
Abstract
Background:
Economic evaluation in health care is becoming increasingly important. Laparoscopic appendectomy (LAp) is one of the most frequent minimally invasive procedures in the pediatric population. The increased costs of this approach in any indication could be justified by proving its cost-utility in terms of health-related quality of life (HRQoL). We aim to perform a cost-utility analysis between open and LAp (open appendectomy [OAp] and LAp).
Materials and Methods:
We included the data of children operated for acute noncomplicated appendicitis, who agreed to answer a validated quality of life (QoL) questionnaire. Costs were calculated for each patient. We established a threshold for cost-effectiveness (λ) of 20,000 to 30,000€ per quality adjusted life year (QALY) according to previous research.
Results:
A total of 53 patients were included. Overall mean costs in the OAp were 758.98€ and in the LAp 1525.50€. The incremental cost-effectiveness ratio was 18,000€/QALY, under the threshold of cost-effectiveness, therefore favoring the laparoscopic approach as it improves HRQoL despite the costs.
Conclusions:
Economic evaluation studies in Pediatric Surgery are scarce and rarely measure outcomes in terms of QoL. This information is important in the decision-making process for institutions and health-care professionals. Our results encourage the use of laparoscopy in pediatric appendectomy to improve HRQoL in our patients.
Introduction
Economics is the branch of knowledge that investigates the best possible way to allocate limited resources that may have alternative uses. 1 This is especially true in Health Economics. Every resource we use in an intervention, regardless of whether it is related to health care professionals, equipment, or use of spaces, has an opportunity-cost, because we could be using these resources on something else.
Minimally invasive surgery (MIS) was first developed in an attempt to minimize a patient's surgical trauma, improve outcomes, and facilitate recovery after operation. Considering the advanced technology and increased operational times that MIS procedures might require, it has an undeniable increase in costs.2,3 However, evidence in the adult population seems to indicate that the decrease in hospital stay and earlier return to normal activity compensate for this cost increase. 4 In fact, in General Surgery, MIS has already proved to be cost-effective in many procedures.5–7
Regarding pediatric MIS, it already has proved its safety and feasibility in many indications and its use has spread widely.8–10 Moreover, randomized controlled trials have been carried out in the most prevalent conditions such as acute appendicitis, inguinal hernia and pyloromyotomy, with results favoring the minimally invasive approach.11–13
However, few studies have focused on the economical evaluation of pediatric MIS. Most of those carried out compare the costs of the laparoscopic procedure and of the postoperative course or hospital stay, without taking into account quality-of-life (QoL) measurements.14,15 Cost-benefit of pediatric MIS might be difficult to prove. The more frequent procedures in Pediatric Surgery are done on a day-case surgery basis, and even in acute noncomplicated appendicitis, children are discharged shortly after surgery.
Cost-utility analysis (CUA), on the contrary, does not focus on the monetary aspects of the consequences of an intervention, but on health-related effects. We take into account the health-state and the quality of this health-state as well. In this way, we can compare different interventions without the limitations of some monetary or disease-specific outcome measurements. 16
The aim of this study is to perform a CUA between open and laparoscopic appendectomy (LAp) in acute noncomplicated appendicitis in children to prove the hypothesis that LAp is superior to open appendectomy (OAp) in terms of health-related quality of life (HRQoL) and cost-effectiveness.
Materials and Methods
Type of study and population included
This is a retrospective analytical economic cost-utility study.
We have included all patients between 8 and 15 years old diagnosed with acute noncomplicated appendicitis operated in two Pediatric Surgical Centers from September 2017 to August 2020 whose parents agreed to participate answering to a validated Pediatric QoL questionnaire. The lower limit of 8 years old was established because this is the minimum age for which the questionnaire has been validated.
Criteria to define uncomplicated appendicitis are the following: less than 2 days of symptoms and no clinical or radiological findings of phlegmon and intra-abdominal abscess or peritonitis.
