
Abstract
Introduction:
Undescended testis is a relatively common congenital anomaly in male children with a prevalence of 1%–2% in live births. Upon discovering an empty scrotum, it is important to determine whether the testis is palpable, ectopic, retractile, or nonpalpable. A canalicular or “emergent” testis is a peeping one that freely slides to and fro between the abdominal cavity and inguinal canal. It may be impalpable initially, but at a time, it emerges from the internal ring to be palpable when it is “milked” down (where it was concealed from detection). It is reported that 15%–40% of cryptorchidism are viable peeping/canalicular testis. The laparoscopic approach for treating intracanalicular undescended testes offers many advantages over open inguinal orchiopexy. It maintains the integrity of the inguinal canal and eliminates the need to divide the epigastric vessels during dissection. The ability to dissect the testicular vessels at a higher level would increase the vessel length available to bring the testis down to the scrotum without strain. The aim of this study is to present our experience and evaluate laparoscopic approach for management of intracanalicular testes regarding operative safety, efficacy, and postoperative outcomes.
Patients and Methods:
This is a prospective study conducted at Department of Pediatric Surgery, MCH Hospital, Bisha, Saudi Arabia and Pediatric Surgery Department, Al-Azhar University Hospitals, Cairo, Egypt, in the period from October 2018 to August 2020 to evaluate the safety and efficacy of laparoscopic orchiopexy for intracanalicular testis. Patients with retractile testes, ectopic testes, testes located distal to the external inguinal ring, and nonpalpable testes were excluded from the study.
Results:
The study was conducted on 62 male children with 70 intracanalicular (peeping) testes, with age range from 8 months to 48 months (mean age: 24 months). Among them, 26 cases (∼42%) were left-sided, 28 (∼45%) were right-sided, and 8 (∼13%) cases were affected bilaterally. Postoperatively, all testes maintained good size without postoperative hydrocele or inguinal hernia. One case (1.4%) required open redo-orchiopexy because of testicular re-ascent to the level of scrotal neck. Moreover, there was no evidence of testicular atrophy confirmed by postoperative ultrasonography. All patients had good satisfied cosmetic results obtained by parent's questionnaire at postoperative follow-up visits.
Conclusion:
Laparoscopic orchiopexy for management of (intracanalicular) undescended testes is safe, effective, less invasive, without disturbance of inguinal canal anatomy, and with better cosmetic results.
Introduction
Undescended testis (UDT) is a relatively common finding in pediatrics with prevalence about 1%–2% in newborns. Upon discovering an empty scrotum, it is important to determine whether the testis is palpable, ectopic, retractile, or nonpalpable. 1
A canalicular or “emergent” testis may be initially impalpable and may appear at a time when it emerges beyond the internal ring to settle inside the inguinal canal. It is estimated that 15%–40% of cryptorchidisms are viable peeping/intracanalicular.1,2 For this group of cryptorchidism, the question as to whether performing laparoscopic orchiopexy would have been beneficial is still controversial. 3
Open inguinal exploration for the intracanalicular UDT is not only unlikely to be successful but also associated with many obstacles in most cases treated with this procedure, which involves extensive blind retroperitoneal dissection of the spermatic cord. Moreover, this procedure is associated with many complications, such as injury of testicular vessels resulting in testicular atrophy or recurrent cryptorchidism.4–5
More proximal dissection of vas and vessels is required for complete safe mobilization of spermatic cord. This is too much difficult and hazardous by open approach, but is facilitated and very easy by laparoscopy. The laparoscopic approach for treating canalicular undescended testes offers many advantages over open inguinal orchiopexy. Most importantly, it maintains the integrity of the inguinal canal anatomy and eliminates the need to divide the epigastric vessels during dissection. The ability to dissect the testicular vessels at a higher proximal level, up to lower pole of the kidney, and to dissect the vas near the urinary bladder, would increase the cord length, available to pull the testis down without tension. 5
Laparoscopic orchiopexy also provides power of magnification, which enables careful dissection, so as not to injure the vas deferens or testicular vessels. At the same time, the contralateral processus vaginalis can be transected when it is patent.5,6 The aim of this study is to present our experience and to evaluate the laparoscopic procedure for management of intracanalicular testis regarding operative safety, efficacy, and postoperative outcomes.
