remaining two discontinuous segments are used to perform an SSIS, according to the original description. The two ends of the SSIS are then anastomosed with the proximal and the distal bowel.
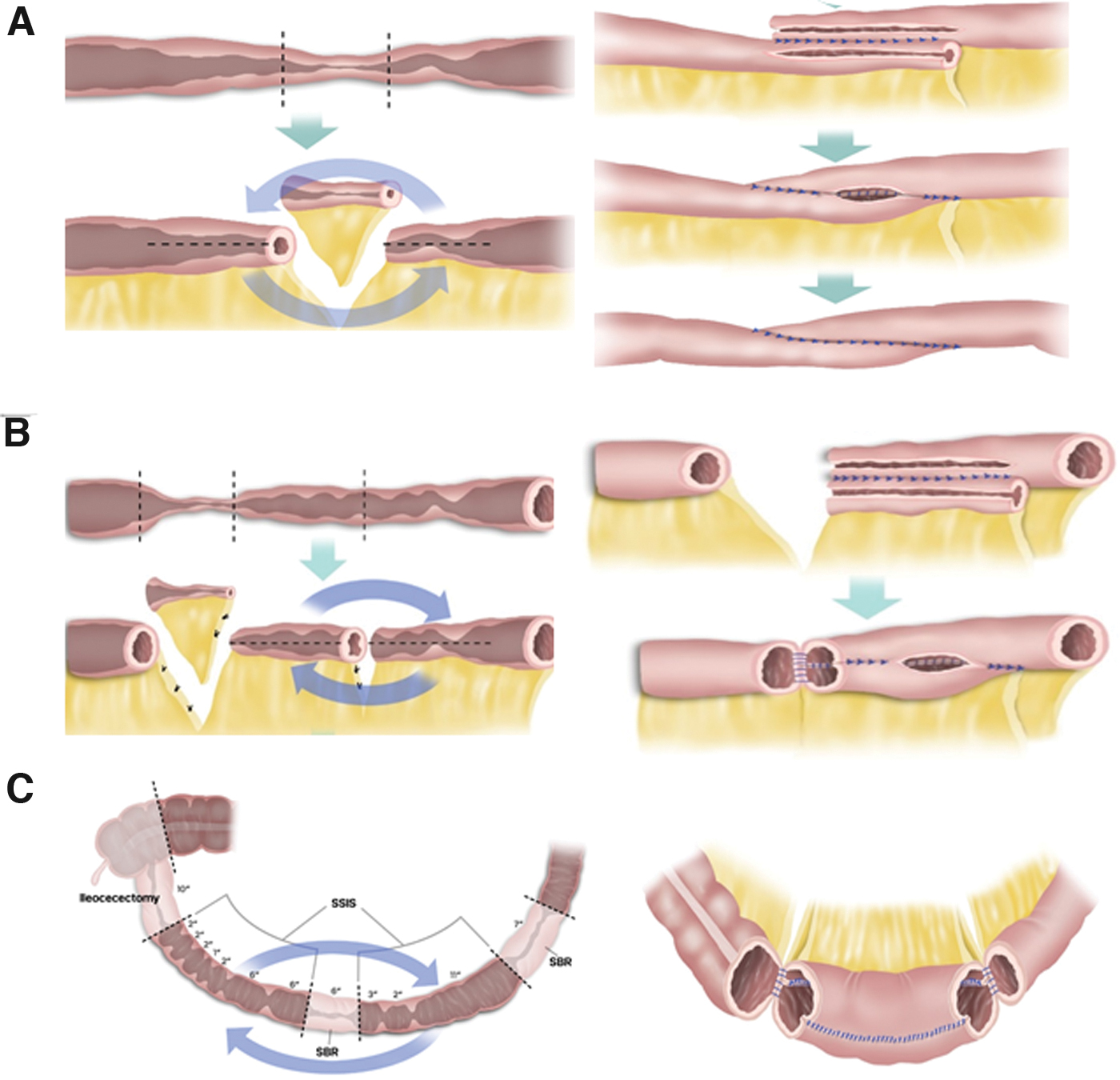
Techniques for combining resection with SSIS.
