
Abstract
Background:
Defecation status is an important determinant of quality of life. Previous studies showed that postoperative defecation disorders occurred after open surgery for ulcerative colitis (UC), but few have investigated defecation status after laparo-assisted surgery. The added precision and magnification provided with laparo-assisted surgery should lead to less damage to the anal sphincter muscle. This study investigated defecation function after a laparo-assisted restorative proctocolectomy (RPC) with ileal pouch anal anastomosis (IPAA). We also clarified factors that worsened defecation status.
Methods:
This retrospective study included 57 patients who underwent laparo-assisted RPC with IPAA for UC from January 2000 to May 2019. At 1 year after surgery, functional outcomes were evaluated with the Kirwan classification and Wexner score. Risk factors for poor defecation status were investigated with multiple regression.
Results:
At 1 year after surgery, the median Kirwan classification score was 2 and the median Wexner score was 8. Defecation disorder was observed in 19 (33.3%) patients, according to the Kirwan classification, and 15 (26.3%) patients, according to the Wexner score. Hand-sewn IPAA was associated with defecation disorder (P = .04), evaluated with the Kirwan classification. Hand-sewn IPAA (P = .01), older age (P = .03), high body mass index (P = .04), and the surgical indication (cancer/dysplasia; P = .03) were significantly associated with defecation disorder, evaluated with the Wexner score. The multivariable analysis showed that hand-sewn IPAA was an independent risk factor (P = .049; odds ratio: 4.99; 95% confidence interval: 1.0–28.39).
Conclusions:
We found that hand-sewn IPAA was a risk factor for defecation disorders after laparo-assisted RPC for UC.
Introduction
Ulcerative colitis (UC) is an idiopathic chronic inflammatory disease, which is increasing in prevalence. UC is characterized by relapsing and remitting mucosal inflammation, which starts in the rectum and generally extends proximally in a continuous manner.1,2 The basic treatment for UC is medication; the main medications are amino salicylate, steroids, immunosuppressants, and biological drugs, which include adalimumab, infliximab, golimumab, ustekinumab, vedolizumab, and tofacitinib.3,4 The rate of drug prescriptions has increased over time, and accordingly, the probability of requiring surgery has decreased. 4 However, the number of patients who require surgery has remained high, due to the increasing prevalence of UC.
The surgical indications for UC include toxic megacolon, hemorrhage, perforation, tumor formation, and failing to achieve remission. 5 In addition, an increasing number of patients with UC also develop cancer or dysplasia. 4 Depending on the indication for surgery, some surgical and anastomosis procedures might require modification, but the standard surgical procedure is a restorative proctocolectomy (RPC) with an ileal pouch anal anastomosis (IPAA).
Previously, open surgery was the main operative method for treating UC, but after the first report on a laparo-assisted RPC with IPAA, in 1992, the frequency of laparo-assisted RPC gradually increased, and surgical outcomes were reported. 6 Although many studies have reported postoperative defecation disorders after open surgery for UC, we lack studies that assessed defecation function after laparo-assisted RPC.6–12 Laparoscopic surgery is expected to minimize the damage to the anal sphincter muscle, due to its enhanced precision and magnification. Therefore, this study aimed to investigate defecation function after laparo-assisted RPC with IPAA and clarify the factors correlated with defecation disorders.
Methods
Surgical procedure
For UC with cancer or dysplasia, the typical treatment was RPC and hand-sewn IPAA, with a mucosectomy of the anal canal. For refractory or severe UC, the typical treatment included IPAA stapling without a mucosectomy. Stapled IPAAs were performed with a circular stapler (double-stapling technique). However, in cases of severe inflammation around the anal canal, a hand-sewn IPAA was typically performed. Some patients initially underwent a subtotal colectomy, as an emergency surgery for acute exacerbation; this was followed by a secondary surgery that included a residual rectum resection and an IPAA. A diverting ileostomy was created at the surgeon's discretion. Most procedures involved the creation of a 15-cm-long ileal J-pouch and a diverting ileostomy on the oral side, 30–80 cm from the IPAA. Therefore, the surgical procedure could include up to three phases, based on whether the colorectum was removed in one stage, whether a diverting ileostomy was created, and whether stoma closure was performed. The study protocol was approved by the Institutional Review Board of Osaka University Hospital (No. 15028).