The study was revised and approved by the Ethics Review Board of both participant centers. Ethics Review Board of Complejo asistencial Universitario de León. 30/3/2021 Reg n. 2143.
Ethics Review Board of Fundació Asistencial Mútua de Terrassa 28/10/2020 Reg n. p/20-164.
Protocols for noncomplicated appendicitis and details of intervention
The protocol followed in both centers was the same. Patients underwent open or laparoscopic surgery depending on surgeon's choice and availability of the equipment.
For LAp, we performed a standard three-port technique as previously described. 17 The appendix was transected by endostapler or sectioning between endoloops depending on surgeon's preference. Some surgeons chose to use an endosealer device in certain cases. For OAp, we followed the classical Rocky Davis approach with limited incision. 18 All surgeons from each center operated on patients from the two groups.
Cost estimation
We considered direct costs for the study. Intraoperative costs, hospital stay, and postoperative follow-up appointments were included. Information on costs was provided by the two participating centers.
The intraoperative costs were calculated for each patient.
For laparoscopic hardware and reusable instruments, we considered a life span of 10 years. We calculated the mean number of times they are used per year and an equivalent cost was estimated for each patient, dividing the total amount per 10 years (approximate life span) and per patients-per-year.
Regarding operating room consumables, such as maintenance, sterilization of the instruments, anesthetics, and so on, we considered them to be similar between both groups, as well as health care professionals working in theater.
We documented analgesic and antibiotic consumption and calculated the prices according to the doses received by each patient during hospital stay.
The price of each day at the hospital was calculated from standard hospital statistics that already include salaries of nurses and staff and other expenses. The total cost of hospital stay was calculated by multiplying the day price by the days each patient was in hospital.
Health-related QoL
We measured children's QoL with the general questionnaire KIDSCREEN19–21 validated in Spanish. 22 We chose KIDSCREEN-10 because its extrapolation to quality-adjusted life-years (QALYs) has been previously reported, which is the standard measure of HRQoL in CEA and CUA. We obtained the QALYs for each patient using the mapping algorithm described by Chen. 23
Sensitivity analysis and acceptability curve
We followed the principles for reporting results published in the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement extended for nonpharmacological Trials. 24
Sensitivity analysis was used to transfer the uncertainty of different estimations to the outcomes of our model, comparing them with different possible values. A probabilistic multivariate sensitivity analysis was done with 5000 Monte Carlo Simulations (MCS). We calculated the 95% confidence interval of the results of this sensitivity analysis. We used a cost-effectiveness plane to show each pair of costs and outcomes of the model.
We established a cost-effectiveness acceptability line to determine the LAp cost-effectiveness to OAp with a reasonable level of willingness-to-pay. This concept means how much money we would pay to improve QoL measured in QALYs.
We established a 20,000 to 30,000€-per-QALY threshold (λ) for cost-effectiveness as it is widely accepted in literature and is a frequently used value in many health care cost-effectiveness analyses. 25
A 3% discount rate per year was applied for the estimation of costs and QALYs, following current health economic guidelines. 26
We calculated the incremental cost-effectiveness ratio (ICER) of LAp in relationship to OAp. This figure means how much money we are spending using LAp over OAp divided by the difference in QALYs between LAp and OAp. If the ICER of LAp were not to exceed the threshold limit established, it will be considered cost-effective. It will mean that the increase in costs with LAp is under the limit we have established, representing what we are willing to pay to improve QoL.
We decided to undertake our analysis from the perspective of the health-provider.
General statistics
For statistical analysis, we used the IBM SPSS Statistics version 23.0 (IBM Corporation, Armonk, NY)
To compare the two study groups, we performed a statistical analysis for independent samples. We ran a Kolmogorov-Smirnov test for each variable to check for normality and compared the basal characteristics of both groups.
For general descriptive statistics, quantitative data are expressed as mean and standard deviation, or median and minimum and maximum values in variables that do not follow normal distribution. Categorical data are expressed as frequencies with percentage (%).
