
Abstract
Background:
After the first laparoscopic Roux-en-Y gastric bypass (RYGB) in 1994 by Wittgrove, the introduction of robot-assisted procedures was the next step in the surgical race to reduce invasiveness. This breakthrough allowed us to perform bariatric surgery with less surgical trauma in obese patients with metabolic disorders, producing an exponential increase in procedures performed.
Methods:
This is a retrospective cohort study of a prospective database for patients who underwent RYGB during a 7-year period through two different approaches, laparoscopic and robotic. The robotic cases were performed by two generations of the da Vinci platform (S and Xi), and three groups were identified and compared (L-RYGB, RYGB-S, and RYGB-Xi).
Results:
A total of 495 patients underwent RYGB, of which 224 by laparoscopy (45.2%) and 271 by robotic approach (54.7%): 134 RYGB-S and 137 RYGB-Xi. The majority of the patients (71.1%) were females, with a mean age of 46.2 years and a mean body mass index of 44 kg/m2. The mean intraoperative time and intraoperative complication rate were higher in the robotic groups, especially in the RYGB-S group. Postoperative complications were higher in the same group, with a rate of 11.9%, where the main leakage occurred on the upper part of the gastric pouch and not in the hand-sewed robotic anastomosis (7.5%). General mortality was 0.6%. We found no significant differences at 1-year percentage of total weight loss (%TWL); at 2 years, the RYGB-Xi group had the lowest %TWL (25.24 ± 14.54, P ≤ .001).
Conclusions:
The present study reflects our experience during the robotic bariatric introduction and performance since 2011. Features of the da Vinci S platform along our learning curve may explain a higher complication rate. The patients who have been operated by the RYGB-Xi system had lower complications than the laparoscopic group. The robotic approach did not differ with laparoscopy in terms of weight loss and chronic complications after 24 months of follow-up.
Introduction
Bariatric surgery has evolved since Professor Mason performed the first open case of gastric bypass in 1967. 1 Even though several advances have been added for the obesity treatment such as medications, endoscopy, and surgical procedures, bariatric surgery remains being the most effective treatment for obesity and related comorbidities. The main procedures are Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy (SG), and biliopancreatic diversion with duodenal switch, among others. Despite those procedures, RYGB has been the crown jewel procedure in the bariatric field for the past 40 years, with low rate of complications and predictable results.
Wittgrove et al. performed the first RYGB by the laparoscopic approach in 1994 and brought obesity surgery the concept of minimally invasiveness, which allowed to perform procedures with less surgical trauma and inflammatory response. 2 Unfortunately, in the beginning, it was limited by instrument, equipment, and technical skill barriers. During the past 20 years, laparoscopy has been used around the world and is now considered the standard approach for bariatric surgery. A new era began in bariatric surgery when Horgan and Vanuno started to use the da Vinci™ system, a robotic platform, in 34 advanced laparoscopic procedures. Among them, 7 patients underwent robot-assisted (RA)-RYGB for morbid obesity. He published his casuistic in 2001. 3
The da Vinci system produced by Intuitive Surgical® (Sunnyvale, CA, USA) reached the Food and Drug Administration approval in 2000. 4 The first generation was limited and had only three arms, and 6 years later, it released the second generation named da Vinci S, which had a fourth hinged arm and better accuracy of operating gestures. Other generations were released in 2009 (da Vinci Si) and in 2014 (da Vinci X). The latest version corresponds to the fourth generation and present significant improvements.
The robotic system improves surgeons' ergonomy due to a comfortable position in the console rather standing next to the operating table. As an innovative technology, it awoke the desire and interest of surgeons for the robotic system; even though it presented a high cost for implementation and maintenance, many hospitals around the world bet on the technique and acquired robotic platform and started a program of bariatric surgery.
The first publications reflected higher rates of complications, reoperation, and longer operative time in RA-RYGB compared with laparoscopic RYGB (L-RYGB).5,6 Otherwise, recent systematic reviews and meta-analysis compared clinical outcomes and demonstrated good results, especially in the complications and hospital stay, favoring robotic surgery.7–10 The aim of this study was to compare the short- and long-term outcomes of RA-RYGB of two distinct generations (S and Xi) with L-RYGB.