In our institution, we generally performed surgery with laparoscopic assistance. Initially, we performed hand-assisted laparoscopic surgery (HALS). Over time, the use of laparoscopic surgery gradually increased, because laparoscopy is less invasive, in terms of the surgical wound (Fig. 1). These procedures are compared in Figure 2, which shows representative intraoperative views of HALS (Fig. 2A and Supplementary Movie S1) and laparoscopic surgery (Fig. 2B and Supplementary Movie S2). With laparoscopy, the magnification feature provided the ability to perform more precise surgery, particularly around the rectum, which is difficult to access in open surgery. In addition, magnification made it possible to identify and avoid damaging nerves during the operation. Furthermore, the resection line can be determined according to each case, and bleeding can be minimized.
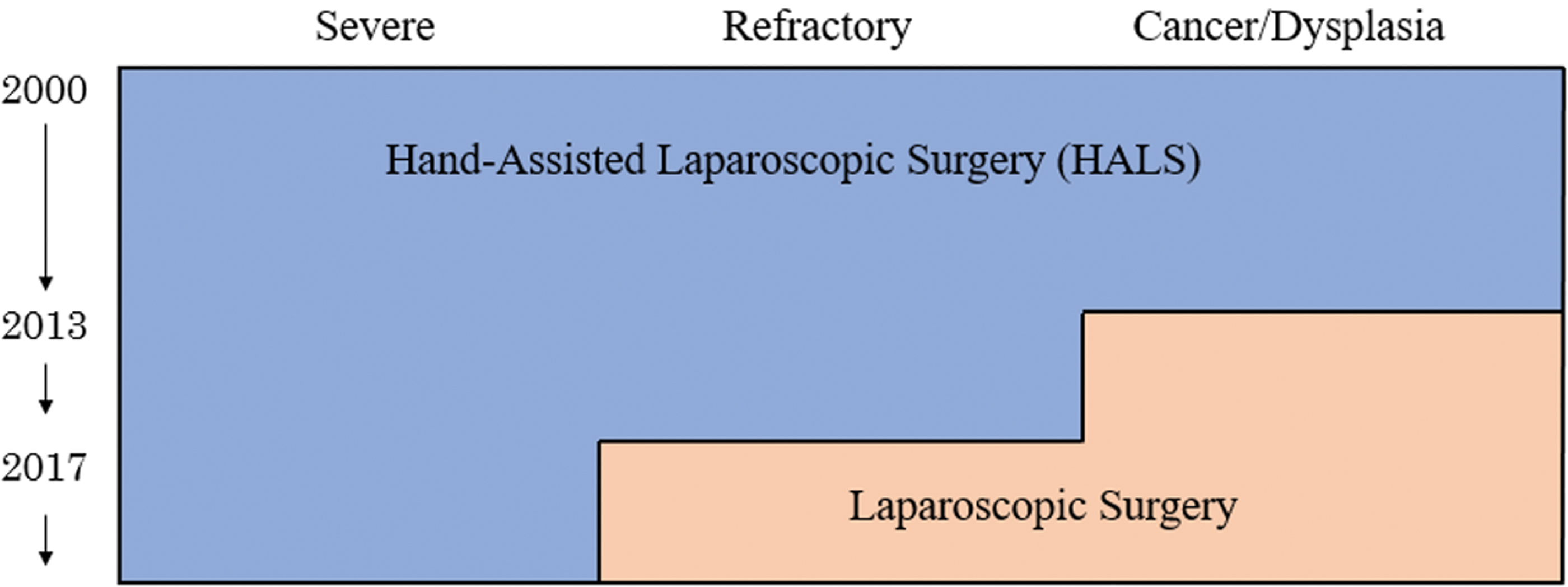
Changes over time in surgical methods for an RPC with IPAA. Laparoscopic surgery became more common over time, for treating refractory UC and UC with cancer/dysplasia. IPAA, ileal pouch anal anastomosis; RPC, restorative proctocolectomy; UC, ulcerative colitis. Color images are available online.