Nonparametric tests were used for the analysis and continuous data were assessed with Mann–Whitney U tests. Multivariable linear regression models were developed using the Spearman test. A P value of <.05 was considered statistically significant.
Results
Fifty-three patients met the inclusion criteria and agreed to participate by answering to the KIDSCREEN-10 questionnaire.
None of the data gathered followed a normal distribution according to the results of the Kolmogorov-Smirnov test.
There were 37 (69.8%) boys and 16 (30.2%) girls ranging in age from 8 to 14 years, with a median of 10 years. At the time of surgery, the appendix was macroscopically phlegmonous in 77.4% of cases and gangrenous in 22.6%. Regarding the approach, there were 27 OAp and 26 LAp. The characteristics of each group are summarized in Table 1.
Demographic and General Data
LAp, laparoscopic appendectomy; OAp, open appendectomy.
Both groups, OAp and Lap, were homogeneous without differences in gender or type of appendicitis. The median age was lower in the OAp group (10 versus 12), and this difference was statistically significant (P = .008). We did not detect any significant difference in hospital stay nor were there any complications in either group.
The costs for the LAp group ranged from 685.53 to 2082.53€ with a median value of 1711.25€ for patient. Intraoperative costs related to laparoscopic equipment ranged from 232.41 to 1307.15€ in cases where both the endosealer and endostapler had to be used. The costs for the OAp group ranged from 465.03 to 2122.99€, with a median value of 465.91€. These variations depended only on hospital stay, with an outlier value of 2122.99€ due to a hospital stay of 6 days in 1 patient. LAp represented an increase in costs, with a statistically significant difference between the median values of 1245.34€ (P < .001) (Fig. 1).
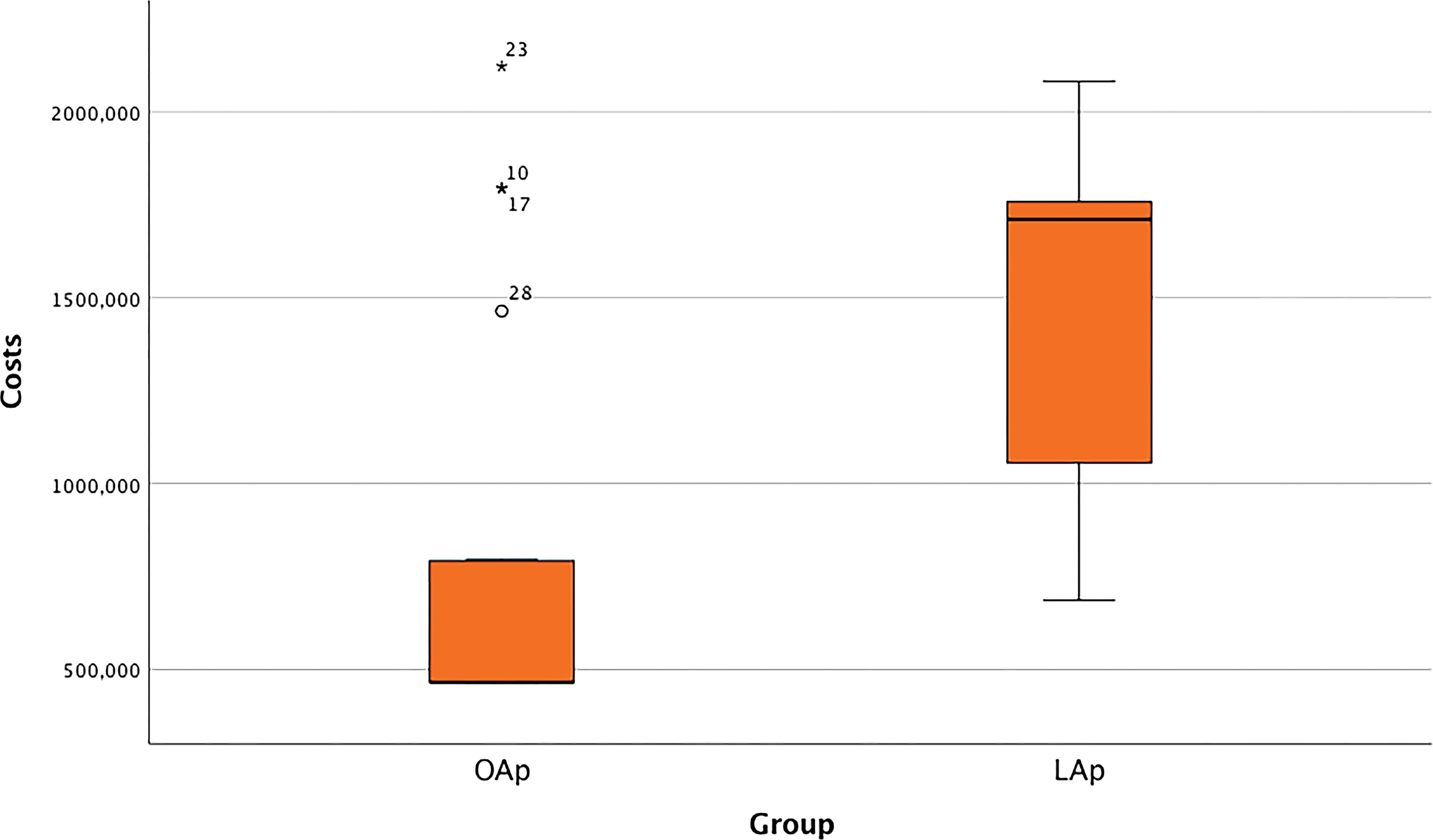
Box plot showing differences in costs between the two groups. Color images are available online.
Regarding the results of the KIDSCREEN questionnaire, patients from the OAp group scored better in one general item related to emotional wellbeing. However, in the LAp group, scores were significantly better in items related to the specific areas of relationships with friends and family, and in those related to performance and getting back to school. In the remaining items (such as use of leisure time or feelings of loneliness or sadness) there were no statistically significant differences.
When considering QALYs, the median value in the OAp group was 0.75 (0.67–0.82) and in the LAp group was 0.77 (0.66–0.88), but this difference did not reach statistical significance (P = .816) (Fig. 2).
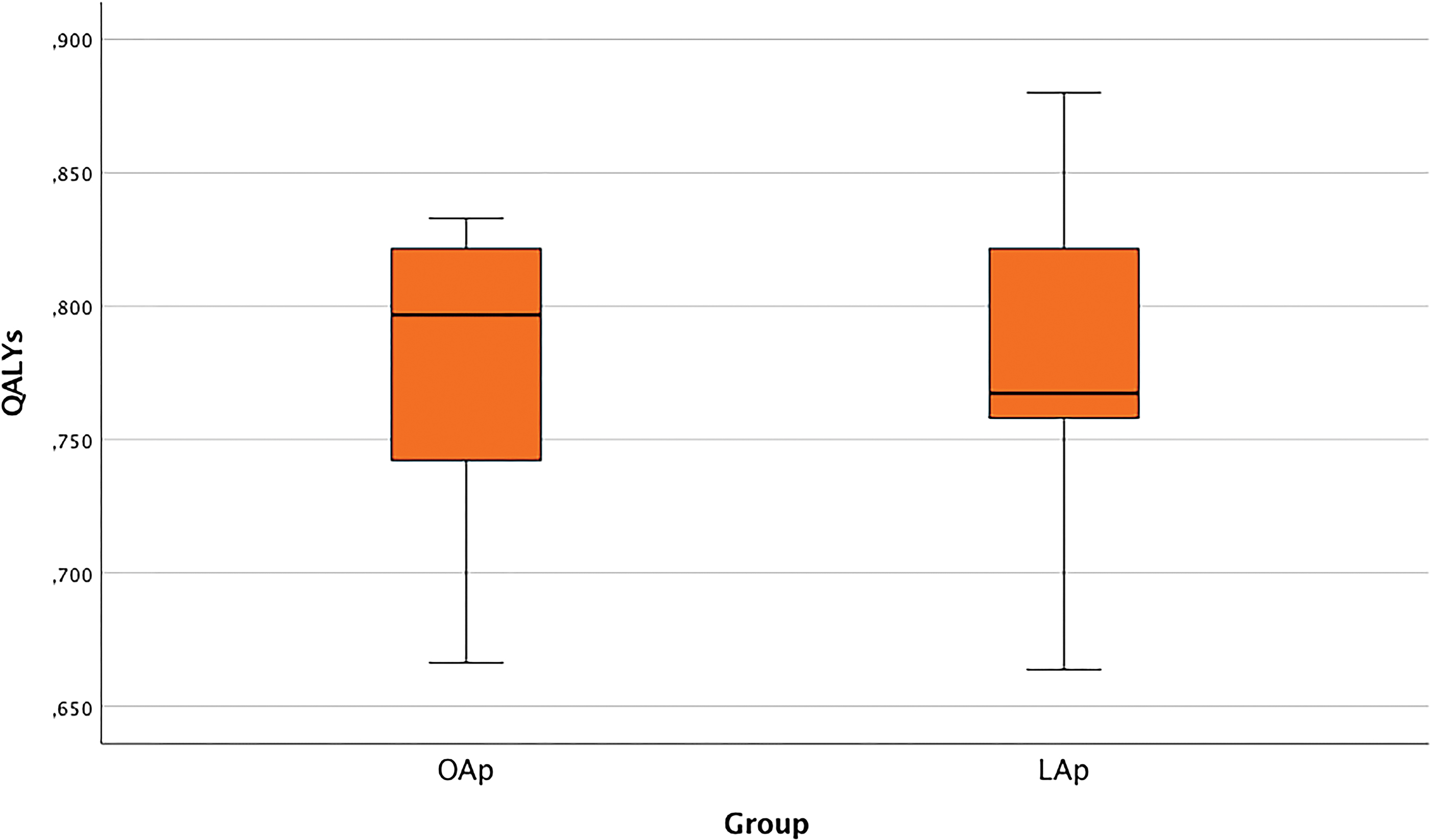
Box plot showing the distribution of QALYs in each group. QALYs, quality-adjusted life-years. Color images are available online.