Patients and Methods
This is a prospective study conducted at Department of Pediatric Surgery, MCH Hospital, Bisha, Saudi Arabia and Pediatric Surgery Department, Al-Azhar University Hospitals, Cairo, Egypt, from October 2018 to August 2020, to evaluate the safety and efficacy of laparoscopic orchiopexy for intracanalicular testis. The study was approved by the Institutional Review Board and ethics committee (registration number: H5D2-2019-0041E) and also registered at ClinicalTrials.gov (ID: NCT04821167). Written informed consents were obtained preoperatively from guardians of all patients.
A total of 304 UDT cases were examined in the outpatient clinic by 2 senior surgeons independently at two different times to verify thus justify the diagnosis of peeping testis for enrolment in the study. Of them, 62 cases with peeping (intracanalicular) testes were included in the study. Proper examination was done for patients using squatting and frog leg position with gentle palpation of the testis, aided by preoperative inguinoscrotal Doppler ultrasonography with estimation of testicular volume and vascularity using 7.5 mHz transducer to assess position, volume (length × width × height × 0.52), echopattern, echotexture, and flow phase of the testicular vessels. Patients were re-examined under anesthesia (while muscles were relaxed) to confirm the diagnosis and proceed with laparoscopy.
Patients with a retractile testis, ectopic testis, palpable testis (located distal to the external ring), and nonpalpable testis (NPT) were excluded from the study.
Sixty-two patients with 70 intracanalicular (peeping) testes met the inclusion criteria and were submitted to laparoscopic retroperitoneal dissection of peritoneal bands anchoring the spermatic cord, skeletonization of testicular vessels, and vas to achieve adequate length for pull-down and tension-free scrotal testicular fixation.
Patients were followed up at the outpatient clinic by frequent visits (1 week, 3, 6, and 18 months postoperatively).
Evaluation parameters included operative difficulties, intraoperative complications, operative time, and early postoperative complications.
Final testicular position was assessed by another (independent) surgeon. Size and vascularity were evaluated by Doppler ultrasonography at 6th month postoperatively.
Operative technique
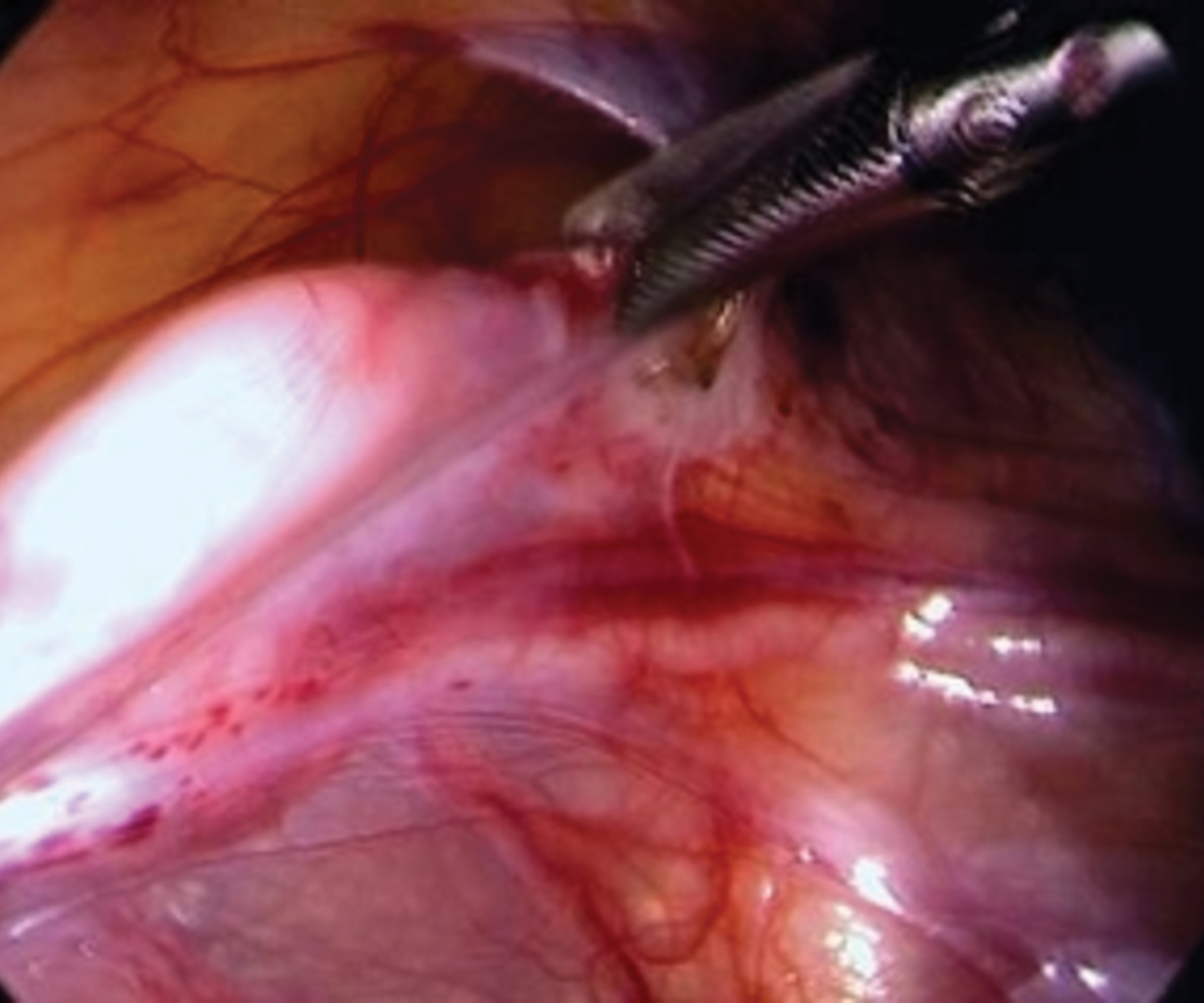
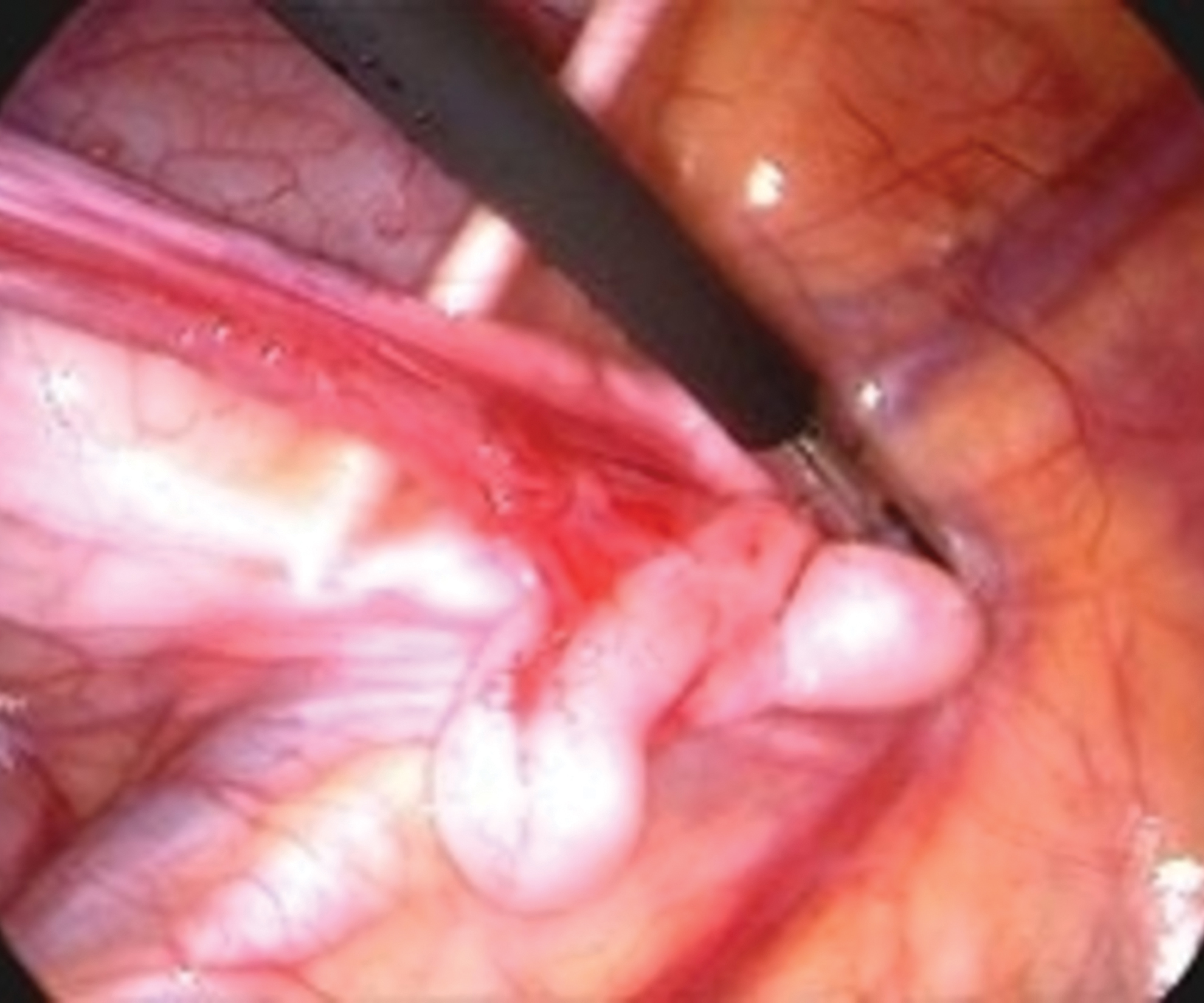
Patients were positioned supine under general anesthesia with full muscle relaxation. Sterilization and draping were done in a standard manner, then a urethral catheter was inserted. The surgeon stood at the patient's head, with the assistant at the left and the scrub nurse at the right side of the patient. A monitor was placed at the lower end of the table. A 5-mm umbilical port was inserted by open Hasson's technique and 3-mm trocars were placed bilaterally in the midclavicular line slightly below the level of umbilicus. The abdominal cavity was insufflated by CO2 to a pressure of 8–10 mmHg. A laparoscope was introduced for inspection of the internal inguinal ring (IIR) area. The peritoneum of the internal ring was incised to disconnect the patent processus vaginalis lateral to the spermatic vessels and medial to the vas deferens (Fig. 1), so the vas deferens and testicular vessels become visible. Next, the testis was pulled into the abdominal cavity. The anterior tunica vaginalis was incised distally, and the gubernaculum was identified, grasped, and divided after determining the distal extent of the vas deferens (Fig. 2). Retroperitoneal dissection was done with excision of all bands and creation of well-vascularized peritoneal flap bounded by testicular vessels laterally and vas deferens medially, with lateral peritoneal flap incised up to the lower pole of the kidney.

Identification of the testis and medial incision of the inguinal ring peritoneum. Color images are available online.
Incision of gubernaculum with great care of looped vas. Color images are available online.
