
Abstract
Objective:
Today, it is recommended that the laparoscopic cholecystectomy (LC) is made with standard three ports. In this study, we aimed to determine the preoperative and intraoperative factors that require the use of an additional fourth port during three-port LC.
Materials and Methods:
All patients who started LC with three ports between January 1, 2018 and December 31, 2019 were included in the study. The patients were divided into two groups as those who underwent three-port LC and those who required additional ports. Independent parameters affecting the transition from three ports to four ports were analyzed using logistic regression analysis. The patients who underwent LC with three ports were included in Group 1 and the patients requiring an additional port were included in Group 2.
Results:
A total of 234 patients (139 women and 95 men) were included in the study. The average age of patients was 52.95 ± 16.26 (20–89) and body mass index is 28.64 ± 5.4 (15.73–48.89), respectively. Three ports were used in 148 patients (Group 1), and an additional fourth port was used in 42 patients (Group 2). Female gender, history of upper laparotomy, presence of acute infection findings, urgent surgery, and advanced age were observed to increase the use of additional ports. In multivariate analysis, it was shown that the presence of hepatic barrier (P < .001) and the presence of complete adhesion in the gallbladder (P < .001) significantly increased the use of additional trocars during LC. In addition, female gender was found to cause an increase of 6.62 times (P < .001).
Conclusion:
Many factors may require the use of additional ports during three-port LC. The use of an additional fourth port should not be avoided, especially in cases where hilum dissection is prevented due to liver origin, in female patients and in cases with complete adhesion to the gallbladder.
Introduction
Laparoscopic cholecystectomy (LC) is the first operation of choice in gallbladder pathologies, especially cholelithiasis, and it is used safely even in patients with anatomical anomalies and cirrhosis.1–4 Two more widely adopted techniques of LC (American and French), which were put into practice by Lyon Philip Mouret in 1987, have been widely used.5,6 However, over time, different technical methods of LC have been defined and applied. 7 The different approach emphasized first was the three-port LC instead of the standard four-port LC applied. 8 On the other hand, although three-port LC is mostly performed by experienced surgeons, it was stated that biliary and vascular injuries should be avoided by recommending the use of additional trocars in case of difficulty in dissection.9,10 As a result of a review, it was emphasized that clinical studies are still needed to evaluate the advantages of three-port LC effectively. 11 As a result of our review, we realized that no complicating factors were determined during three-port LC, and no objective parameter was emphasized in which situations should not be continued persistently using three trocars. In this study, we aimed to determine the factors that make it difficult to make a three-trocar LC safely.
Materials and Methods
This study was started with three ports in Yeni Yüzyıl University Gaziosmanpaşa Hospital General Surgery Clinic between January 1, 2018 to December 31, 2019, after obtaining the Ethics Committee approval from Istanbul Yeni Yüzyıl University Faculty of Medicine Ethics Committee on March 10, 2020 with the number 2020/03. Retrospective results of all patients who were administered were included. The most important factor in the selection of these dates was the routine video recording of all laparoscopic surgeries. Patients who resulted in open technique were excluded from the study. Two hundred thirty-four patients who underwent surgery by using a three-port laparoscopic technique were included in the study. Preoperative and intraoperative findings that may affect the use of additional ports were recorded
Preoperative and Intraoperative Parameters Viewed
BMI, body mass index; CRP, C-reactive protein.
Surgery technique
All of the surgeries were performed by a team who has more than 1000 four-port LC experience. Insufflation was routinely done by using a Veress needle. After the 10 mm trocar was inserted through the incision made under the umbilicus, the operating table was placed in a 30° reverse T gratedburg and 15° left lateral position. Under visualization, a second 10 mm trocar was inserted into the epigastric region from the right of the falciform ligament and a third 5 mm trocar was placed at the fundus of the gallbladder (Fig. 1a). In cases where the fundus of the gallbladder was not visible due to anatomical reasons or adhesion, a localization 3 cm below the subcostal margin at the right midclavicular line was preferred (Fig. 1b). In cases where three trocars were used, an additional trocar was added at the right anterior axillary line in cases of intraoperative difficulties. (Fig. 1c). Trocars were routinely inserted by transillumination with 30° camera light to prevent vascular injuries. The gallbladder cystic duct and cystic artery were dissected by blunt dissection and clipped, and then separated from the liver bed using Hook's tool. The gallbladder was removed from the epigastric trocar incision in all cases.
