
Abstract
Background:
Renal stone disease is a common disorder in urology practice. Kidney stone has various treatment methods such as extracorporeal shock wave lithotripsy, retrograde intrarenal surgery, and percutaneous nephrolithotomy (PCNL). In this study, we aimed to determine the value of S.T.O.N.E. nephrolithometry score, which is considered as a new scoring system for predicting residual stone rate and complications in patients undergoing PCNL due to renal calculi.
Materials and Methods:
A total of 120 patients >18 years old who underwent PCNL were evaluated prospectively. Five parameters available from preoperative noncontrast-enhanced computed tomography were measured: stone size (S), tract length (T), obstruction (O), number of involved calices (N), and essence or stone density (E) and then S.T.O.N.E. nephrolithometry score was calculated. The prediction of the stone-free rates and complication rates of this scoring was evaluated statistically.
Results:
When the age, gender, body mass index, comorbidities, and American Society of Anesthesiologists scores of the patients were evaluated according to the patients' postoperative stone-free status, no statistical difference was found between the groups. Patients had a stone-free rate of 78%. Patients' mean neuropilitometry score was calculated to be 7.75 S.T.O.N.E. nephrolithometry score statistically significant (P = .001) for prediction of stone-free status. S.T.O.N.E. nephrolithometry score was significantly correlated with operation time, estimated blood loss, duration of fluoroscopy, duration of hospital stay, and number of punctures. Complications were seen in 13 patients.
Conclusions:
S.T.O.N.E. nephrolithometry score can be used as an objective criterion for predicting the complexity of the PCNL process. In addition, this scoring system is expected to provide more objective preoperative counseling and can provide standardization in academic studies.
Introduction
Urinary system stone disease, first encountered in 4800 BC, is one of the most common diseases in daily urology practice. 1 Kidney stone disease affects about 1%–5% of the people in industrial societies. 2 In a multicenter study from Turkey, its prevalence has been reported to be 14.8%. 3
Various methods including extracorporeal shock wave lithotripsy (ESWL), retrograde intrarenal surgery, and percutaneous nephrolithotomy (PCNL) are used in the treatment of kidney stones. PCNL is a treatment modality used for the kidney stones larger than 2 cm in diameter, ESWL-resistant kidney stones, multiple kidney stones, and staghorn stones. 4 The success rate of PCNL has been reported to be >95%. 5
Factors affecting the success rate of PCNL include anatomy of the kidney, size, location, and structure of the stone, patient's anatomy, and surgical experience. As with any surgical procedure, complications may develop during and after PCNL. Bleeding, hydrothorax, adjacent organ injury, collecting system perforation, fever, urine leakage, and problems arising from residual stones can be listed among these complications. 6
Various scoring systems have been developed to predict preoperative complications and the number of residual stones in the treatment of upper urinary tract stones. 7 There is no internationally accepted scoring system to be used for patients with kidney stones. In this study, S.T.O.N.E. nephrolithometry scoring system, developed by Okhunov et al. 8 was used. Five parameters available from preoperative noncontrast-enhanced computed tomography (CT) were measured: stone size (S), tract length (T), obstruction (O), number of involved calices (N), and essence or stone density (E) (S.T.O.N.E.). As a result of this evaluation, a score ranging from 5 to 13 was obtained. 8
This study aimed to determine the value of S.T.O.N.E. nephrolithometry score, considered as a new scoring system to predict residual stone ratio and complications in patients undergoing PCNL for kidney stones.
Materials and Methods
This study was carried out with the Okmeydani Training and Research Hospital Ethics Committee's approvel dated November 17, 2015 and numbered 357.
This study included patients >18 years of age, who were admitted to the urology outpatient clinic of Okmeydani Training and Research Hospital between December 14, 2015, and June 14, 2017, due to kidney stones and underwent PCNL. Preoperative comorbidities, previous surgical interventions, body mass index (BMI), and American Society of Anesthesiologists (ASA) scores were evaluated. Patients, who underwent an open, endoscopic, or laparoscopic intervention to the kidney with stones previously, and those with a nephrostomy tube or ureteral stent, were excluded from the study.
Noncontrast-enhanced CT of the upper abdomen routinely taken before surgery was evaluated based on S.T.O.N.E. nephrolithometry score. Five parameters corresponding to the first letters of “S.T.O.N.E.” were evaluated: stone size (S), tract length (T), obstruction/hydronephrosis (O), number of involved calices (N), and essence or stone density (E).