Materials and Methods
Patients and selection of groups
After institutional review board approval, a retrospective cohort study was made for a prospective database from January 2011 to June 2018. As a public health system hospital, the Unit of Bariatric and Metabolic Surgery has L-RYGB as the main surgical technique, and the robotic platform become available in the last years. Patients with previous abdominal surgery were rejected for robotic procedures. This study represents a chronological series of the robotic gastric bypass between two generations (S and Xi), which was compared with the standard L-RYGB. Three different groups have been identified over that timeline: standard L-RYGB cases (from 2011 to 2018), RA-RYGB-S cases (from 2011 to 2015), and RA-RYGB-Xi cases (from 2016 to 2018). Demographic variables included were age, gender, preoperative body mass index (BMI), main obesity-related comorbidities (diabetes, hypertension, dyslipidemia, obstructive sleep apnea, and/or continuous positive airway pressure), alcohol consumption, and smoking.
Preoperative
All patients have had a multidisciplinary team evaluation and have followed an obesity surgery protocol for bariatric and metabolic surgery, which is based on Criteria for Bariatric Surgery of the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). Patients who were eligible candidates for bariatric surgery signed the informed consent with careful communication along with family members. All patients underwent a thromboprophylaxis protocol with intermittent compression socks on the trans and immediate postoperative time associated with low-molecular-weight heparin during 4 weeks.
Laparoscopic surgical technique
The traditional L-RYGB technique performed under a 34F bougie was used for gastrojejunostomy (GJ) anastomosis. Patients were positioned in the supine position with a 20° Fowler and open legs, wrapped by pneumatic leg sleeves. In a standardized manner, five ports (one trocar of 11 mm, two trocars of 12 mm, and two trocars of 5 mm) were used. Afterward, a 15–30 mL gastric pouch was created with a 60 mm Echelon Flex™ Endopath® linear stapler (Ethicon Endo-Surgery, Inc., Cincinnati, OH, USA). A completing reinforcement of the pouch was performed by hand-sewn, continuous absorbable suture. GJ was performed by Echelon Flex, a linear stapler with a white cartridge, stapling the anastomosis at 2.5–3 cm, considering a biliopancreatic limb of 100 cm length. The Roux limb was brought to the gastric pouch in an antegastric–antecolic position. Mechanical lineal jejunojejunostomy was completed with an application of a 60 mm Echelon Flex linear stapler with a white cartridge, which created an alimentary limb (Roux) with 130 cm of length. The mesenteric defect and the Petersen space were closed with a running nonabsorbable suture. The Petersen space closure started to be systematical part of the procedure in 2016.
Robotic surgical technique
The patient positioned in the supine 30° Fowler position with closed legs and six ports as a conventional technique where four 8 mm trocars were used (four arms) and associated with one 12 mm and one 5 mm trocar. A liver retractor was placed in the epigastrium. A single-docking manner was used during the entire procedure. Access started in the lesser omentum creating a retrogastric window, a small gastric pouch of 15–30 mL was made using endoscopic (non-robotic) 60 mm Echelon Flex with a calibrating device. The model of stapler used from 2011 to 2016 was the ATS45® (Articulating Linear Cutter), which had a length of 34 cm. After 2016, the Echelon Flex long (44 cm length) was used in all robotic cases. A complete reinforcement of the vertical part of the pouch including the stapling line was carried out using polydioxanone (PDS 3-0). A 2 cm gastrostomy and enterostomy were created with a harmonic robotic scissor device. Hand-sewn two-layer antecolic–antegastric GJ was performed with polyglactin 3-0 and PDS 3-0. The jejunojejunostomy was created with an Echelon Flex linear stapler. The length of the Roux limb and biliopancreatic limb was the same in the L-RYGB. For all the groups, a standard endoscopic staples device was used. The technical steps performed for RA-RYGB were identical on both the generations of the da Vinci system (S and Xi). The mesenteric defect was closed in both robotic groups, despite that the Petersen space only was closed routinely in the RA-RYGB-Xi group. Finally, an intraoperative methylene blue test was performed at the end of the surgical procedure as a leak test.