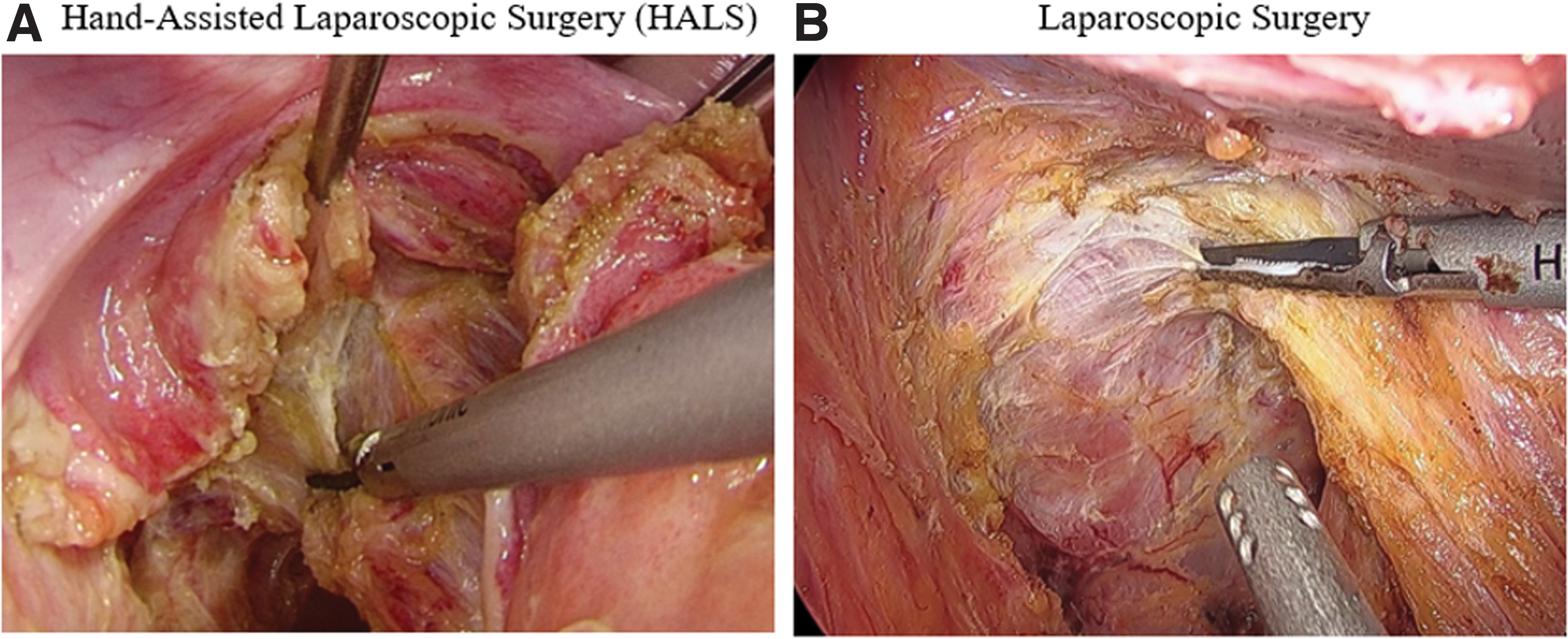
Intraoperative images of a perirectal dissection.