Stone size was calculated by multiplying the length and width of the stone in CT in square millimeters (mm2). Stone size was scored as 1 (0–399 mm2), 2 (400–799 mm2), 3 (800–1599 mm2), and 4 (≥1600 mm2). The tract length was measured as the distance from the center of the stone to the skin in the vertical direction on CT scans. This value was scored as 1 for ≤100 mm and 2 for >100 mm. Obstruction/hydronephrosis, the third variable, was scored according to the degree of width in the collecting system. Absence of hydronephrosis or mild hydronephrosis was scored as 1, and moderate or advanced hydronephrosis as 2. As the fourth variable, the stone was evaluated for number of involved calices. If one or two calices were involved, one point was assigned; if three calices were involved, two points were assigned; and if it was a staghorn stone, three points were assigned. Density/essence of the stone on CT was measured in Hounsfield units (HUs). One point and two points were assigned for ≤950 HU and >950 HU, respectively.
The S.T.O.N.E. nephrolithometry score was calculated by summing the scores from each variable, with the lowest score of 5 and highest score of 13. This score was divided into three groups: low (5–6–7), medium (8–9–10), and high (11–12–13).
Perioperative operation time, percutaneous access number, time of fluoroscopy use, estimated blood loss, intraoperative complications, postoperative complications, length of nephrostomy tube stay in place, and length of stay in hospital were evaluated. Residual stone status was evaluated by intraoperative fluoroscopy or postoperative direct urinary system radiography (DUB) for opaque stones, and by postoperative CT for nonopaque stones. Residual fragments of 4 mm and below after PCNL were accepted as stone free. The correlation of S.T.O.N.E. nephrolithometry score with stone-free and complication status was investigated.
Statistical analyses were performed using SPSS version 15.0 software (SPSS for Windows, 15.0; SPSS Inc., Chicago, IL). Student's t-test, chi-square test, and correlation analysis were used for the analysis of data. A P value of <.05 was considered statistically significant.
Results
A total of 120 patients, who underwent PCNL in our clinic between December 14, 2015, and June 14, 2017, were included in the study. Considering the demographic characteristics of the patients, the mean age was 45.2 years. Of the patients, 58.3% were male and 41.7% were female. The mean BMI value was 27.2 (23–31) kg/m2. There was hypertension in 35% of the patients and diabetes mellitus in 25%. The ASA scores of the patients were as follows: ASA I in 55%, ASA II in 37%, and ASA III in 8%. There was no statistically significant difference between the patients in terms of age, gender, BMI, comorbidities, ASA score, and postoperative stone-free status (Table 1).
Patients Demographic and Clinical Data
ASA, American Society of Anesthesiologists; BMI, body mass index; HU, Hounsfield unit.
The postoperative stone-free status and operation data of the patients were evaluated. Operation time, fluoroscopy time, estimated blood loss, and length of stay were higher in patients with residual stones. However, there was no significant difference in terms of the number of punctures (Table 2).
S.T.O.N.E. Nephrolithometry Score and Residual Stone Status
HU, Hounsfield unit.
The mean stone size was 445.3 mm2 in the stone-free group and 1154.8 mm2 in the group with residual stones. Stone size was found to be statistically higher in patients with residual stones (P = .001). The number of involved calices was one or two in 60% of the patients and three in 14% of the patients, whereas staghorn stones were identified in 26% of the patients,. When the number of calices was evaluated according to the stone-free status, a statistically significant difference was found between the groups (P = .001). The mean tract length was 98.3 cm in the stone-free group and 97.9 cm in patients with residual stones, and there was no statistically significant difference between the two groups in this regard. When the presence of hydronephrosis was evaluated according to the stone-free status, no statistically significant difference was observed between the groups (P = .18). The mean stone density/essence was 875.6 HU in the stone-free group and 1044.8 HU in the group with residual stones. Stone density was statistically significantly lower in the stone-free group (P = .011).
The mean S.T.O.N.E. nephrolithometry score was calculated to be 7.75. The S.T.O.N.E. nephrolithometry score alone was found to be statistically significant in predicting stone-free status (P = .001). Distribution of the S.T.O.N.E. nephrolithometry scores of the patients is summarized in Figure 1.
