
Abstract
Background:
To explore the clinical efficacy of natural orifice specimen extraction surgery (NOSES) combined with transanal endoscopic operations (TEOs) to remove specimens from the anus for laparoscopic radical resection of colorectal cancer.
Methods:
From January 2014 to May 2020, 120 colorectal cancer patients were selected as study samples, including 60 cases who underwent NOSES laparoscopic radical resection of colorectal cancer (experimental group) and 60 cases who underwent traditional laparoscopic radical resection of colorectal cancer (control group). The basic preoperative conditions, operative time, intraoperative blood loss, lymph node dissection, postoperative hospitalization time, postoperative exhaust and defecation time, postoperative anal function, and postoperative complications were analyzed retrospectively.
Results:
Sleep quality score (6.26 ± 1.16), pain score (2.95 ± 0.79), and hospitalization time (11.55 ± 3.79 days) were better than those for the control group (P < .05). There were no positive cases of incisal margin in both groups. Gastrointestinal function recovery time, blood loss, lymph node dissection, and postoperative complications were not statistically significant (P > .05).
Conclusion:
NOSES combined with TEOs has the advantages of less trauma, quick postoperative recovery, and low psychological pressure, so it is worth popularizing.
Introduction
Colorectal cancer is one of the common malignant tumors. At present, surgical resection of tumor tissue and lymph node dissection are the standard radical methods. 1 Laparoscopic radical resection of colorectal cancer has become the mainstream surgical method in China. Compared with open surgery, it has the characteristics of less trauma and faster recovery. 2 During laparoscopic surgery, the specimen must be removed from the abdomen by an incision of ∼5 cm in length. Although it is smaller than abdominal incision in open surgery, complications such as incision infection and incisional hernia are inevitable. 3 For the purpose of beauty and reducing trauma, natural orifice specimen extraction surgery (NOSES) was born. With the development of NOSES in China, more and more surgeons are accepting this new technology, and the advantages of NOSES are increasingly found by many surgeons.4,5 Some studies have shown that NOSES has the advantages of shortening the movement and exhaust time after operation, increasing the slight comfort of postoperative pain, increasing the confidence of patients, improving the beauty of abdominal wall, and less abdominal wall dysfunction.6,7 TEO (transanal endoscopic operation) equipment can be used as a channel for specimen removal. Its advantage is that it can maintain pneumoperitoneum pressure during perineum operation and ensure laparoscopic operation. In addition, the metal sleeve can resist the extrusion pressure of the specimen to the lateral wall, thus protecting rectal mucosa and reducing anal sphincter injury.8–10
Materials and Methods
Patients
From 2014 to 2020, 120 patients with colorectal cancer who were admitted to the Department of Gastrointestinal Surgery of the Affiliated Hospital of Chengde Medical College were selected. Sixty patients underwent NOSE laparoscopic colorectal cancer radical surgery (experimental group), with an average age 61.05 ± 10.21 years old, average body mass index (BMI) 24.09 ± 3.19 kg/m2. All the patients in the experimental group had no abdominal specimen to remove the incision, and the specimen was removed through the TEO metal sleeve through the natural cavity anus. Sixty patients underwent traditional laparoscopic radical resection of colorectal cancer (control group), with an average age of 59.58 ± 10.63 years and an average BMI of 25.12 ± 3.92 kg/m2. All patients in the control group underwent 5 cm incision in the lower abdomen to remove the specimen. There were no cases of preventive stoma or conversion to laparotomy in both groups. Research data approved by IRB.
Inclusion and exclusion criteria
The inclusion criteria of the experimental group were as follows:
Preoperative colonoscopy was diagnosed as sigmoid colon cancer or rectal cancer. Laparoscopic tumor resection was performed without auxiliary incision on the abdominal wall, and the specimen was taken out from the anus.
The exclusion criteria of the experimental group were as follows:
Severe surgical taboos.
Distant metastasis.
Patients undergoing laparotomy due to other diseases.