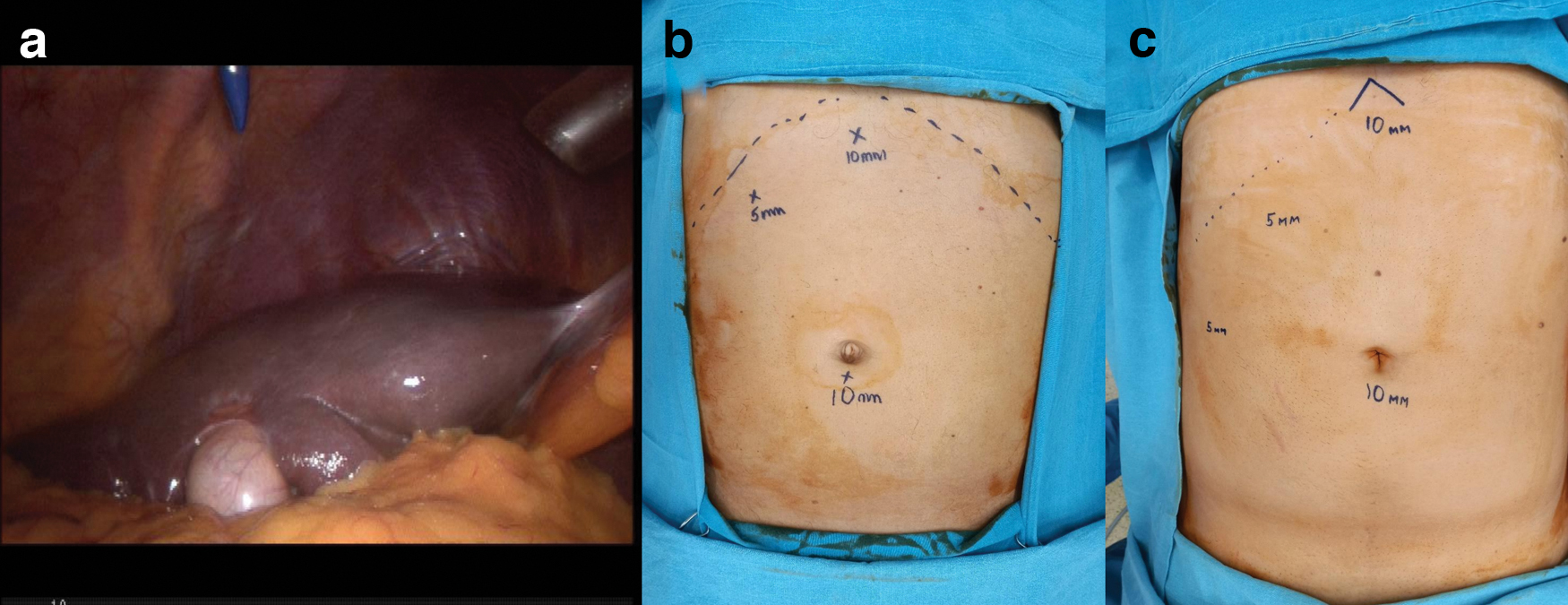
The trocar locations and dimensions we prefer in three-port LC:
Statistical analyses
Statistical analyses were performed using SPSS version 20.0 (SPSS, Inc., Chicago, IL, USA) software. Categorical variables of patient characteristics were compared using Pearson's chi-square test or Mann–Whitney U test as appropriate. For continuous variables, Student-T test was used. For the multivariate analysis, the possible factors identified with univariate analyses were further entered into the logistic regression (with “enter” method) analysis to determine independent predictors of conversion to four-port technique. Hosmer–Lemeshow goodness-of-fit statistics was used to assess model fit. All P-values from two-sided tests and a P value ≤.05 were considered statistically significant.
Results
Around 59.4% of the patients were female (139 patients) and 40.6% (95 patients) were male. The average age of patients was 52.95 ± 16.26 (20–89) and body mass index (BMI) is 28.64 ± 5.4 (15.73–48.89), respectively. Three-port LC was performed in 192 patients (82.1%) (Group 1) and an additional port was used during the three-port LC in 42 (17.9%) patients (Group 2). The mean patient age was 28.88 ± 15.4 years in the first group and 51.66 ± 16.2 years in the second group. The average age of patients in the first group was 28.88 ± 15.4 and while the second group was 51.66 ± 16.2. There was a significant difference in patient age between the two groups, and there were more elderly patients in the second group (P = .008). As a result of the univariate analysis, no significant difference was found between the groups in terms of chronic liver disease, BMI, time interval between acute attack and surgery, and preoperative C-reactive protein values. Edema in the gallbladder wall, hydropic gallbladder, severe inflammation in the gallbladder, urgent cholecystectomy, bleeding from the gallbladder bed, liver-induced barrier, dissection difficulty due to transverse colon distension, complete adhesion of the gallbladder, and previous upper abdominal surgery were found to be significantly higher in second group (Table 2).
