
Abstract
Although once thought to be a point of contention, the use of minimally invasive surgery for the hemodynamically stable pediatric trauma patients has grown dramatically since its conception in the 1970s and becoming a widely acceptable option for select patient populations. An accumulation of literature over the decades has continued to support laparoscopy for both diagnostic and therapeutic purposes in the pediatric trauma patients as laparoscopy is likely to decrease morbidity, hospital cost, and negative laparotomy rates. In this review, we describe what we believe to be the critical aspects of diagnostic laparoscopy in the setting of pediatric trauma.
Introduction
In the United States, the most common cause of death in the pediatric population (1–19 years of age) remains to be trauma. 1 Traditionally, laparotomy was the means by which providers achieved both diagnosis and therapy, but with the increase in popularity of minimally invasive surgery (MIS), laparoscopy has become a procedure of choice especially when faced with the clinical challenge of the hemodynamically stable pediatric trauma patients. 2
Since the 1970s, MIS has evolved in capability and efficiency with previous studies supporting its role in pediatric trauma to decrease postoperative morbidity, length of stay, and hospital cost. 3 Perhaps one of the strongest arguments for laparoscopy over laparotomy is the current body of literature to suggest that MIS can greatly reduce an institution's negative laparotomy rate as unnecessary laparotomy can be associated with increased postoperative morbidity. 4
In this study, we describe our approach to the diagnostic laparoscopy for pediatric abdominal trauma as well as recommendations on how to proceed based on various injuries that are identified.
Patient Selection
Appropriate patient selection is paramount in determining whether or not to proceed with an MIS approach in the setting of pediatric trauma. Hemodynamic instability or obvious signs of peritonitis should preclude patients from laparoscopy and the cause of instability should be further investigated before considering MIS for trauma. 2 As such, we do not consider laparoscopy as a replacement for laparotomy but rather two different treatments for two different patient presentations.
In pediatric trauma, the appropriate treatment for most solid organ injuries is often times nonoperative. Therefore, those patients who proceed with open surgery are either unstable or the provider has identified a large amount of hemoperitoneum that necessitates exploratory laparotomy. Furthermore, conversion to laparotomy should be considered if the surgeon is packing all four quadrants as packing is not typically recommended during laparoscopy for trauma.
Positioning
We recommend placement of ports in a diamond-shaped configuration with the umbilicus acting as the top of the diamond. Initially, 5 mm ports can be placed at the umbilicus, suprapubic region, right lower quadrant, and left lower quadrant (Fig. 1). If a laparoscopic stapler is needed, one of these 5 mm ports can be converted to a 12 mm port depending on the injury that is identified. If the mechanism of injury or the patient presentation is concerning for a high probability of conversion to open surgery, consider prepping the patient in a larger area. For example, some surgeons recommend prepping from the chin to the bilateral knees in the scenario in which harvest of a vein graft or clamping of the aorta becomes necessary. To reiterate, this is highly unlikely in the stable patient, but depending on the patient presentation, it is still a reasonable consideration. As with all most laparoscopy procedures, we recommend induction of general anesthesia, placement of an endotracheal tube, the patient in supine positioning, and both arms tucked. The surgeon and camera operator should stand on the same side of the patient to maintain the same perspective and to avoid operating in parallax.
