
Abstract
Background:
Common bile duct exploration (CBDE) is performed uncommonly. Issues surrounding its uptake in the laparoscopic era include perceived difficulty and lack of training. We aim to determine the success of CBDE performed by “specialist” and “nonspecialist” common bile duct (CBD) surgeons to determine whether there is a substantial difference in success and safety.
Methods:
A 10-year retrospective audit was performed of patients undergoing CBD exploration for choledocholithiasis. Northern Health maintains an on-call available “specialist” CBD surgeon roster to aid with CBDE.
Results:
Five hundred fifty-one patients were identified, of which 489/551 (88.7%) patients had stones successfully cleared. Specialists had a higher success rate (90.8% versus 82.6%, P = .008), associated with a longer surgical time. Method (transcystic or transductal), approach (laparoscopic or open), and indication for operation were similar between groups. There was no significant difference in complications. To be confident of a surgeon having an 80% success rate, 70 procedures over 10 years were required, however, an “in-control” 50% success rate may only require 1 procedure per year.
Conclusion:
While specialist CBDE surgeons have improved success rates, nonspecialist general surgeons also have a good and comparable success rate with an equivalent complication rate. With realistic annual targets, nonspecialist CBD surgeons should be encouraged to perform CBDE in centers without specialist support.
Introduction
The treatment of common bile duct (CBD) stones is controversial with the traditional method of operative open CBD exploration being virtually replaced by endoscopic retrograde cholangiopancreatography (ERCP) when operative management of gallbladder disease transitioned to laparoscopic cholecystectomy ∼30 years ago. 1 Through pioneers, such as Rhodes and Nathanson (among others), laparoscopic CBD exploration techniques were developed with early studies demonstrating a benefit over ERCP in terms of success, time and resource cost, and decreased morbidity. 2 It was unclear at that stage whether these results were limited to skilled enthusiasts of the technique. More recent studies from varied global centers have confirmed the safety of CBD exploration with acceptable, if not superior, success and complication profiles than ERCP.3–6
Educating and training surgical trainees does not appear to be an impediment to learning CBD exploration, with evidence that surgical trainees can easily attain CBD clearance rates similar to experienced surgeons with training. 7 Despite this, lack of training and access to training is often cited as a reason why CBD exploration is uncommon.8,9 Learning curves of 10 cases for transcystic CBD exploration and 20 cases for choledochotomy have been used with little evidence to justify this level of experience.10,11 In other areas of surgery, including surgical oncology and hernia repair, subspecialization has been associated with improved outcomes.12,13 Despite evidence that specialization and centralization may improve outcomes, the issue of whether CBD exploration is within the domain of Hepato-Pancreatico-Biliary (HPB) surgeons or general surgeons, or both, continues to be debated.
The aim of this study was to evaluate the success and learning curve of surgeons with and without a special interest in CBD exploration in the setting of a single institution with strong CBD exploration support, including an on-call service for CBD exploration.
Methods
The study was performed as a retrospective audit at The Northern Hospital, Epping, Australia over a 10-year period (between September 2008 and September 2018). This study was assessed and approved by the Northern Health Research and Governance Office (ALR 35.2017). All patients undergoing cholecystectomy and CBD exploration were identified from hospital records using operation coding. Data, including age, gender, date of admission, date/time of operation, date of discharge, indication for operation, white cell count (WCC), C-reactive protein (CRP), American Society of Anesthesiology (ASA) grade, operative approach, stone clearance, and postoperative complications were recorded. Complications were recorded according to the Clavien–Dindo classification. 14 Surgical time was recorded routinely by theatre staff from the time of anesthetic handover to the surgeons to the time dressings were placed. Success was defined as the surgeon documenting that the biliary system was cleared at the end of the operation. Missed stones were defined as CBD stones found within 6 months of CBD exploration (CBDE) clearance, and recurrent stones were defined as CBD stones found after this time.