Variables Found Significant in Univariate Analysis
SD, standard deviation.
In the multivariate analysis of the parameters that were significant in the univariate analysis, liver-induced barrier, female gender and total adhesion in the gallbladder were found to be significantly higher. It was observed that hepatic barrier increased the probability of additional ports by 141.67 times (P < .001, 95% confidence interval [CI]: 0.001–0.036), female gender was 6.62 times (P < .001, 95% CI: 0.001–0.036), and similarly, full adhesion in the gallbladder increased the probability of using additional ports 6.89 times (P < .001, 95% CI: 0.037–0.341) (Table 3).
Multivariate Analysis Results
CI, confidence interval.
Discussion
LC is still one of the most common operations performed in surgical clinics. Many studies that determine the factors that increase the risk of LC returning to open surgery have been started over time. Factors such as advanced patient age, obesity, previous laparotomy, presence of widespread adhesion, gallbladder perforation, and scleroatrophic appearance have been reported as risk factors for conversion to open cholecystectomy (OC).12–14 Due to the relatively high rates of bile duct and vascular injury compared with OC, a safe LC understanding has emerged over time and has been widely accepted. 15 One of the recommendations made for this purpose was the use of an additional fifth trocar. Nguyen et al. reported 11% additional use of the fifth trocar in their study of difficult LC patients with four trocars. 16 With the spread of different LC techniques over time, the risks of returning to open surgery and the factors that require the use of additional ports have started to be emphasized. 7
Three-port LC is the most preferred technique and it is at least as safe as four-port LC in studies; However, although it has been shown that it has advantages such as cost, reduction in scarring, reduction in the number of assistants needed during surgery, and reduction in the use of analgesia, it has been stated that there is no change in the duration of the operation and the duration of hospitalization.11,17 Therefore, it has been recommended to initiate the LC with a routine three trocar and use a fourth trocar only if there is difficulty in dissection. 18 Tagaya et al. reported the need for additional ports in three-port LC patients with a rate of 4.8%, and Ciftci et al. with 24.4% in their study.19,20 In our study, an additional port was required at a rate of 17.9% (42 patients). Although our fourth trocar usage rate is compatible with the literature, we think that our center is high because it is the advanced center where comorbid patients are referred and therefore more complicated patients are operated. Although Al-Azawi et al. and Hajibandeh et al. reported that three-port LC was successfully performed in patients with acute and chronic cholecystitis, they did not evaluate for the use of additional ports.9,18 In our study, there were 45.24% (42 patients) in the first group and 29.17% (56 patients) in the second group with acute infection and it was observed that acute infection increased the use of the additional fourth port (P = .002). Similar results are seen in factors associated with acute cholecystitis, such as gallbladder wall thickness, gallbladder hydrops, and urgent LC.
Bleeding during LC usually originates in the gallbladder bed when vascular structures are not injured, and has been reported in 1%–10%. 21 The use of an additional fifth trocar has been recommended to control such bleeding during the four-port LC. 16 In our study, bleeding from the gallbladder bed was significantly higher in the second group in which an additional port was used (Group 1 22.92% [33 patients]/Group 2 45.24% [19 patients]; P < .001). All of these patients had acute infection with widespread adhesions, so we think that the use of additional ports beforehand led to a significant statistical result. There was no significant difference in multivariate analysis.
In 9 patients (21.43%) in the second group, it was observed that a significant additional port was used due to colonic distension (P < .001) (Fig. 2). We did not find any study to compare this result in the literature. Kapoor et al. reported that in patients with acute infection, the transverse colon segment adjacent to the gallbladder was affected by inflammation and therefore dissection of the Calot triangle during LC was difficult. 22 It is thought that the preoperative and prolonged ERCP procedure may also cause this.23,24 In their own studies, Yadav et al. and Kapoor emphasized that there were colon injuries that developed during LC due to this reason.22,25 Although there are studies showing that factors, such as advanced patient age, previous upper laparotomy, chronic liver disease, and BMI, are risk factors for transition to OC, studies showing the opposite have also been reported.26–29 In our study, advanced patient age (P < .008) and previous upper laparotomy (P < .003) were found to be significantly higher in the univariate analysis in the second group. In our study, we could not reach the literature data that would compare these results and report the use of additional ports.

