
Abstract
Background:
Over the last decade, a significant rise in pediatric robot-assisted minimally invasive surgeries has been observed. Apart from the urological surgeries in children, robot assistance for complex nonurological reconstructions is being explored increasingly. This study highlights our preliminary experience of robot-assisted minimally invasive surgeries in children.
Materials and Methods:
An ethical waiver was given by the Institute's Ethics Committee in view of the retrospective nature of the study and all procedures being performed as a part of the routine care. A retrospective analysis was done to include all the pediatric robot-assisted surgeries performed at our hospital over a 4-year period (January 2017–January 2021). The surgeries were categorized based on the involved organ system and the total study duration was divided into four 12-month time periods. A comparison of the total number of surgeries done in each time period was also done. A log of the surgeon's console duration for each surgery was also kept.
Results:
A total of 65 patients, with the majority (50/65; 77%) undergoing reconstructive surgeries for anomalies within the genitourinary system, were included. Almost two-thirds of the total surgeries were technically complex. The number of procedures performed during the four 12-month time periods was 18, 18, 15, and 14. The average (range) surgeon's console time was 95 minutes (45–327 minutes) and showed a progressive improvement with the passage of time. Only 1 patient required conversion to an open approach, and none had major complications during the postoperative period.
Conclusion:
Our early experience of robot-assisted minimally invasive surgeries in children reaffirms its safety and feasibility in complex reconstructive surgeries. It also highlights the advantages of robot assistance in smaller children with nonurological anomalies.
Introduction
Following the first robot-assisted surgery in the 1980s, the proportion of surgeries performed with robot assistance in adults is gradually increasing.1,2 In recent years, a similar trend has been observed in pediatric robotic surgeries. 3 The Pediatric Health Information System (PHIS) data, from 19 children's hospitals in the United States, depict a significant rise in the utilization of surgical robots for performing pediatric surgeries in the last decade. 3 Nonurological complex reconstructive surgeries in children are also increasingly performed under robot assistance.3,4
Although various case reports and case series have been published, comprehensive data from India is lacking.5–9 In the present study, we aim to present our initial experience of robot-assisted minimally invasive surgeries in children. We also intend to highlight the feasibility and advantages of performing complex surgical procedures in smaller children under robot assistance.
Materials and Methods
Our center is equipped with two surgical robots made by Intuitive Surgical (Sunnyvale, CA), an older da Vinci Si and a newer da Vinci Xi system since 2012 and 2017, respectively. These robots are used by nine different specialties (Pediatric Surgery, Urology, Uro-Oncology, Gynecology, Gynecological Oncology, Otorhinolaryngology, Head and Neck Oncology, General Surgery, and Gastrointestinal (GI) surgery) to perform various surgeries. The department of Pediatric Surgery has been performing robot-assisted minimally invasive surgeries w.e.f. January 27, 2017. A retrospective analysis was done to include all the pediatric robot-assisted surgeries performed at our hospital over a 4-year duration (January 2017–January 2021). All the surgeries in children were performed by a single surgeon. Written informed consent and assent were obtained from parents and subjects, respectively. The ethical waiver was given by the Institute's Ethics Committee in view of the retrospective nature of the study and all procedures being performed as a part of the routine care.
Categorization of the robotic surgeries
For the purpose of this study, all the surgeries were categorized based on the involved organ system. The categories included genitourinary (GU), GI, and non-GU oncology (Table 1). Procedures were defined as technically complex surgical procedures based on a previous study. 4 The total study duration was divided into four 12-month time periods. A comparison of the total number of surgeries done in each time period was also done.
System-Wise Distribution of the Robotic Surgeries
Three additional procedures: bladder neck closure with appendicovesicostomy and augmentation cystoplasty (n = 1); cystoscopy with retrograde pyelography (n = 1) and pyelolithotomy (n = 1).
Majority (23/50; 46%) were extravesical.
GI, gastrointestinal; GU, genitourinary.
Statistical analyses
The continuous data were presented as mean (range) if normally distributed, and median (range), if data were nonlinear. Categorical variables were presented as frequency and percentages. Data entry was done in an extraction table using MS Excel (Version 15.24). IBM SPSS Statistics software version 26 (IBM Corp., Armonk, NY) was used for statistical analyses.
Results
A total of 65 patients underwent robotic surgeries during the study period. Of these procedures, 63% (41/65) were technically complex procedures. The median (range) age of the cohort was 36 months (1 month–21 years) with a male gender preponderance (44/65; 68%). In addition, 58% (38/65) of the overall cohort and 53% (8/15) of the children with nonurological anomalies were <36 months of age at the time of surgery. The procedure-wise age distribution of the study population is depicted in Supplementary Table S1. The weight of the cohort ranged from 3 to 55 kg. Twelve different types of surgical procedures, all involving the abdominal domain, were performed in these patients. Of these, 77% (50/65) were pertinent to the GU system. Within the GU system, the most common procedures performed at our center were ureteric reimplantation (52%; 26/50) followed by pyeloplasty (38%; 19/50). Besides this, 17% (11/65) of the patients underwent robotic surgeries involving the GI system. A detailed organ system-wise distribution of the robotic surgeries is depicted in Table 1.