The multivariate analysis considering the rest of the variables showed no significant correlation with QALYs: the variable “age” has no independent correlation with QALYs in the sample, neither did “type of appendix” nor “length of hospital stay.”
The results of the CUA are summarized in Table 2.
Summary of the Cost-Utility Analysis
ICER, incremental cost-effectiveness ratio; QALYs, quality-adjusted life-years.
The acceptability curve for LAp over OAp represents the probability that LAp is cost-effective according to the values we set as the threshold for willingness-to-pay. Here, we can see where our threshold of 20,000 to 30,000€/QALYs is located (Fig. 3).

Acceptability curve. WTP, willingness to pay. Color images are available online.
The ICER of choosing LAp over OAp was 18,122.73€/QALY, which is just below the cost-effectiveness threshold λ set at 20,000 to 30,000€/QALY.
Figure 4 shows the graphical representation of the probabilistic simulations generated to prove our model (MCS). We can see that most of the simulations are under the cost-effectiveness threshold. This means that the increase in costs divided by the increase in QALYs, which is how much money we are spending to gain a QALY, is under the limit of what we are willing to accept.

Incremental cost-effectiveness plane. The continuous line is the threshold λ of 20,000€/QALY and the dotted line is the 30,000€/QALY one. QALYs, quality-adjusted life-years. Color images are available online.