Intraoperative cholangiography is performed by all general surgeons at Northern Health. CBD exploration was performed on an ad hoc basis up until the end of 2012, depending on surgeon expertise available and decision making. Based on support from all surgeons, an on-call roster was developed in 2013, consisting initially of two general surgeons and two hepatobiliary surgeons, to be available to perform CBD exploration on any patient with CBD stones detected on cholangiogram. Patients were either identified preoperatively as having a high chance of requiring CBD exploration, with the attending surgeon negotiating operative timing with the on-call CBD surgeon, or patients were incidentally found to have CBD stones at cholangiogram, in which case the surgeon could elect to attempt exploration themselves, call in the on-call CBD surgeon, or arrange for postoperative ERCP. Over time, the on-call service has changed some personnel, and now consists of 2 general surgeons and 3 hepatobiliary surgeons. For the purposes of this article, any surgeon that has been a part of the CBD on-call service is deemed a CBD “specialist” surgeon, with other surgeons deemed “generalists.” Specialist surgeons were chosen based on a volunteer basis, and the prior experience and number of cases performed by all surgeons at other institutions during the study period was unknown. With the limitations of the study being performed as a retrospective audit and not knowing the roles played by surgeons listed on the operative report, CBD explorations performed under the direct supervision of the CBD specialist were deemed to have been performed by the CBD specialist if present. All other operations were deemed to have been performed by the consultant surgeon who was supervising the operation.
Laparoscopic cholecystectomies were performed with the standard four-port American technique with intraoperative cholangiography performed with iohexol (Omnipaque™, GE
Descriptive statistics were prepared to show differences between generalist and specialist operations. Student's t-tests or Mann–Whitney (rank sum) tests were used to test for differences in normally and non-normally distributed variables, respectively. Chi-squared or Fisher's Exact tests were used for categorical variables. The success rates for each surgeon were presented in a funnel plot, which provides a comparison of each surgeon's performance against the average pooled success rate, with control limits of 2 and 3 standard deviations (95% and 99.8% control limits) used to indicate the chance of exceeding these limits for an in-control surgeon, 15 according to the “exact” approximation for the conditional binomial distribution. 16 Stata v15.1 (StataCorp, College Station, TX) was used for the statistical analysis, with a two-sided P value of <.05 indicating statistical significance.
Results
In the 10-year period (September 2008 to September 2018), there were 597 patients in whom CBD exploration was attempted (Fig. 1). Of these 597 patients, surgeons performing the CBD exploration failed to cannulate the cystic duct or CBD and thus CBD exploration was abandoned in 13 cases. Of the remaining 584 patients, 49 (8.4%) patients had CBD stones identified visually at choledochoscopy, but attempts to clear the CBD failed. Both instances of either failed cannulation or failed clearance have been combined and labeled as failed CBD exploration. Of the other patients, 46 patients (7.7%) did not have stones confirmed at choledochoscopy, having undergone this procedure for a high clinical suspicion or a presumed stone identified on intraoperative cholangiography. These patients may have had stones or sludge that passed while manipulating and flushing ducts while commencing choledochoscopy, but for scientific integrity these patients have been excluded, leaving 551 patients for further analysis. Four hundred eighty-nine (88.7%) patients had CBD stones successfully cleared.
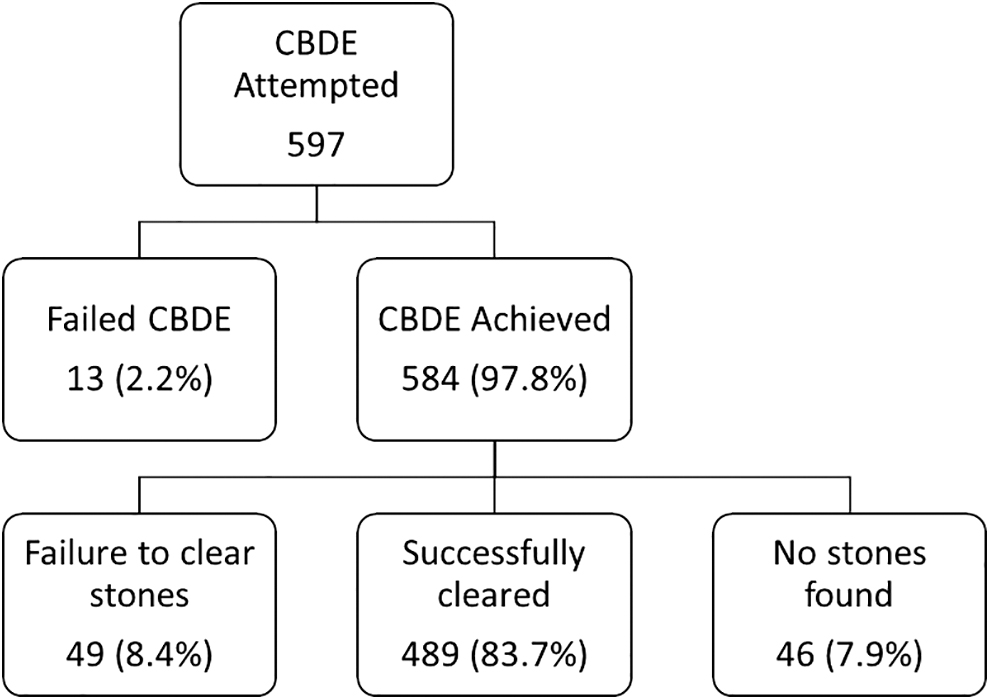
Patient flow chart.
