
Abstract
Background:
When the disposable arthroscopic banana knife (Linvatec, Largo, FL) became unavailable, many pediatric surgeons adapted the use of spatula tip cautery for laparoscopic pyloromyotomy; however, reusable arthroscopic knives remain readily available and are well suited to the procedure.
Methods:
We compared laparoscopic pyloromyotomy with a reusable arthroscopic banana knife (Sklar, West Chester, PA; catalog no. 45-6050) to those using spatula tip cautery at a single institution between September 1, 2012, and December 31, 2019. Mann–Whitney U test was used to compare operative time, room time, and time to discharge between groups.
Results:
Overall, 109 patients underwent pyloromyotomy for hypertrophic pyloric stenosis during the study time period. Of these, 12 were open and one was undertaken with the Storz pyloromyotomy knife, so these were excluded. A total of 74 (77.1%) laparoscopic cases with spatula tip cautery and 22 (22.9%) with the banana knife were included. Mean age at the time of surgery was ∼37 days. The majority of patients in each group were white, male, and full term. The most common comorbid conditions were reactive airway disease and neonatal abstinence syndrome. There were no significant differences in operative time (P = .61), room time (P = .41), or time from surgery to discharge (P = .26) between procedures using the banana knife and those using the cautery spatula tip. There were no perforations or recurrences.
Conclusion:
Our findings suggest that the reusable banana knife is a safe and effective alternative to spatula tip cautery for laparoscopic pyloromyotomy, with no difference in operative time, time from surgery to discharge, or complications.
Introduction
For infants with hypertrophic pyloric stenosis, operative intervention with a Ramstedt pyloromyotomy is the standard of care. This procedure was performed through an open approach until 1990, when the first known laparoscopic pyloromyotomy was performed. 1 Subsequently, several case series reported that a 3-port technique was safe and feasible,2,3 and provided superior cosmetic outcomes compared to an open approach.3,4 Additional small studies found that, although there was a learning curve associated with laparoscopy, perioperative outcomes were comparable or superior to an open surgery.5–7 However, due to concerns regarding the safety of laparoscopy in children, open pyloromyotomy remained the procedure of choice until other laparoscopic procedures became more widely accepted in the pediatric population.8–10
In 2006, the first large prospective trial comparing open and laparoscopic pyloromyotomy was published. 11 They found no difference in operative time or length of recovery between procedures, but a laparoscopic approach resulted in less postoperative pain, fewer episodes of postoperative emesis, and fewer complications. Subsequent studies have published concordant findings,12–15 resulting in the widespread adoption of a laparoscopic approach as the new standard of care for infants with hypertrophic pyloric stenosis. 15 Some concerns remain, however, for slightly higher rates of mucosal injury and incomplete pyloromyotomy with a laparoscopic approach, particularly during the initial learning period.13–16
Before 2010, many pediatric surgeons performed laparoscopic pyloromyotomy with the use of a disposable arthroscopic banana knife (ConMed; Linvatec, Largo, FL); however, when this instrument became unavailable in 2010, many surgeons adapted the use of spatula tip and hook cautery for this indication, with similar operative time, time to first full feed, length of stay, readmission rates, and postoperative complication rates.17,18
Although the disposable banana knife is no longer available, reusable arthroscopic knives remain readily available and are well suited to the procedure. For instance, the reusable arthroscopic banana knife (Sklar, West Chester, PA; catalog no. 45-6050) is ∼23.5 cm long and 3 mm in diameter (Fig. 1). It has a curve in the blade centered 3 mm from the tip of the knife and itself is curved and sharp on both sides; however, as a reusable knife, it is slightly dull and thus provides excellent tactile sensation for the operating surgeon. In comparison, the unprotected portion of the spatula tip cautery is ∼4 mm in length. The purpose of this study was to compare laparoscopic pyloromyotomy procedures using the reusable arthroscopic banana knife to those using the spatula tip cautery.

Views of the reusable arthroscopic banana knife. Views of the reusable arthroscopic banana knife.
Materials and Methods
All patients who underwent pyloromyotomy by one of seven pediatric surgeons at a single, academic medical center between September 1, 2012, and December 31, 2019, were eligible for inclusion. Patients were identified by current procedural terminology (CPT) code for pyloromyotomy (CPT codes 43520 and 43659). Individuals were only included in the final cohort if they underwent laparoscopic pyloromyotomy with either the spatula tip cautery or the banana knife. In addition, patients were excluded from the final cohort if the indication for surgery was not hypertrophic pyloric stenosis. Among patients who underwent a laparoscopic pyloromyotomy, our exposure of interest was the instrument used to create the pyloromyotomy, which could be the spatula tip cautery or the banana knife. Instruments were identified based on the description in the operative report.
The reusable arthroscopic banana knife was utilized exclusively by a single surgeon at our institution, while the remaining five surgeons employed the cautery spatula tip. Our primary outcomes of interest were median operative time, median operating room time, and median time to discharge. Operative time was defined as the time from initial incision until closure of all operative sites. Room time was defined as the time from entry into the operating room until transport to the recovery room. Time to discharge was defined as the time from leaving the operating room until discharge from the hospital. This project was reviewed by the Baystate Medical Center Institutional Review Board (IRB) and determined to meet the definition of non-human subjects research; thus, the project was exempt from full IRB review.