In an article reviewing the 25 years of experience with SSIS, Michelassi et al. found that 24% of patients who underwent strictureplasty for jejunoileitis underwent one or more SSIS, and of those patients who underwent SSIS, 47% required additional small bowel resection away from the site of strictureplasty and 45% required at least one synchronous conventional strictureplasty. 42 Most importantly, the median length of spared bowel was 52.5 cm (range: 20–280), equal to 17% of bowel length (range, 4.3%–40%).38,42
In a meta-analysis including 19 series on strictureplasty, Yamamoto concluded that the most commonly performed strictureplasty was the Heineke-Mikulicz strictureplasty (81%) and strictureplasties are most often performed in the jejunoileal region (94%). 43 The mean number of strictureplasties performed during an operation was three, and the majority of patients underwent simultaneous resection and strictureplasty (61%). 43 The risk of postoperative hemorrhage was 9.3%, probably due to creating a sutureline in thick diseased bowel; septic complications occurred in 4% of cases and malignant transformation at the site of the strictureplasty was identified in only 3 cases (0.34%). In a meta-analysis including 32 studies with a total of 1616 patients and 4538 strictureplasties, Campbell found that the incidence of early or late complications after a conventional (Heineke-Mikulicz, Finney) or nonconventional (SSIS) strictureplasty was similar (early complications 15% versus 8% and late complications 29% versus 17%, respectively). 44
Comparing recurrence rates after strictureplasty and resection is challenging due to the fact that these operations are usually performed in two different groups of patients who may have different risks of recurrence: strictureplasties are performed in fibrostenotic Crohn's, whereas resections are performed in all types of Crohn's (fibrostenotic, inflammatory, and penetrating). How much the phenotype of the disease influences the recurrence rate is unknown. Yamamoto reported the 5-year recurrence rate after strictureplasty at 28%, with only a 3% site-specific recurrence rate. 43 Overall, the site-specific operation-free intervals is similar for patients who undergo resection or strictureplasty. 45
Clinical Application
The initial presentation of a patient with a single stricture or a series of strictures in a relatively short segment of intestine is most often best managed with surgical resection. The treatment of multifocal, extensive, and recurrent disease after prior resection is more complex and requires utilization of multiple different techniques, that is, strictureplasty and resection.
The first step in surgical planning is to develop a roadmap of the bowel, noting the length of the bowel involved, the degree of disease, and the number and location of strictures, previous resections, and strictureplasties. This must be done preoperatively with review of prior operative reports and radiologic and endoscopic assessments. This must also be repeated as the first step of the operation by examining the entire the bowel to identify the extent of disease as well as the extent of healthy intestine. The bowel must be visually inspected, palpated, and can be luminally evaluated by passing a partially inflated Foley or Fogarty balloon to identify more subtle luminal narrowings.
Gastroduodenal strictures may be alleviated with endoscopic dilatation. When surgery is needed, the Heineke-Mikulicz strictureplasty is ideally suited for short strictures throughout the first three portions of the duodenum; the Finney strictureplasty is best suited for strictures of the fourth portion of the duodenum by recruiting the first loop of jejunum. Full mobilization of the duodenum should be performed to allow for complete inspection of the duodenum and to facilitate strictureplasty. For longer strictures where a strictureplasty is not feasible, a gastrojejunal bypass is considered a viable alternative.
Jejunal-ileal strictures may be addressed with a combination of resection and strictureplasty techniques. For short segments, Heineke-Mikulicz strictureplasty is the procedure of choice. For longer segments, Finney strictureplasty is performed. The Michelassi strictureplasty is best used for multiple sequential strictures.
Terminal ileum and colon strictures are usually the result of inflammatory, nonpenetrating or penetrating, disease. As such a segmental resection is preferred.
Anastomotic strictures can be addressed with a strictureplasty if limited in extension. Adequate mobilization and lysis of adhesions must be performed to perform a tension-free strictureplasty at the site of the prior anastomosis. Anastomotic strictureplasty is safe and efficacious, but associated with a high rate of recurrence (57%) when followed long term. 46
Clinical case
An 18-year-old male with a history of CD presented with complaints of weight loss, abdominal pain, bloating, and nausea despite being on a liquid diet. He had a history of two previous extensive small bowel resections. Preoperative imaging revealed multiple strictures and dilated areas throughout the small bowel. At surgical exploration, he was found to have 208 cm of small intestine from ligament of Treitz to ileocecal valve. In the proximal 158 cm, there were 14 strictures and 6 diseased segments (extent of disease: 62″/82″, 76%; Fig. 5A).