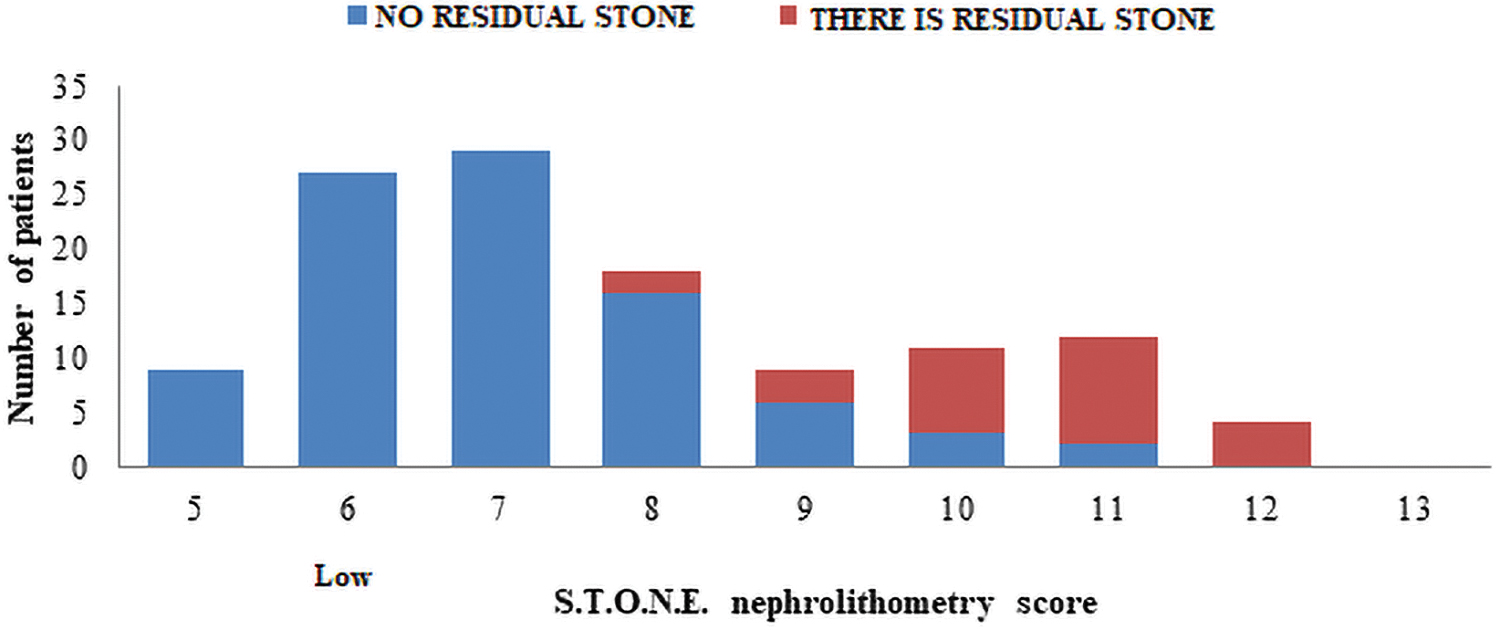
Distribution of the S.T.O.N.E. nephrolithometry scores of the patients. Color images are available online.
The S.T.O.N.E. nephrolithometry scores and operation-related data are presented in Table 3 The S.T.O.N.E. nephrolithometry score was found to have a significant correlation with operation time, estimated blood loss, fluoroscopy time, length of stay, and number of punctures.
S.T.O.N.E. Nephrolithometry Scores and Peri- and Postoperative Data
Only 1 patient developed a major bleeding complication requiring intervention. A total of 13 patients were observed to develop complications: postoperative fever in 5 patients, bleeding requiring transfusion in 2 patients, need for a stent in 4 patients, prolonged leakage in 1 patient, and urinary retention in 1 patient.
Discussion
The use of PCNL has been increasing in the treatment of patients with kidney stones, thanks to its advantages including high success rates, a short length of hospital stay and recovery time, small surgical incision, and almost no scar tissue being left.
The main purpose of the success of this surgical procedure is to achieve maximum stone-free status and minimum morbidity. Many factors affecting this success have been evaluated in the literature. In a study by Goldwasser et al. 9 investigating the factors affecting the success of PCNL, the authors investigated the effects of chemical structure of the stone, history of open renal surgery on the same side, and lithotriptor used on the success rate, and emphasized that success rate was affected by the size and localization of the stone.
Various scoring systems have been developed for the evaluation of patients before PCNL. These include Guy's symptom score (GSS), Clinical Research Office of Endourological Society (CROES) nomogram, S.T.O.N.E. nephrolithometry score, and Seoul National University Renal Stone Complexity score. These nomograms allow the surgeon to evaluate possible postoperative and preoperative complications and surgical success, and to share them with their patients. They further allow the operation results to be standardized and compared with other series. There is no internationally accepted scoring system to be used for patients with kidney stones. In these scoring systems, factors such as stone size, caliceal anatomy, number of involved calices, the degree of hydronephrosis, stone density, the distance of the stone from the skin, and the experience of the surgeon were evaluated on DUB, intravenous pyelography, and CT scans taken during the preoperative period.8,10–12
In this study, S.T.O.N.E. nephrolithometry scoring system, developed by Okhunov et al., 8 was evaluated. Five parameters are evaluated on preoperative noncontrast-enhanced CT scans: stone size (S), tract length (T), obstruction (O), number of involved calices (N), and essence or stone density (E). As a result of this evaluation, a score ranging from 5 to 13 is obtained. 8 Unlike other scoring systems, score is easily calculated and there is no need for additional software.