Statistical analysis
We initially evaluated baseline patient characteristics overall and between the different laparoscopic instruments. Results for continuous variables are shown as mean and standard deviation or median and interquartile range, while categorical variables are shown as frequencies and percentages. Mann–Whitney U test was used to compare operative time, room time, and time to discharge between groups. Statistical significance was set at a two-sided alpha of 0.05. Statistical analysis was carried out with R Studio. 19
Results
A total of 109 patients underwent pyloromyotomy for hypertrophic pyloric stenosis during the study time period. Twelve of these were performed through an open approach by a single surgeon who does not perform laparoscopic pyloromyotomy procedures and one with the Storz pyloromyotomy knife, so these were excluded from the study population. Of the remaining 96 patients, 74 underwent laparoscopic pyloromyotomy with the cautery spatula tip (77.1%) and 22 with the banana knife (22.9%).
Baseline characteristics between the spatula tip cautery and banana knife groups are summarized in Table 1. In both cases, mean age at the time of surgery was ∼36 days and the majority of patients were white, male, and full term. The most common comorbid conditions were reactive airway disease in the spatula tip cautery group (n = 4, 5.4%) and neonatal abstinence syndrome in the banana knife group (n = 5, 22.7%). There were no significant differences in baseline patient characteristics between groups. All procedures using the spatula tip cautery and those using the banana knife were performed using a similar technique with one port and two stab incisions. A side-by-side comparison of the main steps in these procedures can be found in Figure 2.
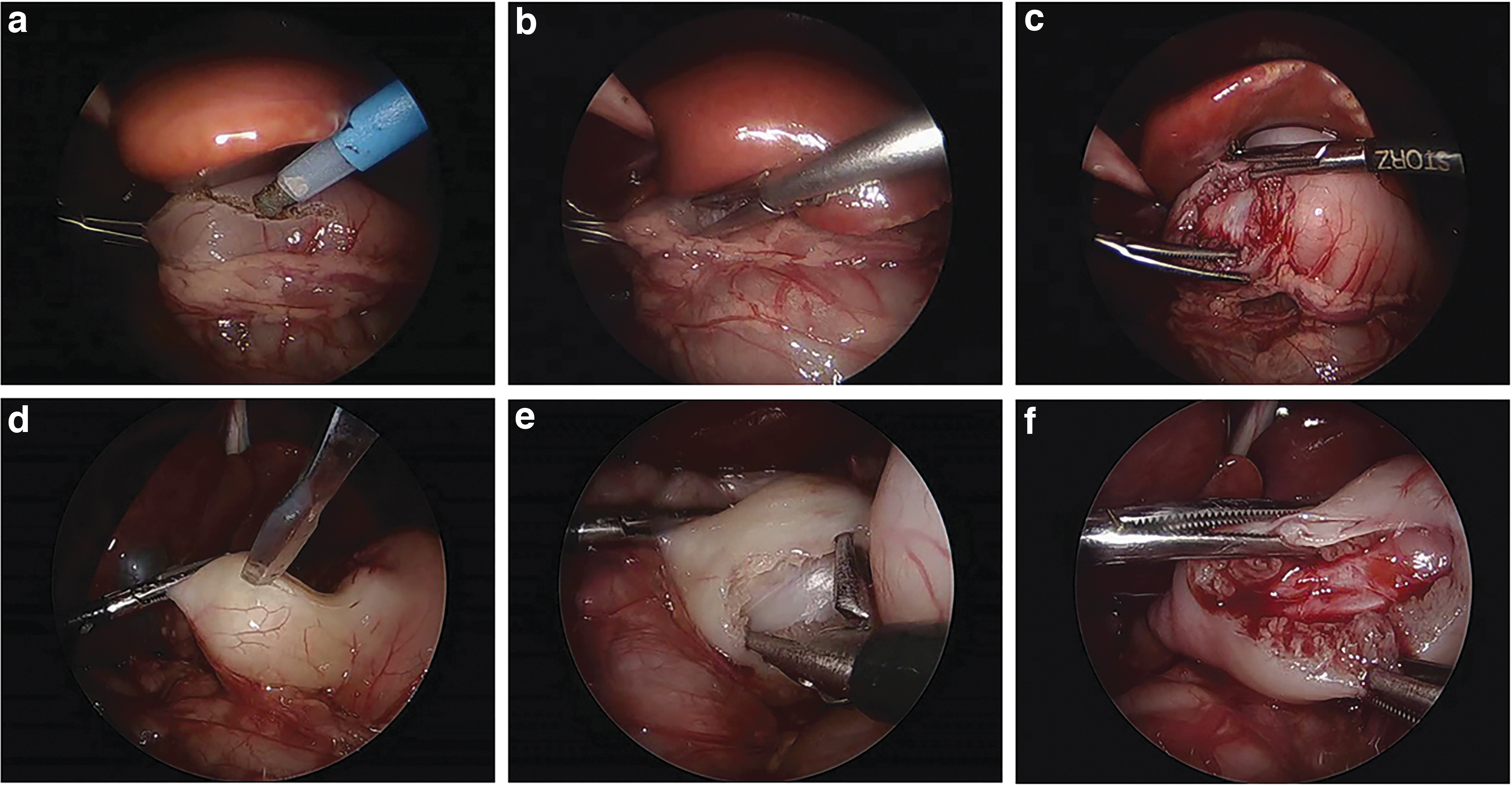
A side-by-side comparison of laparoscopic pyloromyotomy procedures using the cautery spatula tip and the reusable arthroscopic banana knife. A side-by-side comparison of laparoscopic pyloromyotomy procedures using the cautery spatula tip
Baseline Patient Characteristics for Laparoscopic Pyloromyotomy Procedures Using the Spatula Tip Cautery and the Banana Knife
SD, standard deviation.