Discussion
All the achievements that have led to the present development of MIS have been progressive and have involved different areas. Besides technical advancements, a favorable and supportive environment is also needed. Society and policy makers alike must be convinced not only of its safety and efficacy but also of its cost-effectiveness.
This is why the economic analysis of health care is important not only for the provider and governmental policy makers but also for surgeons. We have a commitment to ensure that these studies take into account our patients' QoL, and not only monetary outcomes.
Measuring QoL is not an easy task. The KIDSCREEN group is an international team of health professionals who have endeavored to overcome the limitations of the international pediatric QoL instruments, by providing measures suitable for children, teenagers, and parents to both evaluate and monitor HRQoL in different settings.27,28
However, we consider that it would be useful to develop specific assessment tools for pediatric surgery, especially for younger children.
Our results show an ICER for LAp of 18,122.73€/QALY, just below the threshold of 20,000 to 30,000€/QALY. This means that although the expenses in the LAp group were significantly higher, they are justified as they were associated with an increase in HRQoL and at the same time remained under the λ threshold of what we are willing to pay to improve QoL.
We are convinced that pediatric MIS is the future of Pediatric Surgery, especially for long complex procedures that require larger incisions and have a more painful postoperative recovery. However, to reach this point with advanced surgeries, we have to first implement MIS in both elective and routine procedures, and reach standards of quality of care in all centers, regardless of their volume of patients or funding.
We should also continue working to improve the costs to try to reach an even more favorable ICER.
For instance, pediatric surgeons could team up with other surgical specialists with a special interest in MIS to share equipment and hardware. This could be particularly useful in low-volume Pediatric Surgery Centers because when we share the most expensive MIS technology, the number of cases per year increases and the proportional total costs per patient decreases.
Regarding the use of instruments, mechanical devices have failed to prove superiority over endoloops for ligating the appendix in noncomplicated appendicitis, and the latter are much cheaper. 29 Similarly, in many cases, dissection of the mesoappendix can be safely done by electrocautery, diminishing the costs considerably by avoiding the use of endosealer. Obviously, the surgeon has to have all the possible resources available in case of complex cases that require the use of more expensive technology, and it is the surgeon's choice to use the most suitable instrument in each case.
We like to highlight the importance of training. Training allows us to improve both our general results and the cost-effectiveness of our MIS procedures because it helps us reduce operative times. Operative time also has a cost-opportunity so, by reducing it, we will improve our cost-effectiveness as well.
Our study has some limitations. First of all, its retrospective and, therefore, nonrandomized nature. Owing to a lack of published articles considering HRQoL in pediatric MIS, we wanted to have preliminary results with a retrospective study to set the basis for future prospective research.
We have included a reduced number of patients, partially due to this retrospective nature, we could not contact some of the patient's families operated in those years. We were also limited to no-complicated appendectomy and, by using the KIDSCREEN questionnaire, we could only include patients older than 8 years (the minimum age for which the questionnaire has been validated). However, the MCS allowed us to overcome this limitation by permitting us to simulate different scenarios to obtain sufficient data from which to draw conclusions.
Conclusion
LAp for noncomplicated appendicitis in children is cost-effective over OAp in terms of HRQoL.
Future prospective and randomized research should be undertaken, in which we could evaluate the HRQoL from the very precise moment of the indication in any pediatric MIS procedure and during the postoperative period.
Gathering information on costs and HRQoL in future studies may provide us with further insight into the economic and social perspective of pediatric MIS and its final outcomes in terms of children's QoL.
Footnotes
Authors' Contributions
All the authors have substantially contributed to this article and all approve the final version of it. They all have participated in design, data acquisition, analysis, and interpretation of data for the work. They have all participated in drafting the work or revising it critically for important intellectual content. They all agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
We thank Caroline Coope for her help in language editing.
Disclosure Statement
None of the authors has any competing interests, personal financial interests, or other interests regarding funding or employment.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.