The testis was pulled to the contralateral IIR without tension as a test of sufficient length (Fig. 3). A midscrotal incision was made and a subdartos pouch was created; then a grasping forceps was advanced into the abdominal cavity through scrotal incision medial to the inferior epigastric vessels. Then, the testis was pulled down under vision to avoid any iatrogenic torsion. If more length was required, the peritoneal flap was incised at the anterior surface of the spermatic vessels, extending proximally, the distal triangle of the peritoneal flap between the vessels and the vas deferens was spared to augment the collateral circulation (Fig. 4A, B), and finally the testis was freely fixed at the bottom of the scrotum within the subdartos pouch.
Mobilized testis pulled to the contralateral IIR freely without tension. IIR, internal inguinal ring. Color images are available online.

Results
Of total 304 UDT cases examined in the outpatient clinic of two pediatric surgery centers, 62 cases with peeping (intracanalicular) testes were included in the study. Whereas 47 cases with retractile testes, 22 cases with ectopic testes, 119 cases with palpable testes located distal to the external ring, and 54 cases with nonpalpable (intra-abdominal) testes were excluded from the study.
The study involved 62 patients with 70 intracanalicular undescended testes, with their age range from 8 to 48 months (Mean age 24 months). Among them, 26 cases (∼42%) were left-sided, 28 cases (∼45%) were right-sided, and 8 cases (∼13%) were bilateral as shown in Table 1.
Patient Characteristics with Intracanalicular Testis
Mean operative time was 24 minutes (range 20–41 minutes) for unilateral cases and 43 minutes (range 36–58 minutes) for bilateral cases. None of the cases required conversion to open orchiopexy, and all patients had successful orchiopexy in the scrotal subdartos pouch.
Postoperative oral antibiotics (amoxicillin 20 mg/kg) and analgesics (paracetamol 15 mg/kg) were given, and oral feeding started 6 hours postoperatively. All patients were discharged after a mean hospital stay of 24 hours and resumed normal activities after one more day.
During subsequent follow-up, which ranged from 10 to 18 months, all testes maintained good size and adequate position without postoperative hydrocele or inguinal hernia. One case (1.4%) needed open redo-orchiopexy because of testicular ascent at level of scrotal neck. Moreover, there was no evidence of testicular atrophy confirmed by postoperative ultrasonography. Testicular volume was estimated by ultrasound using the formula (length × width × height × 0.52). The difference between pre and postoperative testicular volume was statistically insignificant, P value >.05 as shown in Table 2. No patient developed wound infection or hematoma. All patients had very satisfied cosmetic results obtained by parents’ questionnaire at postoperative visits.
Difference Between Pre- and Postoperative Testicular Volume Was Statistically Insignificant (P Value > .05)
cc, cubic centimeters; SD, standard deviation.
Statistical analysis
Data will be presented as mean, standard deviation, range, and average for quantitative data and number and percentage, using chi-square test (X 2 ) for qualitative data. The significance level was set at P value <.05. Statistical analysis was performed using statistical package for social sciences (SPSS) version 23.0 (IBM Corp, IBM SPSS Statistics for Windows, Armonk, NY).
Discussion
UDT jeopardizes the reproductive potential, predisposes to torsion, causes the parents’ anxiety, and increases the risk of testicular tumor. 7 Laparoscopy used for the diagnosis and treatment of nonpalpable intra-abdominal cryptorchidism has been universally accepted in clinical practice, whereas the inguinal palpable cryptorchidism is treated by traditional open inguinal orchiopexy. 8
A canalicular or emergent testis represents a challenging variant. A variety of clinical examination techniques and radiological imaging modalities have been used to palpate/visualize the canalicular testis. 9 Ultrasonography is a useful tool in identifying the intracanalicular testis and is also effective in documenting the testicular size and volume.10,11 In this study, we utilized ultrasonography for measurement of testicular volume pre- and postoperatively.