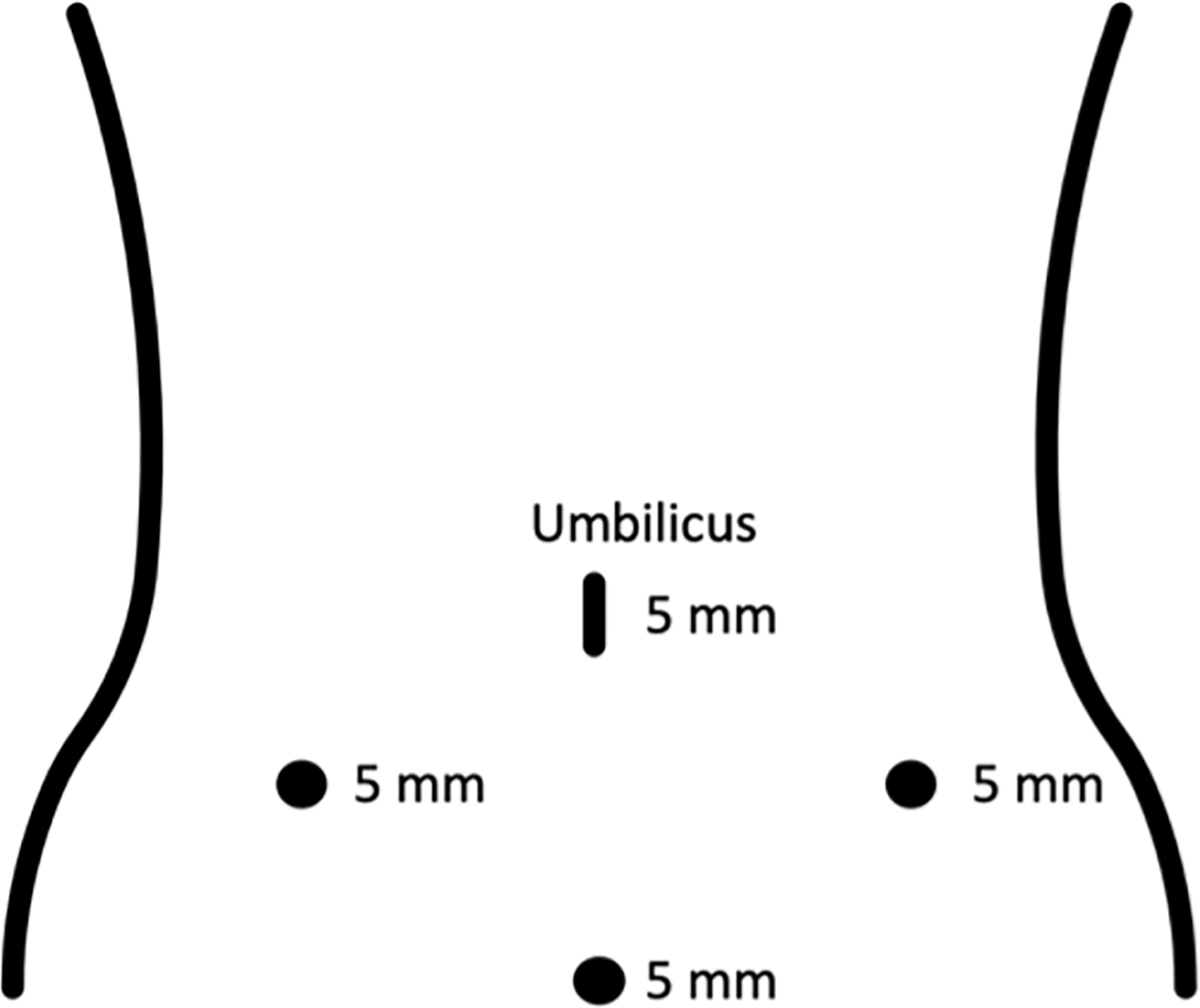
“Diamond-shaped” port placement for diagnostic laparoscopy in trauma.
Technique
Step 1
Access the peritoneum through the umbilicus per surgeon preference (either Hasson or Veress needle). Once access is confirmed, proceed with port placement as already described with the diamond-shaped arrangement.
Step 2
With both surgeon and camera operator standing on the patient's left, proceed with general inspection of the abdomen noting the color and character of peritoneal fluid and whether it is blood, bile, or stool. For penetrating abdominal injuries specifically, failure to identify any rent in the peritoneum may rule out intra-abdominal injury. Run the bowel from ileocecal valve to the ligament of Treitz, making sure to evaluate both sides of the bowel and mesentery for injury. We recommend repair of injuries to the small bowel and mesentery promptly upon recognition to avoid both forgetting to repair the injury and losing the location of the injury in the event that there are multiple intestinal injuries present. We typically repair bowel injuries with interrupted Vicryl suture. If intracorporeal repair proves difficult, we recommend extracorporealizing the bowel to most adequately treat the injury.
Step 3
Attention is then turned to the stomach. Evaluate the anterior surface of the stomach for injury before opening the gastrocolic ligament to obtain access to the lesser sac. Inspect the posterior aspect of the stomach for injury. Then evaluate for any evidence of bleeding, bruising, or free fluid to suggest pancreatic or duodenal injury.
Step 4
If concern for duodenal injury, Kocherize the duodenum to evaluate the second portion of the duodenum for injury. Evaluate the liver and gallbladder for evidence of injury. If small incidental liver lacerations are identified, direct application of thrombogenic agents and pressure can be applied. But if hemostasis is not achieved or the hepatic injury is too extensive, we recommend converting to laparotomy. While in the right upper quadrant (RUQ), take time to also inspect the right hemidiaphragm.
Step 5
Inspect the right colon to the mid transverse colon. If there is suspicion of retroperitoneal injury, you must mobilize the colon to evaluate both sides. The surgeon and camera operator should then move to the right side of the patient to better inspect the splenic flexure and left side of the colon and rectum.