Thirty days of outcome
Variables analyzed were operating room time (ORT), intraoperative complications (including blue test, bleeding, and other complications), and length of hospital stay (LHS). The postoperative 30-day morbidity with surgical complications (return to the operating room) and main nonsurgical complications (deep venous thrombosis, pulmonary embolism, pneumonia, wound infection/seroma, urinary tract infection, and gastrointestinal bleeding) and mortality rate were recorded. The ORT was defined as the time from the first skin incision to the closure of the last incision. The complications were graded according to the Clavien–Dindo classification and divided into minor complications (I, II, and IIIa) and major complications (Grade IIIb and IV). 11
Follow-up period
The main variables analyze follow-up in months, BMI after the RYGB at 3, 6, 12, and 24 months, and weight loss, which are expressed in variation of BMI (ΔBMI) and percentage of total weight loss (%TWL) at 1 and 2 years. The rate of complication per group and main types, as well as reoperation and weight regain, were described.
Statistical analysis
The results of parametric and nonparametric data are expressed as mean and standard deviation and median (range), respectively. Statistical analysis was performed using the IBM® SPSS® Statistics Software version 24.0. Confidence intervals were set at 95%. A two-sided P value ≤.05 was considered statistically significant. Comparisons between the three groups were carried out with Fisher's exact test for discrete variables. Other tests used were Pearson's chi-squared test for nonparametric variables and one-way analysis of variance (ANOVA) test to compare three or more groups. When the ANOVA test presented statistical significance, the post-hoc analysis, Bonferroni comparison, was used. The study received the IRB approval.
Results
Between January 2011 and December 2018, a total of 495 patients underwent gastric bypass: 224 by L-RYGB (45.2%) and 271 by RA-RYGB (54.7%). On the robotic group, 134 patients underwent RA-RYGB-S and 137 underwent RA-RYGB-Xi technology. Patients' demographic data are summarized in Table 1. The majority of the patients (71.1%) were females, with a mean age of 46.2 years and a mean BMI of 44 kg/m2. The three groups were comparable without any demographic data differences among them with statistical significance. The exception was diabetes that presented difference between the L-RYGB and RA-RYGB-Xi groups (30.8% and 48.9%, respectively; P < .001). Twenty five percent of the patients in each group had a history of smoking.
Demographic Data of the Population with Laparoscopic and Robotic Roux-en-Y Gastric Bypass
BMI, body mass index; CPAP, continuous positive airway pressure; L-RYGB, laparoscopic RYGB; OSA, obstructive sleep apnea; RA-RYGB, robot-assisted RYGB; RYGB, Roux-en-Y gastric bypass; S and Xi, generations of the da Vinci system.
The follow-up period for patients was 39.1 ± 25 months in the L-RYGB group and 41.1 ± 36 and 9.1 ± 8 months in the RA-RYGB-S and RA-RYGB-Xi groups, respectively (P ≤ .001). Overall morbidity was higher in the RA-RYGB-S group compared with the two other groups (11.9% versus 4% and 2.9%, respectively; P = .002). The RA-RYGB-S group had higher major intraoperative complications compared with the two other groups (11.9% versus 2.2% and 2.2%, respectively; P < .001). Minor complications were similar in all the groups (Table 2). Complications were more common in the L-RYGB and RA-RYGB-S groups, with a rate of 10.7% and 13.4%, respectively, against 2.2% on the RA-RYGB-Xi group (Fig. 1). Regarding chronic complications, the most prevalence was hypoglycemia and it occurred on the L-RYGB (13 cases), followed by RA-RYGB-S (4 cases). No cases of hypoglycemia were identified on RA-RYGB-Xi. Anastomotic strictures did not present differences among the groups. These cases and some other related to chronic pain and weight regain treatment such as bypass distalization have been included in the reoperative procedures in the long-term follow-up. The number of complications and types are described in Figure 2. During the second period, an increase in postoperative complications, 1–4 cases for every 50 cases period, was noticed in the robotic group (Fig. 2A refers to the robotic group), and in the laparoscopic group, the overall complication rates got stable after 60 cases (Fig. 2B refers to the laparoscopic group).