Open surgery for intracanalicular testis requires dissection of the inguinal canal, which, in older children, needs to dissect the internal oblique and transversus abdominis muscles till the internal ring for a higher level, to release the peritoneum from the vas and vessels and perform herniotomy at the proper neck of the sac, which is liable to cause wound infection, bleeding, incisional hernia, and even testicular retraction or malposition. According to the literature, the wound infection rate after open inguinal orchiopexy is 1.9%–2.5% and testicular atrophy occurred in about 3.7%–5% of low inguinal cryptorchidism, whereas in high inguinal cryptorchidism it reached up to 9%.6,8,12
Although laparoscopy has a great role in the diagnosis and treatment of NPT, its role in the management of canalicular or peeping testis is not well established. 9
In 1995, Docimo et al. first introduced laparoscopic orchiopexy for management of cryptorchidism located high in the inguinal canal. 4 Subsequently, He et al. have submitted 103 patients with canalicular undescended testes for laparoscopic orchiopexy and followed up them for a period range from 6 to 12 months. Testes maintained good size and a correct position without recurrent hydrocele, inguinal hernia, or testicular atrophy. In this study, we have longer follow-up period and similar results except of 1 patient of testicular ascent at level of scrotal neck that required redo open orchiopexy. 5 In this study, we agreed with He et al. that laparoscopy is feasible, safe, and effective in management of canalicular testes.
Elderwy et al. supported the results of this study, as they compared between two groups of cases of intracanalicular peeping testes, randomized to be managed by laparoscopic orchiopexy in one group (n = 21) and open orchiopexy in the other group (n = 25), and they reported that laparoscopic orchiopexy is a successful eventless approach for peeping testis, with no redo orchiopexy. Whereas 2 cases in the open group required redo orchiopexy. They have longer follow-up period (1–5.5 years) with insignificant difference of testicular volume between the two groups. 13
Mean operative time of laparoscopic orchiopexy with Riquelme et al. and He et al. was 50 and 32.7 minutes, respectively.5,14 In this study, we spent shorter mean operative time (24 minutes). This may be due to worldwide rise of the learning curve and progressive improvement of laparoscopic skills.
In this study, we agreed with Riquelme et al. and He et al., as we found laparoscopic orchiopexy for high inguinal (canalicular) testis has high success rate, low incidence of testicular re-ascent, and no testicular atrophy.5,14 We also found that no need to close the peritoneal defect after patent processes vaginalis dissection, because transection of the processus vaginalis was sufficient, without any postoperative increased risk of inguinal hernia or hydrocele. This is well supported by other authors such as Khairi et al. and Ceccanti et al.15,16
Laparoscopic technology has obvious advantages: above all, the magnification power that gives a large and clear surgical field view, so it is easier to loosen and separate the retroperitoneal spermatic vessels under excellent visualization. The testis is fixed in the scrotum without tension, which can effectively reduce the occurrence of testicular atrophy and retraction, in addition to maintaining the anatomical integrity of the inguinal canal. Compared with the traditional open surgical methods, the postoperative pain is less, and the recovery is faster, no obvious surgical scars, and the parents declared better satisfaction by the excellent cosmetic results. Also, laparoscopic surgery can simultaneously detect and manage a contralateral occult hernia. Studies have shown that >10% of asymptomatic hernia accidentally found by laparoscopy will develop into symptomatic metachronous inguinal hernia, eventually requiring repair.5,13,17,18
Limitations of the study include that it is nonrandomized, relatively small sample size, and short follow-up period. Further randomized controlled studies, conducted on a large scale of patients and longer follow-up time, are required to support these findings and draw more meaningful generalizable conclusions.
Conclusion
Laparoscopic orchiopexy for management of high inguinal (canalicular/peeping) UDT is safe, effective, less invasive, and has better cosmetic results.
Patient Consent
Written informed consents were obtained from all parents. The consents were approved by our Hospital's Ethics Committee.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.