Patients with low tumor location and unable to retain anus.
Patients with possible prophylactic stoma.
Inclusion criteria of control group:
Preoperative pathological report diagnosed as sigmoid colon cancer or rectal cancer.
Conventional laparoscopic tumor resection was performed, and 5 cm abdominal incision was performed.
Exclusion criteria of control group:
Severe surgical taboos.
Distant metastasis.
Patients undergoing laparotomy due to other diseases.
Patients undergoing Miles surgery.
Patients with possible prophylactic stoma.
Operation procedures
To establish laparoscopic operation and exploration: after general anesthesia is successful, modified lithotomy position and routine disinfection were undertaken, from umbilical transverse incision, ∼1 cm, long into 10 mm Trocar, to establish pneumoperitoneum and maintain pressure at 12 mmHg. The inferior abdominal artery is avoided and 5 mm Trocar is placed at the intersection of the external edge of the right rectus abdominis and the anterior superior iliac spine. 12 mm Trocar were placed at the Mcburney's point as the chief operation hole and 5 mm Trocar as the assistant operation hole at the anti-Mcburney's point. The lens is routinely probed through the umbilical cord into the abdomen.
Anatomy of the sigmoid colon: Pull the sigmoid colon up to make the sigmoid mesangial tense. Start the dissection at the root of the sigmoid colon, to the root of the Inferior mesenteric artery. Enter the Told's space level, dissect to the root of the inferior mesenteric artery, and continue dissecting the Told's space until reaching the Told's line of the sigmoid colon. Removal of lymph around the root of the inferior mesenteric artery and dissection of the inferior mesenteric artery. The adhesion zone is cut between the sigmoid colon and the left peritoneum, and the Told's line is extended on the outside of the sigmoid colon to the cephalic side to cut the outer peritoneum and reverse the sigmoid colon to the right side. Dissect medially within the Told's fascia gap and dissect to 5 cm below the tumor.
TME principle free rectum: According to the (TME) principle, the posterior aspect of the rectum was dissected along the anterior sacral space. The rectum was freed on both sides to the lateral peritoneal fold. The anterior rectal wall is freed and dissected along the gap between the prostate (or vagina) and the rectum to 5 cm of the lower edge of the tumor.