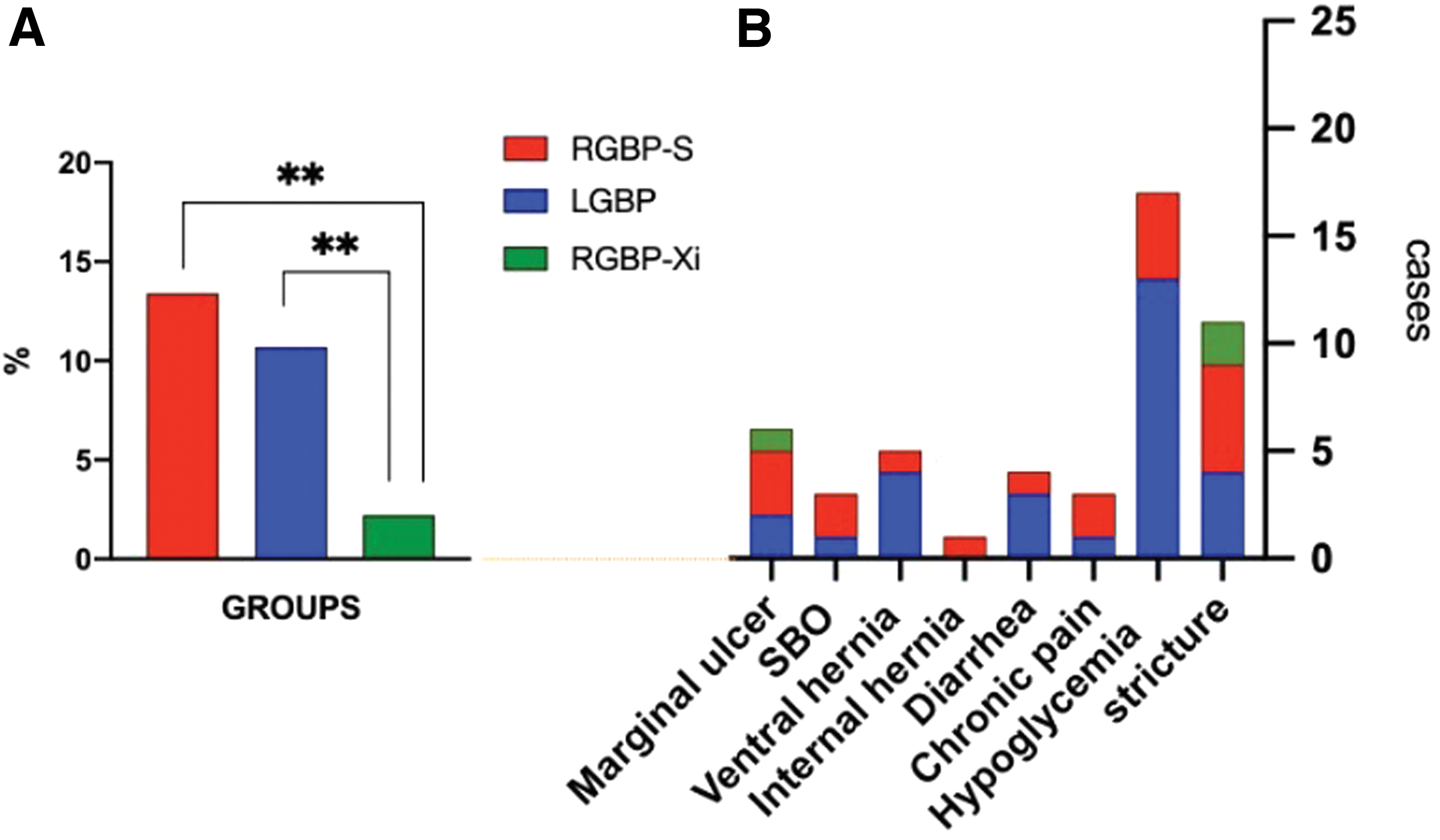
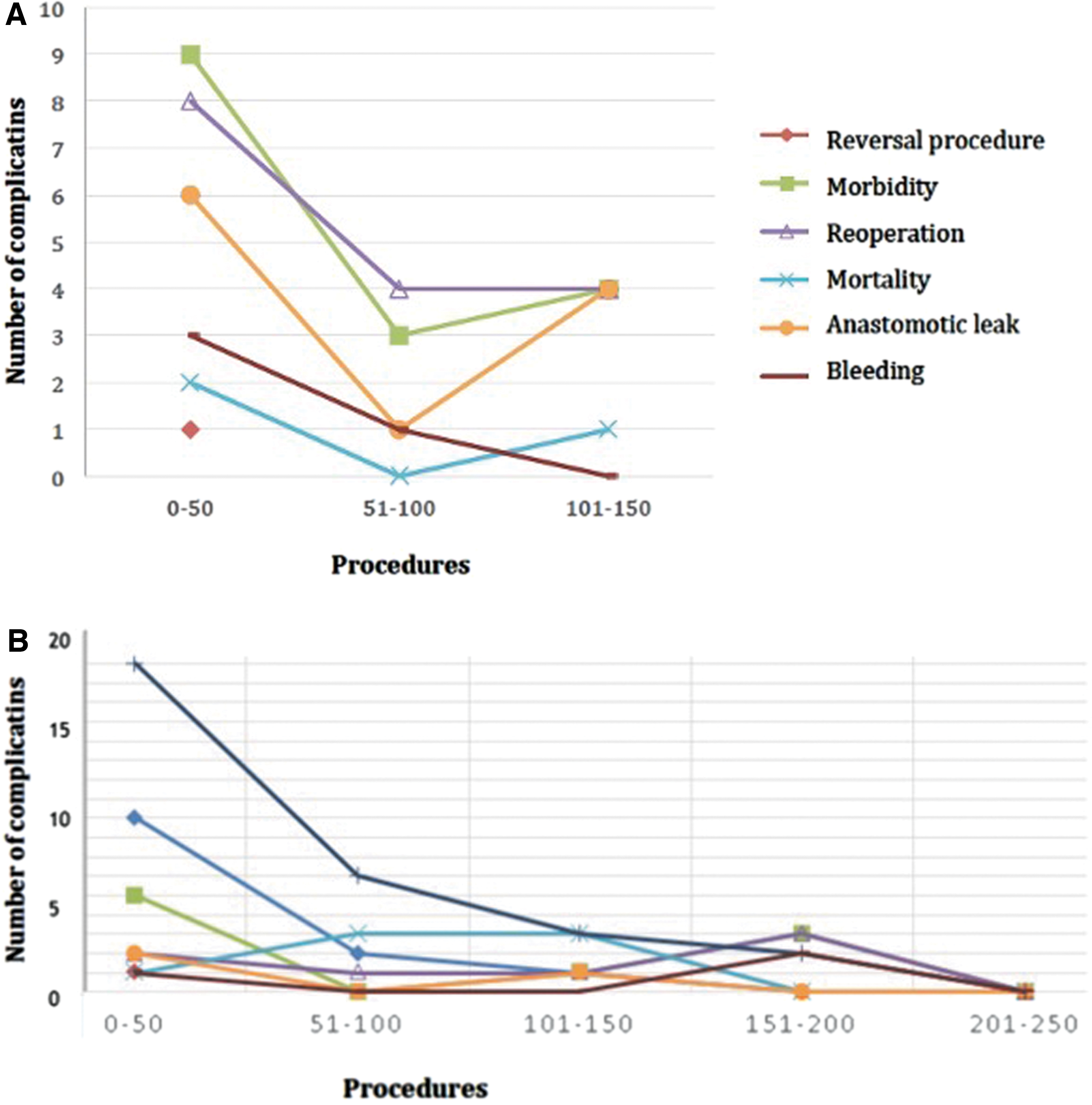
Overview of RYGB complications plotted along the number of performed procedures.
Thirty Days of Postoperative Outcomes in Patients with Laparoscopic and Robotic Roux-en-Y Gastric Bypass
Clavien–Dindo classification for surgical complications.
L-RYGB, laparoscopic RYGB; ns, no significance; RA-RYGB, robot-assisted RYGB; RYGB, Roux-en-Y gastric bypass; S and Xi, generations of the da Vinci system.
The follow-up data of ΔBMI and %TWL on the first and second year are summarized in Table 3. Reoperation and weight regain were significantly lower in the RA-RYGB-Xi group than in other groups (P = .005 and .008, respectively). BMI evolution during the follow-up did not present differences between the time of surgery (operative BMI) and at 24 months. However, RA-RYGB-Xi had a weight regain more noticeable despite without statistical significance (Fig. 3). As ΔBMI in the first year, RA-RYGB-Xi had the highest mean of BMI change (16 points) against L-RYGB that had the lowest change of BMI (P < .001). No differences were detected between ΔBMI of RA-RYGB-S and other groups in the first year and among all the groups in the second year. In contrast, %TWL in the first year for RA-RYGB-Xi was higher than others even though it decreased sharply in the second year when it presented the lowest %TWL among the groups (Fig. 4).