In the literature, clinically insignificant residues definition is used to evaluate post-PCNL success rate. This definition is generally used for stone particles <4 mm that do not cause infection, pain, or obstruction. The presence of stone-free or CIRF after PCNL is accepted as “success,” and the presence of particles >4 mm is accepted as “failure” because 85% of stones <4 mm are reported to pass without causing clinically symptomatic pain.13,14 In this study, the presence of particles <4 mm after PCNL was accepted as “stone free.” The evaluation of PCNL series shows that the success rate varies from 72% to 98%.15,16 The stone-free rate has been reported to be 60% by Müslümanoğlu et al. 17 and 77% by Ünsal et al. 18 in the first PCNL studies from Turkey. Compatible with the literature, the success rate in this series was found to be 77.3%.
There are many factors affecting the success rate of PCNL, but the most important one is the stone burden. Kim et al. 19 reported the success rate of PCNL as 88%–91% in stones measuring 1–3 cm and this rate could decrease to 75% in those measuring >3 cm.
In a study by Özçift et al., 20 the need for additional treatment was found to be 9.6% when the stone size was square centimeter (cm2), whereas this ratio increased to 17.4% for stones measuring >10 cm2. In the same study, 6.6% of simple stones were reported to require additional treatment, whereas 16.5% of complex stones did not. 20
In a study by Akhavein et al. evaluating the S.T.O.N.E. nephrolithometry score, CIRF rate was reported to be 81% for stone size of 0–399 mm2, 82% for stone size of 400–799 mm2, 75% for stone size of 800–1599 mm2, and 59% for stone size ≥1600 mm2. 21 In this study, the stone burden of the patients was calculated according to the mean surface area and these stones were divided into four groups according to their size. A statistically significant difference was found between these four groups in terms of PCNL success rate (P = .001).
In a study by Goldwasser et al. 9 published in 1986, the factors affecting the success of PCNL were investigated and success rate was emphasized to be affected particularly by the size and localization of the stone. Özçift et al. 20 classified stones based on their location in the kidney: simple stones (single calix or pelvic stones) and complex stones (coraliform, partial coraliform, pelvis + calix stones, or multiple calix stones), and reported stone-free rate as 82.4% in simple kidney stones and 59.6% in complex kidney stones in the 3rd month after PCNL. In a study by Akhavein et al., 21 the stone-free rate was reported to be 95% in patients with stones in a single calix, 90% in those with stones in two or three calices, and 63% in those with staghorn stone. In this study, the stone-free rate was 98% in patients with stones in one calix or two calices, 82% in those with stones in three calices, and 34% in those with staghorn stone, and there was a statistically significant difference between these groups (P = .001).
In complex stones, although access is easy in hydronephrotic systems accompanied by large stones, the failure rate increases as the stones can escape to other calices. 22 Zhu et al. 23 reported that the presence of obstruction or hydronephrosis significantly affected the stone-free rate after PCNL. In this study, multivariate analysis showed that the presence of moderate/severe hydronephrosis was insignificant alone in predicting stone-free status and complications (P = .18).
Tract length is an important parameter for predicting the success rate of PCNL. Increased tract length makes many stages of surgery difficult, from puncture to dilatation. 24
Increased nephrostomy tract length reduces nephroscope maneuverability and can lead to lower stone-free rates and increased complication rates, as well as longer procedures. 25 In a study by Zhu et al., 23 in which they applied S.T.O.N.E. nephrolithometry to the patients, tract length alone was found not to be statistically significant in predicting stone-free status and complications. Similar results were obtained in this study.
Another parameter measured within the scope of S.T.O.N.E. nephrolithometry is stone density measured in HU on CT scans. HU can be used to evaluate the CT density of urinary tract stones. In recent years, HU has become an important diagnostic tool not only for predicting the stone type but also for determining the most suitable treatment. Gücük et al. 26 investigated various factors, including HU, and concluded that the HU value was an independent factor affecting PCNL success. The authors further reported that there was a positive correlation between the HU value and bleeding, and this was associated with an increased frequency of endoscopic manipulation for stone removal. 26 In a study by Akhavein et al. 21 evaluating the S.T.O.N.E. nephrolithometry score, stone density alone was found not to be significant in predicting stone-free status and complications. Similarly, there was no significant correlation between stone density and PCNL success in this study (P = .001).