Patients were divided into two groups depending on whether their CBD exploration was performed by a generalist or a specialist with the number of patients in each group being 138 (25.0%) and 413 (75.0%), respectively. Demographic information is listed in Table 1 with a slight observed increase in age in the specialist group (48.2 versus 52.0 years, P = .065). There was otherwise no difference between groups in terms of presentation, indication for operation, preoperative WCC, CRP, liver function tests, bilirubin, or ASA classification. There was an indication of more weekday operating and a significantly higher number of patients being operated on in-hours in the specialist group, which may reflect surgeons' preference for performing potentially more difficult and longer cases in daytime hours when more support is available and surgeons are more refreshed.
Preoperative Variables, n (%) Unless Otherwise Indicated
ASA not available for all cases.
ASA, American Society of Anesthesiology; CBD, common bile duct; CRP, C-reactive protein; CT, computed tomography; ERCP, endoscopic retrograde cholangiopancreatography; IQR, interquartile range; LFTs, liver function tests; MRCP, magnetic resonance cholangiopancreatography; MRI, magnetic resonance imaging; SD, standard deviation; US, ultrasound; WCC, white cell count.
There were no differences in the operative approach between generalists and specialists with both groups completing the operation laparoscopically in over 92% of cases (Table 2). In addition, the CBD method was predominantly through a transcystic approach with both groups performing this approach 88%–89% of the time. There was a significant difference in CBD clearance success between generalists and specialists (82.6% versus 90.8%, P = .008). This may also be related to the time taken to perform the operation, with surgical time also increased in the specialist group (161 versus 186 minutes, P < .001). Clavien–Dindo grade 1 and 2 complications were observed to be higher in the specialist group (8.7% versus 4.4%), but overall there was no difference in complications between the two groups. Technical complications of bile leak and bile duct strictures were not common with no differences between the groups.
Operative and Postoperative Outcomes, n (%) Unless Otherwise Indicated
CBDE, common bile duct exploration; IQR, interquartile range; SD, standard deviation.
To address the issue of a learning curve, success rates of individual surgeons were compared using a funnel plot (Fig. 2), according to the number of procedures conducted over the 10-year study period. The funnel plot indicates considerable variability in the observed success rate for surgeons conducting fewer than 50 procedures. Three surgeons are observed to have conducted a minimum of 100 procedures, and since they conducted over 50% of all procedures over the 10-year period, they have the greatest effect on the pooled average success rate of 88.7%. The majority of specialist CBD surgeons had individual success rates above the pooled average success rate. If a clinically acceptable minimum success rate is considered to be 80%, a surgeon would be required to perform a minimum of 70 procedures over a 10-year period. However, a surgeon performing 10 procedures over a 10-year period would only need to demonstrate a success rate of 50% to be within 95% confidence intervals.