The number of procedures performed during the four 12-month time periods was 18, 18, 15, and 14. The distribution of robotic surgeries with respect to time is depicted in Figure 1. The operation room time ranged from 50 minutes to 6 hours. The average (range) surgeon's console time was 95 minutes (45–327 minutes). The variation of average console time of different surgeries over the study duration is depicted in Table 2. The average docking and undocking durations were 15 and 1 minute, respectively.
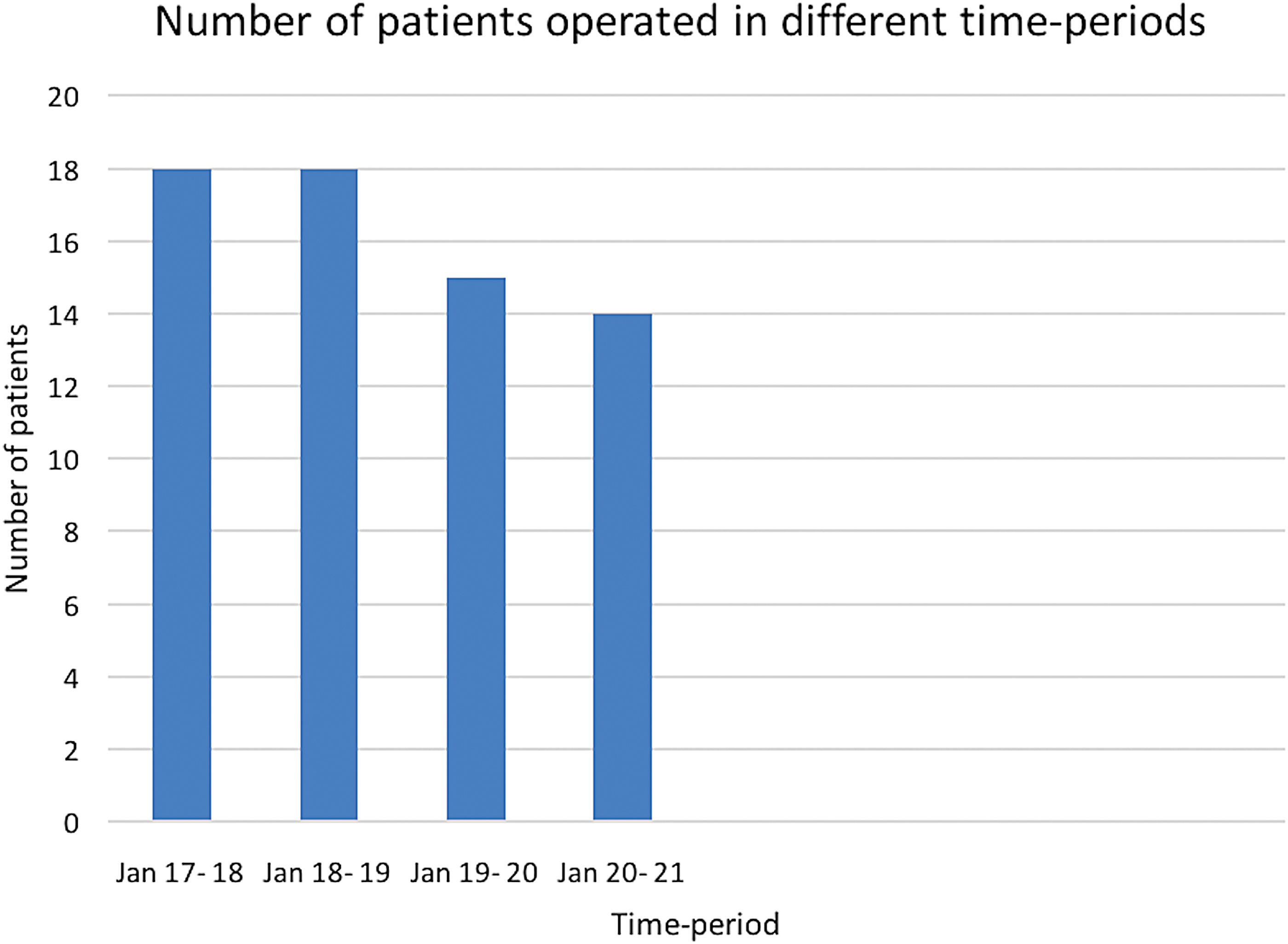
Number of patients operated in different time period. Color images available online.
Surgeon's Console Duration of the Robotic Surgeries
Complex reconstruction also involving bilateral ureteric reimplantation, bladder neck closure and appendicovesicostomy.
B/L, bilateral; U/L, unilateral.