Study population
This retrospective study included patients with UC who underwent laparo-assisted RPC with IPAA at Osaka University Hospital, between January 2000 and May 2019. We excluded patients who had insufficient data or required a conversion to open surgery. Informed consent was obtained from all patients before the operation. The study protocol was approved by the Institutional Review Board of Osaka University Hospital (No. 15028).
Questionnaires and definition of defecation dysfunction
At 1 year after the RPC with IPAA or stoma closure, patients were surveyed with a questionnaire for collecting data on the Kirwan classification, the Wexner score, and the frequency of bowel movements.13,14 The Kirwan classification is a simple scale for assessing the frequency of fecal leakage; the score ranges from 1 to 4, where 4 indicates severe incontinence. 13 The Wexner score evaluates lifestyle alterations, the need for an incontinence pad, and the presence of incontinences to solid, liquid, and gas. The score ranges from 0 to 20, where 20 indicates severe incontinence. 14 In this study, defecation disorder was defined as a Kirwan classification of 3 or 4 or a Wexner score of 13 or higher.
Statistical analysis
All statistical analyses were performed with JMP pro 14.0.0 (SAS Institute, Inc., Cary, NC). Demographic variables were compared between groups with the Wilcoxon signed rank test, for continuous variables, and Fisher's exact test, for categorical variables. Binary logistic regression was performed for analyzing multivariable associations between potential influencing factors and defecation disorder. Linear relationships were assessed with the Pearson correlation analysis. An ROC curve analysis was performed to determine an appropriate cutoff value for predicting the risk of developing a defecation disorder. P-values <.05 were considered significant.
Results
Patient characteristics
During the study period, 71 patients underwent RPC with IPAA for UC. We excluded 3 patients who underwent open surgery and 11 patients with incomplete data. Thus, 57 patients were included in the analyses. The patient clinical characteristics are shown in Table 1. Among 57 patients, 38 (66.7%) were male, the median age at surgery was 49 years, and the median body mass index (BMI) was 20.4 kg/m2. The main surgical indication was cancer/dysplasia (n = 20 patients, 35.1%). HALS was performed for 17 patients (29.8%), and laparoscopic surgery was performed for 40 patients (70.2%). The IPAA was stapled in 36 patients (63.2%), and hand-sewn in 21 patients (36.8%). The main surgical strategy was a two-stage surgery (84.2%).
Patient and Operative Characteristics of Patients with Ulcerative Colitis
Data are presented as the n (%) or median (range), as indicated.
HALS, hand-assisted laparoscopic surgery; TNF, tumor necrosis factor.
Postoperative defecation status
At 1 year after surgery, the median Kirwan classification score was 2, and the median Wexner score was 8. Defecation disorder was observed in 19 patients (33.3%), according to the Kirwan classification and 15 patients (26.3%), according to the Wexner score. These results were superior to those previously reported for open surgery for UC. 7
Distributions of the Kirwan classification and Wexner scores are shown in Figure 3. We found that the Kirwan classification score was positively correlated with the Wexner score (r = 0.63, P < .001).

Scatterplot of the Wexner scores and the Kirwan classification scores. Red dots indicate patients with defecation disorder; the line shows the Pearson correlation fit. Color images are available online.
Factors related to defecation disorder
To investigate factors potentially related to defecation disorder, we compared observations between patients with and without postoperative defecation disorder. Defecation disorders were defined according to either the Kirwan classification score (Table 2) or the Wexner score (Table 3).
Association Between Potential Risk Factors and Defecation Disorder, Defined with the Kirwan Classification
Data are presented as n (%) or median (range).
HALS, hand-assisted laparoscopic surgery; TNF, tumor necrosis factor.
Associations Between Potential Risk Factors and Defecation Disorder, Defined with the Wexner Score
Data are presented as n (%) or median (range).
HALS, hand-assisted laparoscopic surgery; TNF, tumor necrosis factor.