Step 6
Evaluate the spleen and the tail of the pancreas. While inspecting the spleen, take time to also inspect the left hemidiaphragm. If bleeding is identified on the spleen—we typically treat solid organ injuries similarly with the application of cautery, argon beam, or attempt application of thrombogenic agents as previously stated with hepatic injuries. If hemostasis is not achieved with laparoscopy, consider conversion to laparotomy.
Step 7
Lastly, evaluate the pelvis. If there is injury to the pelvic sidewalls and you do not have preoperative imaging of the pelvis, you should proceed with on-table intravenous pyelogram to evaluate extent of possible injury to the urinary system.
Postoperative care
Postoperative care varies based on extent of the injury and necessary interventions. If there are no injuries identified, we allow for clear liquid diet (CLD) immediately after surgery. Similar to some enhanced recovery after surgery (ERAS) protocols for abdominal MIS, we also recommend multimodal pain control including per oral administration, ambulation on postoperative day 0 if able, advancement of diet as tolerated, initiation of bowel regimen, etc. If injuries were identified and the patient necessitated repair (i.e., bowel resection), we recommend following with institutional or surgeon preference for postoperative care.
Results
Diagnostic laparoscopy for penetrating abdominal trauma has been shown by O'Malley et al. in a large review of the literature to have a sensitivity ranging from 66.7% to 100% and specificity ranging from 33.3% to 100%. 5 The potential accuracy of laparoscopy in identifying injuries can be further improved with the implementation of systematic abdominal inspection, intraoperatively changing patient positioning to increase visibility, and utilizing atraumatic graspers to fully evaluate bowel. 3 By using such techniques, the rate of missed injury can decrease down to 0%–1%. 3 In a retrospective study performed by Marwan et al. in 2010, the outcomes for hemodynamically stable pediatric patients who suffered both blunt abdominal trauma and penetrating abdominal trauma were evaluated. They found that because of diagnostic laparoscopy, laparotomy was successfully avoided in 13 out of 21 patients overall and 10 out or 10 patients who had PAT. 6 O'Malley et al. performed a systematic review of the literature that included 2569 pediatric patients who suffered penetrating abdominal injury and subsequently underwent diagnostic laparoscopy. They estimate that the conversion rate to laparotomy is ∼33.8%. 5 Similarly, a multiinstitutional study performed by Alemayehu et al. evaluated 200 pediatric trauma patients who underwent either laparoscopy or thoracoscopy for trauma. Laparoscopy was performed in 187 of the total subjects and a laparotomy conversion rate of 36% was reported. 7 Furthermore, the most common reason for conversion to open procedure was for treatment of a bowel injury. 7 Perhaps the most feared complication of laparoscopy for trauma is the potential for missed injury, but it should be noted that multiple studies that evaluated MIS for trauma have reported a missed injury rate of 0% in the pediatric trauma population.4,7 But surgeons should be aware of the false-negative rate of diagnostic laparoscopy for trauma as it has been reported to be as high as 19% previously. 3 Other complications to be cognizant of include but are not limited to trocar site injury, air embolism, and bowel injury. 3
Discussion
Laparoscopy is safe and effective in the diagnosis and treatment of pediatric trauma patients when compared with laparotomy and should be considered in those patients who present with hemodynamic stability. One guiding principle to consider is the idea that we as providers should limit the trauma to the patient. This includes avoiding an unnecessary laparotomy as this may confer a longer recovery time and increased risk for postoperative complications. To date, there is growing body of literature to support the use of MIS for trauma as it may be associated with decreased length of stay, postoperative complications, readmission rates, and hospital cost.2,4,8 A retrospective chart review performed by Marks et al. in 1997 compared the total hospital costs incurred by trauma patients who underwent a diagnostic laparoscopy versus a negative laparotomy or diagnostic laparoscopy that necessitated conversion. They found a significantly less total cost for those patients who underwent diagnostic laparoscopy when compared with both the laparotomy and conversion groups: $5427 versus $7026 and 7855, respectively (P < .005). 8
It is worth reiterating that we do not recommend laparoscopy instead of laparotomy as those patients in whom laparotomy is indicated should proceed with appropriate management. Rather, we propose that those select trauma patients who are hemodynamically stable with a suspicion for hollow viscus injury or other concerning features that do not warrant a laparotomy, MIS should be considered. In conclusion, laparoscopy is a safe and effective tool in the diagnosis and treatment of the hemodynamically stable pediatric trauma patients and should be considered especially when there is concern for possible hollow organ injury.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received in the writing of this article.