Postoperatively, all patients were fed ad lib and discharged once tolerating feeds at goal. When comparing outcomes between groups, there was no difference in median operative time (P = .61) or median room time (P = .26) between groups (Table 2). Postoperatively, median time to discharge was not significantly different between groups (P = .41). All patients had complete resolution of their preoperative symptoms, no revisions were necessary, and there were no perforations.
Comparison of Median Operative Time, Room Time, and Time to Discharge Between Procedures Using the Cautery Spatula Tip and the Banana Knife
IQR, interquartile range.
Discussion
In this retrospective cohort study of 96 patients with hypertrophic pyloric stenosis, who underwent laparoscopic pyloromyotomy with either the spatula tip cautery or the reusable arthroscopic banana knife, we found no difference in safety, operative time, room time, or time to discharge between instruments.
Pyloromyotomy is the standard of care for the treatment of hypertrophic pyloric stenosis. Over the past two decades, evidence has emerged that laparoscopy is a safe and effective approach for the management of hypertrophic pyloric stenosis. For instance, several studies have shown that, although there was initially an institutional learning curve associated with the adoption of a laparoscopic approach, there is no difference in the incidence of mucosal injury, incomplete pyloromyotomy, or postoperative complications compared to an open approach.11–13 In addition, a laparoscopic approach may shorten operative time, decrease recovery time, reduce hospital length of stay, and provide superior cosmetic outcomes without any increase in complication or readmission rates.14,15,20 For this reason, laparoscopic pyloromyotomy has become increasingly accepted among pediatric surgeons. 15
Originally, laparoscopic pyloromyotomy was performed with the use of a disposable arthrotomy or retractable knife; however, the disposable arthrotomy knife became unavailable in 2010, so surgeons have since adapted the use of spatula tip cautery and hook cautery, with good effect.17,18 For instance, Jain et al. compared procedure characteristics and postoperative outcomes between 12 laparoscopic pyloromyotomy procedures with a pyloromyotomy knife to 15 procedures using the hook cautery. 17 They found no difference in operative time, time to full feeds, and hospital length of stay between groups and there were no postoperative complications in either group. Similarly, Thomas et al. compared 191 laparoscopic pyloromyotomy procedures using the arthrotomy knife to 190 procedures using the blunt tip cautery and found no difference in operative time, hospital length of stay, or the need for readmission between operative techniques. 18 Although these reports did not employ a reusable arthrotomy knife, they do lend credence to our findings that similar perioperative outcomes can be achieved when using the arthrotomy knife compared to the spatula tip or hook cautery.
In this study, we chose to repurpose the reusable arthroscopic banana knife for the purpose of laparoscopic pyloromyotomy; however, other knives have also been employed with good outcomes. For instance, Anwar et al. in United Kingdom proposed a two-port trocar system using an ophthalmic knife, 21 while Abu-Kishk et al. in Israel adapted the use of a myringotomy knife. 22 As in our study, these authors found that the mean operative time was ∼23 minutes and patients were discharged after 24–48 hours. Other novel approaches have also been proposed, such as a peroral endoscopic approach, which has the added benefit of being incision free. 23 Peroral endoscopic myotomy was originally proposed as a less invasive treatment of achalasia in adults, 24 but could theoretically revolutionize the treatment of hypertrophic pyloric stenosis in infants. The success of these other approaches suggests that other knives and surgical approaches may be safe and effective for the performance of laparoscopic pyloromyotomy in the treatment of hypertrophic pyloric stenosis.
Although our findings were similar to the results of other studies using the spatula tip and hook cautery, subjectively, our surgeon reported that the tactile sensation provided by the arthrotomy knife was helpful in perceiving the myotomy incision. In addition, the curve of the banana knife is 3 mm from the tip and thus serves as a good frame of reference for the depth of the myotomy. The angle of the curve also provides a good angle of approach for the myotomy, thereby minimizing the need to roll the pylorus and potentially helping to prevent onion peeling of the pylorus.
Conclusion
Our findings suggest that the reusable arthrotomy banana knife is a safe and effective alternative to spatula tip cautery for laparoscopic pyloromyotomy, with no difference in operative time, time from surgery to discharge, or complications.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.