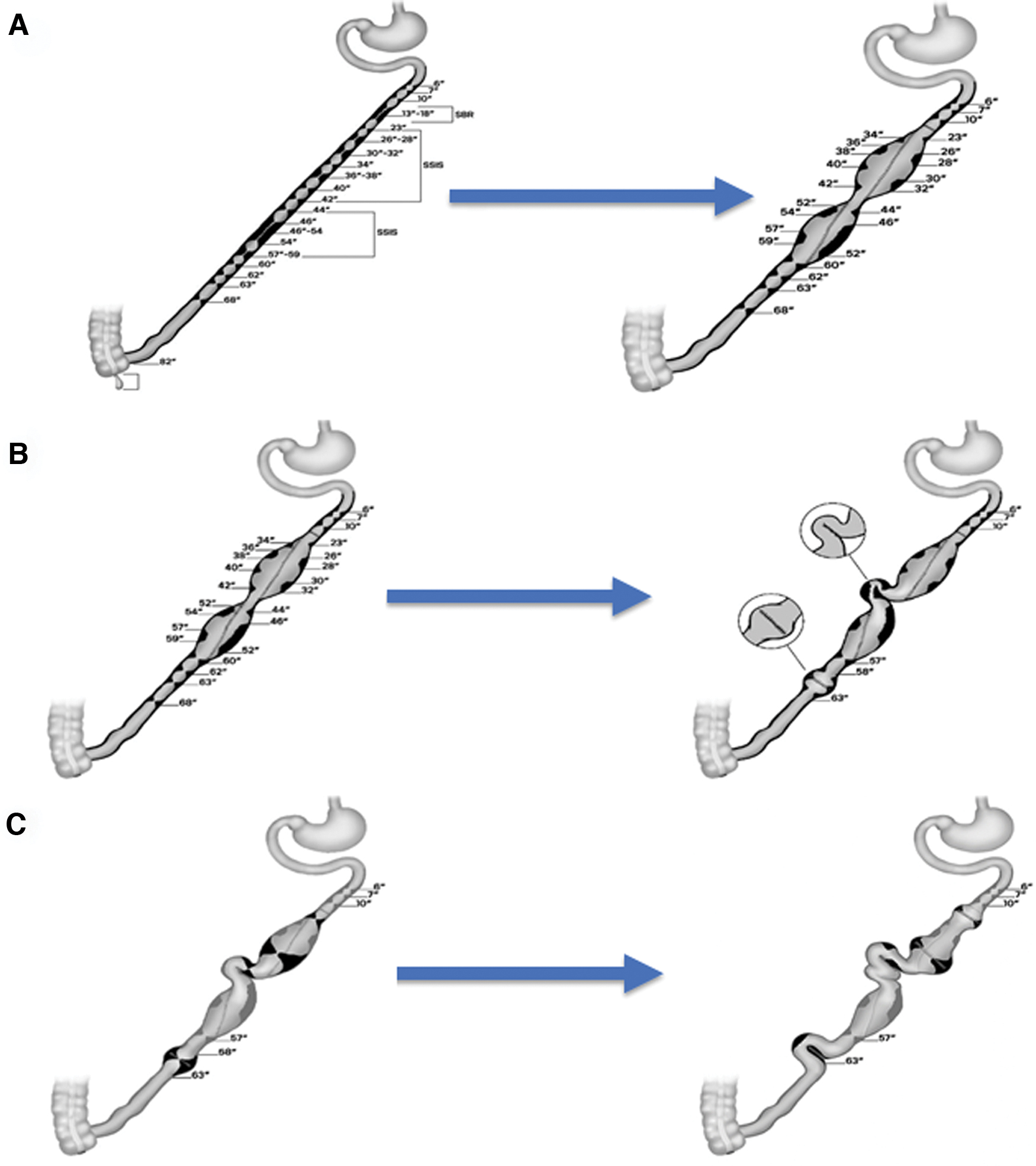
Clinical case.
The history of the patient and the findings at surgery prompted several observations and considerations: (1) small bowel severely shortened by two previous extensive bowel resections; (2) lengthy recurrence extending over three quarters of the small bowel consistent with the notion that the length of the recurrence is similar to the length of the index disease; (3) young patient, already experiencing a second surgical recurrence, hence likely to experience additional in the future.
The sum of all these considerations pointed to the necessity of using bowel sparing procedures as much as possible. The patient underwent a limited small bowel resection of a severely diseased intestinal loop between at 13 and 18 inches from the ligament of Treitz and two Michelassi strictureplasties (Fig. 5A). Three proximal and four distal strictures were left untouched because they appeared not to be critical.
Three years later, the patient returned with recurrent symptoms of chronic intestinal obstruction, abdominal pain, nausea, and weight loss. Preoperative imaging and intraoperative exploration revealed two areas of recurrence: one in between the two SSISs and one distal to the second SSIS, probably progression of one stricture that had been left untouched at the previous exploration. The same considerations as aforementioned led to perform a Finney and a Heineke-Mikulicz strictureplasty, respectively, on the two strictures (Fig. 5B).
Five years later, the patient developed recurrent symptoms of chronic bowel obstruction. Preoperative imaging and intraoperative exploration revealed three areas of recurrence: one in the body of the proximal SSIS, one at the outlet of the proximal SSIS, and one on the previous Heineke-Mikulicz distal to the second SSIS. Following identical considerations as aforementioned led to perform two separate Heineke-Mikulicz strictureplasties on the two more proximal strictures and a Finney strictureplasty on the strictured Heineke-Mikulicz strictureplasty (Fig. 5C).
In summary, this case exemplifies how strictureplasties are an indispensable surgical technique in the armamentarium of a surgeon dealing with CD. It also illustrates the recurrent nature of the disease and the need to apply bowel-sparing procedure especially in patients with extensive disease. Finally, it makes clear that strictureplasties can be performed on strictureplasties. The result for the example case is the loss of only 5 inches of bowel after three surgical procedures over the course of 8 years despite the presence of severe and recurrent disease.
No treatment is curative in CD and a combination of medical, endoscopic, and surgical (resection and strictureplasty) therapy is often required to address symptoms and complications. These treatments may be used simultaneously, sequentially, and repeatedly, and should be considered complementary.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.