Absence of hilum due to transverse colon distension. Color images are available online.
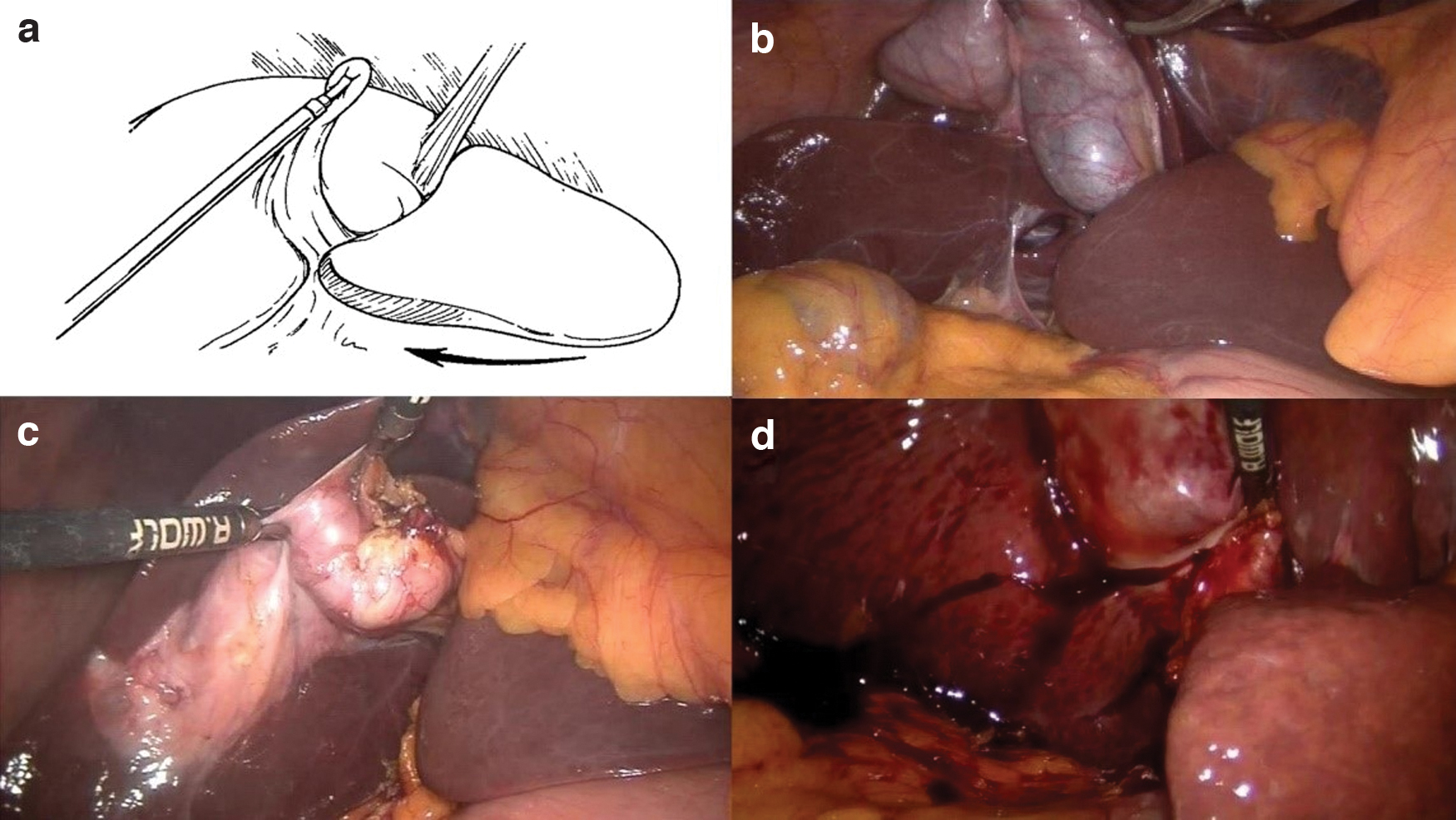
In the multivariate analysis performed in our study, three important parameters that required the use of additional ports during the three-port LC were determined. These were hepatic barrier (P < .001), female gender (P < .001), and complete adhesion in the gallbladder (P < .001). Literature information regarding the use of additional ports due to liver barrier during three-port LC is very limited and detailed comparison could not be made. Çiftçi et al. reported that liver barrier due to segment IV hypertrophy that coexist with gallbladder adhesion caused additional trocar use. 20 In his evaluation, Halpern reported that the dissection of the Calot triangle in the LC was difficult as a result of hypertrophy and ptosis of the liver left lobe (Fig. 3a). 30 In our study, 15 patients (6.41%) had hepatic barrier that made hilum dissection difficult, and an additional fourth port was required in 13 of these patients (86.66%) (Fig. 3b–d). There are studies showing an increased risk of conversion to OC during four-port LC in female patients, as well as studies showing the opposite.11,26–28 We could not find any information about the literature to compare this result from our study and similar results to compare. Although Tagaya et al. reported that they used additional ports due to adhesion in 5 patients (4.8%) in their study, they did not specify the total adhesion rates. 19 In meta-analysis studies on three-port LC, it has been stated that adhesion requires the use of additional ports. 11 In 55 cases, there was complete adhesion of the gallbladder during LC, and it was seen in 32 patients (16.67%) in the first group and in 23 patients (54.76%) in the second group, which significantly increased the use of additional ports (Fig. 4).