In many studies, the S.T.O.N.E. nephrolithometry scoring system defined by Okhunov et al. 8 has been reported to be a valuable tool in predicting stone-free status in patients undergoing PCNL due to kidney stones.21,27
In a multicenter study by Tailly et al., 28 S.T.O.N.E., GSS, and CROES scoring systems were compared and they were reported to have similar rates in predicting stone-free status after PCNL. Furthermore, S.T.O.N.E. score was found to be an efficient instrument in predicting the operation time. 28
In this study, the S.T.O.N.E. nephrolithometry scoring system was found to be statistically significant in predicting stone-free status. When the patients were divided into three groups according to their S.T.O.N.E. nephrolithometry scores as low (5–6–7), medium (8–9–10), and high (11–12–13), a statistically significant difference was observed between the groups in terms of stone-free rates. Furthermore, a statistically significant increase was observed in the estimated blood loss, length of hospital stay, and operation time when the S.T.O.N.E. nephrolithometry scores increased. Okhunov et al. 8 found estimated blood loss, length of hospital stay, and operation time to be significant. Doulian et al. 29 applied S.T.O.N.E. nephrolithometry score to the pediatric age group and found that the estimated blood loss and length of hospital stay were insignificant.
In the study, the S.T.O.N.E. nephrolithometry score was also applied to patients in the pediatric age group. Aldaqadossi et al. 30 reported that STONE score was more valuable than other scoring systems in predicting stone-free status among pediatric patients undergoing PCNL, whereas it was found to be insignificant in predicting complications. The authors concluded that the scoring systems could be used in the pediatric age group, but further studies were needed to modify the several parameters of these scoring systems for use in children. 30
PCNL is also performed in patients with anatomical anomalies. Kocaaslan et al. 31 reported that the CROES score predicted the success of PCNL in cases with anatomical abnormalities, but that the S.T.O.N.E. score and GSS did not predict the success rate.
Anatomical variables, such as duplicated collecting system, horseshoe kidneys, and caliceal diverticulum, were not included in the scoring system due to the low incidence of these conditions and the inability to distinguish these differences in scoring in the development of S.T.O.N.E. score.
Although PCNL is a treatment alternative drawing attention with its high success rates, it should be kept in mind that various complications may develop during or after the procedure, and these complications may become life threatening.
The most common complications of PCNL are fever (21%–32.1%), bleeding requiring blood transfusion (11.2%–17.5%), and urine extravasation (7.2%). Septicemia (0.3%–4.7%), colon injury (0.2%–4.8%), and pleural injury (0%–3.1%) are rare major complications and overall major complication rate is reported to be 0.9%–4.7%. 32
Only 1 patient developed a major bleeding complication requiring intervention. A total of 13 patients were observed to develop complications: postoperative fever in 5 patients, bleeding requiring transfusion in 2 patients, need for a stent in 4 patients, prolonged leakage in 1 patient, and urinary retention in 1 patient. This study has shown that the likelihood of complications is statistically significantly greater as S.T.O.N.E. nephrolithotomy scores increase. Okhunov et al. 8 reported no significant correlation between the S.T.O.N.E. nephrolithotomy score and complications. The authors attributed this to the low complication rate and small sample size. 8
Kumsar et al. 33 reported that the S.T.O.N.E. score had a statistically significant correlation with Clavien's complication score (P < .001), operation time (P = .012), and stone-free status (P = .001).
Conclusions
The S.T.O.N.E. nephrolithometry score applied to predict stone-free status and complications in patients undergoing PCNL due to kidney stones will provide (1) a more objective and healthy preoperative counseling to the patient and (2) standardization in academic studies. Furthermore, this scoring system can be used as an objective criterion for predicting the complexity of the PCNL process.
Moreover, it will facilitate risk correction and enable physicians to better define the persistence of kidney stone and to identify patients who need to be referred to tertiary health institutions.
Footnotes
Authors' Contributions
Conception and design were carried out by E.D., M.E., E.C.P., A.O., M.B., and O.C. Acquisition of data was done by E.D., M.E., M.B., O.C., and F.A. Analysis and interpretation of data were by E.D., M.E., E.C.P., O.C., and A.O. Final approval of the completed article was given by E.D., M.B., E.D., E.C.P., O.C., and F.A.
Disclosure Statement
There is no conflict of interests between authors.
Funding Information
No research support or funding was received in connection with this study. The authors have no significant affiliation or involvement, either direct or indirect, with any organization or entity with a direct financial interest in the subject matter or materials discussed.