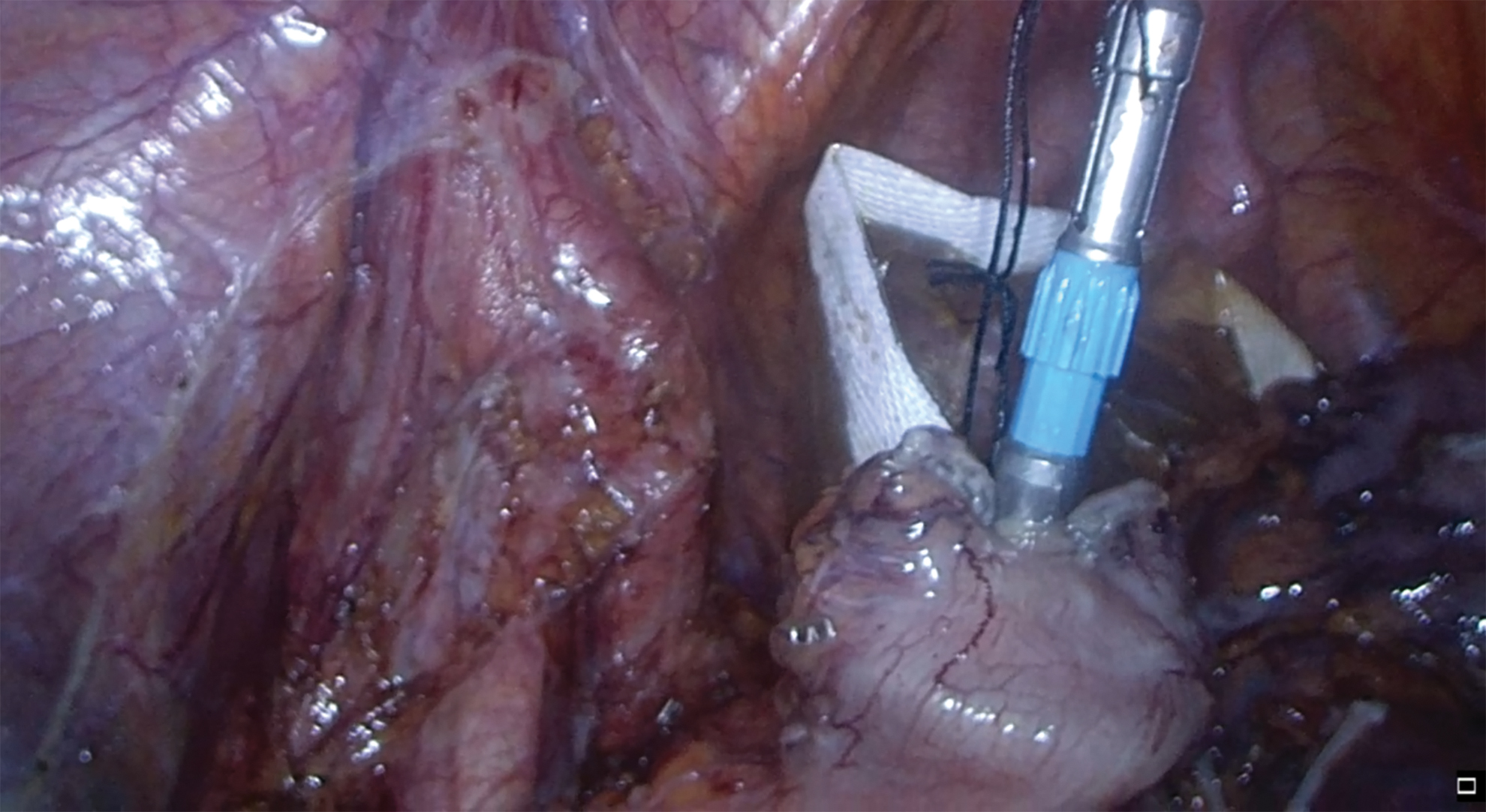
Tumor resection and specimen removal: The intestinal canal is cut 5 cm from the distal end of the tumor. A thin wire is tied to the stapler head. The stapler head is put into the plastic protective sleeve, and the plastic protective sleeve is inserted from the anus. The intestinal wall is cut 15 cm from the upper edge of the tumor. The head of the stapler is placed into the intestine. Leave the thread head outside the intestine, adjust the position, close the intestine with the closure, pull the hanging thread, and make the stapler head pierce through the intestine. The anus was placed in the TEO anorectal operation tube with anorectal device, the obturator was removed, and the tumor specimen was put into a plastic protective sleeve and pulled out of the body from the anus (Figs. 1–3).
Intestinal anastomosis: The distal rectal stump is closed, after fully covering the anus, the stapler body is inserted through the anus to complete the end-to-end anastomosis. After flushing the abdominal cavity, a pelvic drainage tube is routinely placed, and a rubber tube is placed at the anal canal.

The proximal bowel of the tumor is opened and the head of the stapler is completely inserted into the bowel. Color images are available online.

Adjust the thread position and cut off the proximal intestine of the tumor. Color images are available online.
The stapler head pierces the intestinal wall. Color images are available online.
Observation
Basic information of the patient: gender, age, BMI, distance, and size of the tumor from the anus are reported by colonoscopy before operation.
Surgery-related indicators: length of the operation time, the amount of blood loss during the operation, the time of the first postoperative exhaust and defecation, the time of the first postoperative meal, the number of intraoperative lymph node dissections, and the postoperative hospital stay and postoperative complications were statistically analyzed. The operation time is subject to the anesthesia record sheet. The method of collecting intraoperative blood loss is the total amount of aspirator collected during the operation minus the amount of abdominal irrigation fluid, and the number of intraoperative lymph node dissections is subject to the postoperative pathological results.