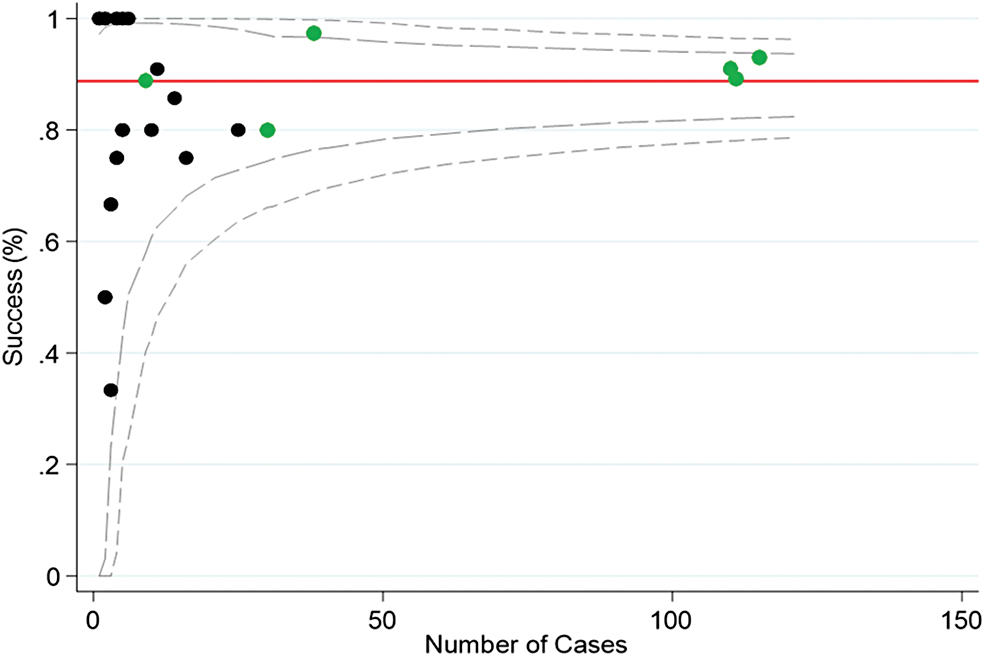
Funnel plot of CBD exploration success by individual surgeons according to number of procedures performed between September 2008 and September 2018 (green dots indicate a specialist CBD surgeon, black dots indicate a nonspecialist CBD surgeon). CBD, common bile duct. Color images are available online.
If, given the high number of cases required and number of cases available, it is considered feasible that specialist CBD surgeons are required to perform the service, then the question would be raised as to whether these specialists should have HPB training experience. When we compared the specialist CBD surgeons depending on whether they had an HPB training background or not, we found no difference in the failure rate of HPB surgeons compared with non-HPB surgeons (8.1% versus 10.6%, P = .242) (Fig. 3). There was also no difference in complication rate, including bile leak and stricture rates.
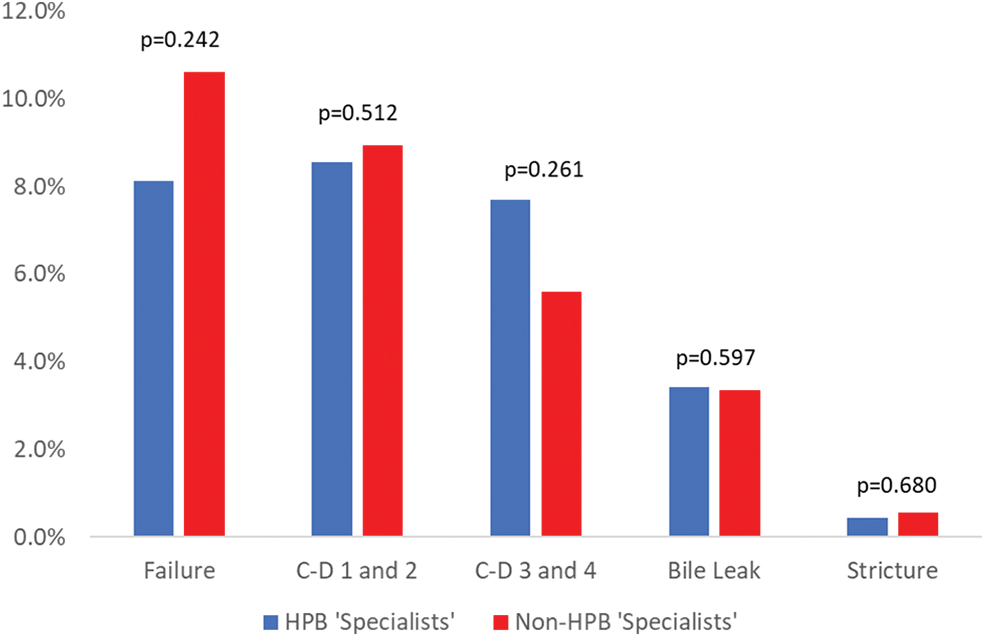
Comparison of failure and complications between HPB and non-HPB CBD specialists. CBD, common bile duct; HPB, Hepato-Pancreatico-Biliary. Color images are available online.