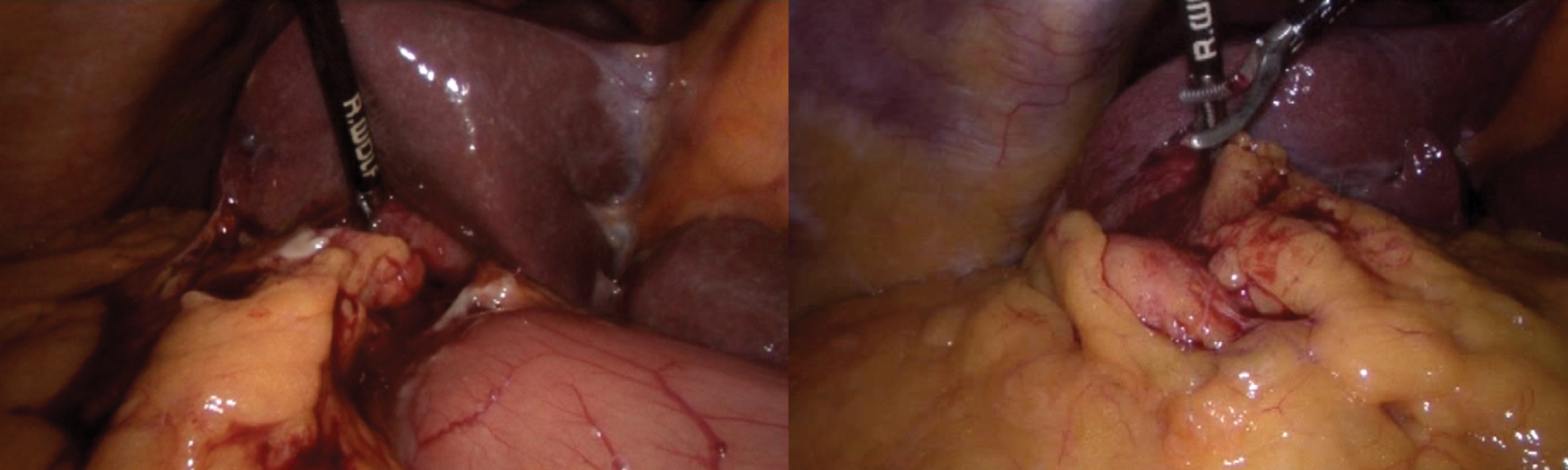
Complete gallbladder adhesion seen in our cases where additional ports were used. Color images are available online.
Although the data were recorded prospectively, the fact that the analyzes were performed retrospectively on video recordings in this study may have created a mistake in determining the objective criterion of the fourth port requirement. In addition, since there is no generally accepted international rating of gallbladder adhesion and liver-related barriers, the different identifiability of these factors from surgeon to surgeon is among the limitations of the study. For this reason, conducting multicenter studies instead of a single center, which is the other deficiency of our study, will help to determine more objective parameters.
Conclusions
As a result, the three-port LC can be done safely, but sometimes additional ports are required to avoid injuries and safe dissection. Although many factors require the use of additional ports during three-port LC, the use of an additional fourth port should not be avoided in patients with full adhesion in the gallbladder, liver-induced barrier that makes dissection difficult, and in female cases.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.