Anal function index: (postoperative anal function and satisfaction with Williams standard and Kirwan grade were evaluated).
Williams standard: A grade: good control of dry, dilute, and exhaust; B grade: good control of dry and dilute, exhaust cannot be self-controlled; C: good control of dry manure, rare manure occasionally poor control; D: dilute manure cannot be controlled; E: dry manure cannot be controlled. A, B, and C levels are functional; D and E levels are dysfunctional.
Kirwan grade: I grade: anal function is good; II grade: unable to control exhaust; III grade: accidental feces; IV grade: regular feces; V grade: anal incontinence.
Questionnaires: To observe the quality of sleep and pain after operation, Pittsburgh sleep quality index (PSQI) and visual analogue scale were used to observe. pain visual analogue score: using a swimming scale ∼10 cm long, 10 scales on one side, the two ends are “0” and “10,” 0 points for painless, 10 points represent the most unbearable pain, the higher the score, the more severe the pain. 11 The sleep quality score was 21, Grade 1 for every 5, four grades, A higher score indicates worse sleep. 12
Statistical analysis
SPSS 26.0 statistical software was used to analyze and process related data. Measured data are expressed as mean and standard deviation by t-test. The counting data were expressed as frequency by χ 2 test, P < .05 was considered statistically significant.
Result
Basic information of the patient
There was no significant difference between the two groups in gender, age, BMI, distance from the anus to the lower edge of the tumor, and the maximum diameter of the tumor (P > .05) (Table 1).
Basic Information
Surgery-related indicators
There was no statistically significant difference between the two groups of patients in terms of intraoperative blood loss, first defecation time after operation, first meal time after operation, and number of lymph node dissections (P > .05). The comparison of operation time and postoperative hospital stay between the two groups was statistically significant (P < .05). The operation time of the experimental group was longer than that of the control group, but the postoperative hospital stay of the experimental group was shorter than that of the control group. The difference between sleep score and pain index was statistically significant (P < .05). In terms of sleep quality and pain, the experimental group was better than the control group (Tables 2 and 3).
Surgery-Related Indicators
Sleep and Pain Score
Postoperative complications and anal function
We analyzed the clinical data of postoperative complications such as anastomotic leakage, intestinal obstruction, and incision infection. Among the 60 patients in the experimental group, there were 2 cases of anastomotic leakage, 1 case of incision infection, no postoperative intestinal obstruction, 60 cases of postoperative anal function were good (Williams criteria). According to the Kirwan classification, there were 57 cases of grades I and II. There were 2 cases of grade III, 1 case of grade III, 0 case of grade IV, and 0 case of grade V. Among the 60 patients in the control group, 4 had anastomotic leakage, 1 had intestinal obstruction, and 1 had incision infection. In the statistical results of complications, there was no statistical difference between the two groups (P > .05). The 60 patients in the control group had good postoperative anal function (Williams criteria). According to the Kirwan classification, 55 cases were grade I, 4 cases were grade II, 1 case was grade III, 0 case was grade IV, and 0 case was grade V (Tables 4 and 5).