Discussion
The treatment of CBD stones is controversial with accepted methods, including ERCP before, during, and after cholecystectomy, as well as operative methods of clearing the CBD during index cholecystectomy, leading to a wide variety of clinical practice.17–19 This study reports the outcomes in a “pro-”CBDE institution and, like others, has shown that CBD exploration can be performed safely with minimal morbidity with a majority of the procedures being performed in the emergency setting.
In this study, we looked specifically at whether CBD specialist surgeons would be more appropriate to perform all CBD explorations. The overall cohort of patients undergoing CBDE is the highest reported in the literature to our knowledge,20,21 with a good number of procedures done by both specialist CBD surgeons and nonspecialists. Compared with other studies with success rates as high as 88% to 98.6% but in meta-analysis was 74.4%,18,21–24 the success rate for nonspecialist surgeons was still good, with an 82.6% success rate ultimately leading to that number of patients avoiding a postoperative ERCP. While there was a significantly higher success rate of 90.8% in specialist surgeons, this did not translate into a decreased morbidity rate, and would support CBD exploration being available to all surgeons who felt they had the expertise and skill to attempt this. While there is no literature to directly support this claim, we suspect the technique of using the choledochoscope as described in our methods is superior to radiologically guided techniques such as using the Nathanson basket.
The success rate may be tempered, however, by the design of this study, with the retrospective nature not able to detect the number of attempts by nonspecialist surgeons who then ultimately called in a specialist surgeon for assistance. Thus, the true success rate for nonspecialists may be lower. This may be the explanation for the discrepancy in surgical time between the two groups, with extra time required for the specialist surgeon to be present, although the majority of CBD explorations were performed during the week in daylight hours when a specialist is often at hand. The increased time is favored to represent a more thorough attempt to clear stones resulting in the higher success rate. There are undoubtedly some cases, which were preoperatively suspected to be difficult cases and were triaged to a specialist to perform, although it is unclear how many of these cases there were and how they reflect in the results.
The definition of success is also argued, with it sometimes impossible to tell whether CBD stones detected following CBD clearance (by any means) are new stones, or stones that were missed previously. More recent literature defines presumed missed stones as any CBD stone detected within 6 months of CBD clearance and those found after that time deemed recurrent stones.25,26 There is little if any literature regarding recurrent stones after CBDE, and we report very low rates of missed or recurrent CBD stones when compared with post-ERCP sphincterotomy rates, which can range between 4% and 25% but which appear to be around 6%–8% in larger studies.25,26
There are thoughts that CBD exploration should be limited to HPB surgeons. 27 However, non-HPB surgeons with a special interest in CBD exploration have also been reported as having good outcomes, with our study showing excellent results when compared with the literature. 28 In health services with large number of patients with choledocholithiasis, we would advocate for any general surgeon with an interest in CBD exploration to pursue this interest given that our study demonstrates no difference between specialist HPB surgeons or specialist CBDE general surgeons. Our study has shown that ∼70 patients over a 10-year period would be required per surgeon to provide a meaningful lower control limit of 80% success in which to monitor surgeon performance, thus it may not be practical for all health systems to adopt a model requiring specialist CBD surgeons. In this case, the success rate for a surgeon conducting 10 procedures over a 10-year period would only need to be greater than ∼50% to be considered an in-control surgeon according to the lower bound for the 95% confidence control limit. This still allows for a reasonable number of patients avoiding the risks of ERCP without subjecting the patient to a low success procedure.
This study is limited by the retrospective nature of its design. While our institution encourages single-stage laparoscopic cholecystectomy and CBDE, we were not able to detect and account for patients that were treated as a two-stage procedure with ERCP either pre- or postlaparoscopic cholecystectomy. The limitations of relying on the operative report have already been mentioned regarding the potential failure of a nonspecialist, and in addition it would be useful to know the time taken for the CBDE component of the operation, the choledochoscope operator (trainee versus specialist), and whether multiple surgeons attempted exploration. Our definition of CBD specialist was made on whether they contributed to our on-call service, which may have unfairly excluded those CBDE enthusiasts who perform a large number of cases at other institutions. A prospective database is in production to answer these issues in the future.
In conclusion, this study has demonstrated that specialist CBD surgeons have a higher success rate, although no difference in morbidity, when compared with generalist surgeons in performing CBD exploration. Generalist surgeons still maintain a high level of success, however, and due to the practicalities of having an on-call CBD specialist available, generalists should be trained and encouraged to perform CBD exploration.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.