Of all the 65 surgeries that were attempted using robot assistance, only 1 (1.5%) procedure was converted to an open approach. The patient was a 6-year-old child with right adrenal neuroblastoma. Transition to open exploration was performed to control the hemorrhage from an aberrant vein, which was draining the tumor and joining the inferior vena cava. Postoperative course was uneventful in the majority of cases apart from minor complications, including port-site dehiscence (n = 1), omental prolapse after removal of the abdominal drain (n = 1), and biliary gastritis (n = 1).
Discussion
The first pediatric robot-assisted surgery was performed by Meininger et al. 10 Owing to its benefits, including minimal blood loss, less postoperative pain, decreased incidence of complications, and shorter hospital stay, it gained popularity among pediatric surgeons and pediatric urologists in a short span of time. However, a few series were published until 2008, when Meehan and Sandler described their comprehensive experience of 100 consecutive pediatric robotic cases. 11 Of the total cases reported by the author, 89% were restricted to the abdominal domain. The most common procedure performed by robot assistance was fundoplication. However, ureteric reimplantation followed by pyeloplasty were the most common procedures in the present series. On comparing the patient characteristics, the median age of children in our study (36 months) was found to be considerably less as compared with the previously published literature.4,11 Also, more than 50% of our patients were <3 years of age at the time of surgery. These findings are in contrast with some previous studies, where age <3 years was one of the exclusion criteria for consideration for robotic approach. 4
The last decade has witnessed a steep rise in the proportion of surgeries performed by robot assistance. 3 The majority of the surgeries in children, which were earlier performed by conventional laparoscopy, are now performed under robot assistance. Of these, renal pelvis/ureter and foregut surgeries have shown the maximum increase in the utilization of the robot. In contrast, the mediastinal and thoracic surgeries in children have shown a significant decline in the utilization of the robot. Other urologic procedures, biliary reconstructive surgeries, and splenic surgeries have shown a similar utilization of the robot over time. 3 In a review by van Haasteren et al., the author has highlighted the feasibility and advantages of robot assistance in complex reconstructive surgeries. 4 In the present series, 63% (41/65) of the cases were technically complex procedures, including choledochal cyst excision, right hepatectomy, ureteric reimplantation, Duhamel's procedure, and so forth.
As compared with a similar single institutional experience, 11 we had performed a similar number of cases during the first time period (first 12 months). However, unlike the study by Meehan and Sandler, 11 a subsequent rise in the next 12 months was not observed. This is probably due to the presence of a single experienced consultant at our center. A further fall in the number of robotic surgeries in the next two time periods (Fig. 1) is due to the curtailed elective services during the COVID-19 pandemic.
The average (range) surgeon's console time in the present series was 95 minutes (45–327 minutes). Moreover, if we exclude the console duration of the two surgeries, which required extensive reconstruction (right hepatectomy and augmentation cystoplasty), the average console duration was 88 minutes. Similar results have been depicted in a previous comprehensive experience by Meehan and Sandler. 11 The present series also shows an improvement in the console duration of specific surgeries with the passage of time, highlighting the experience of the operating surgeon (Table 2). This was even observed while performing complex reconstructive surgeries like choledochal cyst excision, ureteric reimplantation, and so forth.
The present study not only demonstrates the safety of robot-assisted minimally invasive surgery in children but also reaffirms its feasibility in nonurological procedures. Second, the considerably low average age of our cohort shows its safety in smaller children. Finally, as per the previous definitions, almost two-thirds of these procedures were categorized as technically complex. Fine dissection, easier access to deep-seated structures, and easy suturing are the advantages of robot assistance in these complex procedures. 4
The results of the present study should be interpreted within the context of few limitations. First, it is a retrospective study with limited sample size. Second, it is an audit of robot-assisted surgeries in children and provides limited clinical data (including weight at presentation) and operative details. Third, it demonstrates a single surgeon experience of robot-assisted minimally invasive surgeries in children. It is well known that there is a learning curve associated with each robotic procedure, and the nuances related to a specific procedure need to be learned by the operating surgeon. Therefore, these results cannot be generalized; specially to centers that have recently started performing robot-assisted minimally invasive surgeries. Finally, the current study provides a glimpse of the safety and feasibility of the robotic approach in complex reconstructive pediatric surgeries. Prospective multicentric studies with a larger sample size need to be conducted before definite conclusions are drawn.
Conclusion
Our early experience of robot-assisted minimally invasive surgeries in children reaffirms its safety and feasibility in complex reconstructive surgeries. It also highlights the advantages of robot assistance in smaller children with nonurological anomalies.
Footnotes
Authors' Contributions
G.S. contributed to study conception and design. Data acquisition was performed by S.A. and B.J. Analysis and interpretation of data were done by G.S., V.B. and M.T. Drafting of the article was performed by S.A., V.B., and M.T. Article was revised by G.S. and S.H. The final draft of the article was read and approved by all the authors.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.