Postoperative Complications
Anal Function
Discussion
According to global statistics, the incidence of colorectal cancer accounts for the third place among all tumor incidences.13,14 Surgical treatment is still the current mainstream treatment. With the development of society and technological progress, the development of surgical methods and instruments has become more and more diversified. Laparoscopic radical resection of colorectal cancer has incomparable advantages over traditional open surgery. 15 In recent years, with the continuous development of surgical technology, surgeons are increasingly pursuing “minimally invasive” surgery under the premise of ensuring the degree of radical surgery. NOSES is another “minimally invasive” label for colorectal tumor surgery. This operation avoids abdominal wall incisions, reduces the incidence of abdominal wall incision complications, while retaining the original functions of the abdominal wall, reduces postoperative abdominal scars, aesthetics, and reduces the psychological pressure of patients. 16 Studies have shown that the larger the abdominal surgical incision, the stronger the pain to the patient, and at the same time increase the patient's negative emotions, which is not conducive to the patient's postoperative recovery. 17
In this study, we innovatively used TEO surgical cannula to protect the anus, making specimen removal safer. According to Williams standard and Kirwan classification, the postoperative anal function and degree of satisfaction were evaluated. The results confirmed that the postoperative anal function was satisfactory. The pain score of the experimental group was 2.95 ± 0.79, and the average sleep quality score was 6.26 ± 1.16, which was significantly better than the control group. This shows that due to the reduction of abdominal incisions, less trauma, reduced postoperative pain, and improved sleep quality, it is beneficial for patients to get out of bed early, reduce their psychological burden, and promote rapid recovery of patients. 18 In addition, the difference in gastrointestinal function recovery time, intraoperative blood loss, intraoperative lymph node dissection, and postoperative complications was not statistically significant between the two groups (P > .05). The experimental group had no difference in the therapeutic effect of the control group. It shows that NOSES has the same tumor treatment effect as traditional laparoscopic surgery. There is no significant difference in the perioperative treatment effect. Under the same indications, laparoscopic NOSES can replace traditional laparoscopic surgery. The operation time of the experimental group (207.75 ± 65.56 minutes) was longer than that of traditional laparoscopic surgery (163.75 ± 46.46 minutes). The length of operation time mostly depends on the surgeon's mastery of surgical proficiency. The increase in the number of operations and the increase in proficiency of the surgeon with NOSES techniques can further shorten operation time. Postoperative hospital stay in the experimental group (11.55 ± 3.79 days) was significantly lower than that of the control group (15.90 ± 7.47 days). The difference in the length of hospital stay between the two groups once again proved that patients receiving NOSES recover faster after surgery and can be discharged earlier, reducing the economic burden of patients. In terms of postoperative complications, there were 2 cases of postoperative anastomotic leakage in the experimental group, 1 case of postoperative incisional infection, and 4 cases of postoperative anastomotic leakage in the control group, 1 case of intestinal obstruction, and 1 case of incisional infection. Postoperative complications in the two groups were not statistically significant. Case analysis of patients with postoperative complications found that preoperative coexisting diseases are high-risk factors, such as diabetes and hypertension; laparoscopic NOSES has no abdominal wall incision, which basically avoids abdominal wall incisional hernia. 19 During the surgical operation, the intra-abdominal opening of the intestinal canal and the delivery of the stapler head into the abdominal cavity via the anus are important factors in postoperative infection. 20 There are deficiencies in this study. This study did not conduct postoperative follow-up, but only studied the perioperative situation, and lacked data to evaluate the long-term efficacy of NOSES. For future studies, we will analyze the long-term survival curve of patients undergoing NOSES and compare them with patients undergoing traditional laparoscopy, and obtain more accurate and objective results.
Conclusion
Compared with traditional laparoscopic surgery, NOSES eliminates the abdominal incision, with only a few stuck holes, reducing the possibility of abdominal incision infection and incisional hernia, with light postoperative pain and rapid recovery, reducing the patient's psychological burden and shortening the hospital stay. It is worthy of further promotion.
Footnotes
Authors' Contributions
Conceptualization of the study was by Z.Z. and E.Z. Data curation was undertaken by Z.Z. and Q.C. Formal analysis was carried out by Z.Z., H.Z., and J.L. Methodology was done by Z.Z. and S.Z. Supervision was performed by E.Z. Writing—original draft—was by Z.Z. Writing—review and editing—was by Z.Z. and E.Z.
Acknowledgments
We thank all the staff in the department of gastrointestinal surgery, Affiliated Hospital of Chengde Medical University, for their contribution to our research.
Ethics Approval and Consent to Participate
Data were obtained from the medical records database of the Affiliated Hospital of Chengde Medical University, and the study was exempted by the database administrators.
Availability of Data and Materials
The data sets generated and/or analyzed during this study are available from the corresponding author on reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.