As shown in Table 2, according to the Kirwan classification, the incidence of defecation disorder was significantly different between patients treated with the stapled and hand-sewn anastomosis methods. Patients treated with a hand-sewn IPAA had a higher incidence of defecation disorder than those treated with the stapled IPAA. According to the Wexner score (Table 3), the hand-sewn IPAA (P = .01), older age (P = .03), a high BMI (P = .04), and a surgical indication (cancer/dysplasia; P = .03) were significantly associated with defecation disorder. As shown in Table 4, the multivariable analysis results showed that the hand-sewn IPAA was an independent risk factor for defecation disorder (P = .049; odds ratio: 4.99; 95% confidence interval: 1.0–28.39).
Multivariate Analysis of Associations Between Potential Risk Factors and Defecation Disorder, Defined with the Wexner Score
The risk of developing a defecation disorder was not significantly associated with the distance from the anastomosis to anal verge, the operative method, the gender distribution, or the preoperative medication. These factors were similar between groups, when either the Kirwan classification or the Wexner score was used to define defecation disorder.
Discussion
UC typically causes gastrointestinal symptoms, including bloody diarrhea, abdominal pain, fecal urgency, and tenesmus. 15 These symptoms are important in the diagnosis of UC. Although multiple drugs are available for treating the disease, about 15% of patients require surgical treatment. However, even after surgery, postoperative defecation status is reported to be poor. Currently, although many studies have reported functional defecation after an open RPC with an IPAA, postoperative defecation disorders have occurred at high frequencies.7,8 Previous studies reported that old age, pelvic sepsis, pouch fistula, anastomotic leakage, the distance between the anastomosis and the anal verge, and hand-sewn IPAAs were risk factors for defecation disorders after surgery for UC.16–20 However, those studies did not distinguish between laparoscopy and other surgical methods. To the best of our knowledge, this study is the first to focus on patients undergoing laparo-assisted surgery. We found that age and the distance between the anastomosis and the anal verge were not associated with postoperative defecation disorders. In contrast, we found that stapled IPAAs provided better functional outcomes than hand-sewn IPAAs, regardless of whether the Kirwan classification or the Wexner score was used. This risk factor was also associated with poor outcomes after open surgery.
In a large-scale survey that includes 1310 patients with UC, 51% of patients displayed Kirwan classifications of 3 and 4 at 1 year after open surgery. In contrast, our results showed that only 33.3% of patients displayed Kirwan classifications of 3 and 4 after laparo-assisted RPC. These data suggested that laparo-assisted IPAA provided better functional outcomes than the open IPAA. This finding contrasted with findings in rectal cancer surgeries that preserve the anus, such as a low anterior resection. Those studies showed no difference in postsurgery defecation function between the laparoscopic and open surgery approaches. 21 Therefore, the use of laparoscopy for UC appeared to provide an advantage, in terms of postsurgical defecation function, which was not observed in cancer surgery.
This study had several limitations. First, our results were based on a single-center retrospective study with a small sample size; moreover, none of our patients experienced postoperative complications related to defecation function. Second, we only assessed defecation disorders at 1 year after surgery. A future study should evaluate whether defecation disorder persists in the long term, because UC is a benign disease, and patients survive for a long time after surgery. Third, preoperative defecation status was not assessed. This study could have been more interesting, if we could have evaluated the change in defecation, from pre- to postsurgery.
Conclusions
We found that, at 1 year after surgery for UC, defecation disorder occurred in 33.3% of patients, when defined with the Kirwan classification, and in 26.3% of patients, which defined with the Wexner score. We also found that hand-sewn anastomosis was a significant risk factor for defecation disorder after laparo-assisted RPC with IPAA.
Footnotes
Acknowledgment
The authors thank San Francisco Edit for English language editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a research grant from the Osaka Medical Research Foundation for Intractable Disease and Danone Institute of Japan Foundation (DIJF R01-24).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.