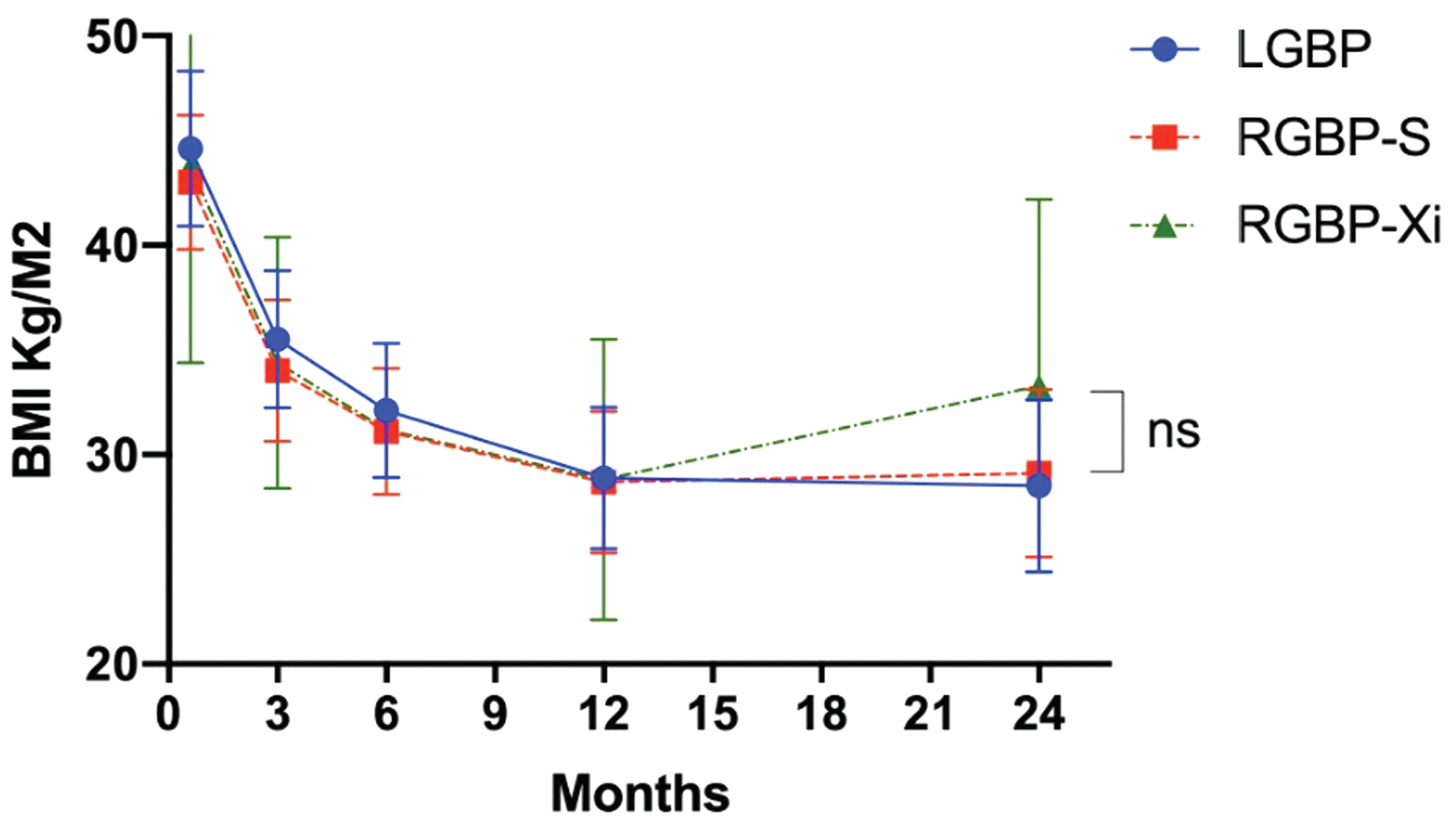
General view of weight loss among the groups during the follow-up period between 0 and 24 months. ns, no significance. Color images are available online.
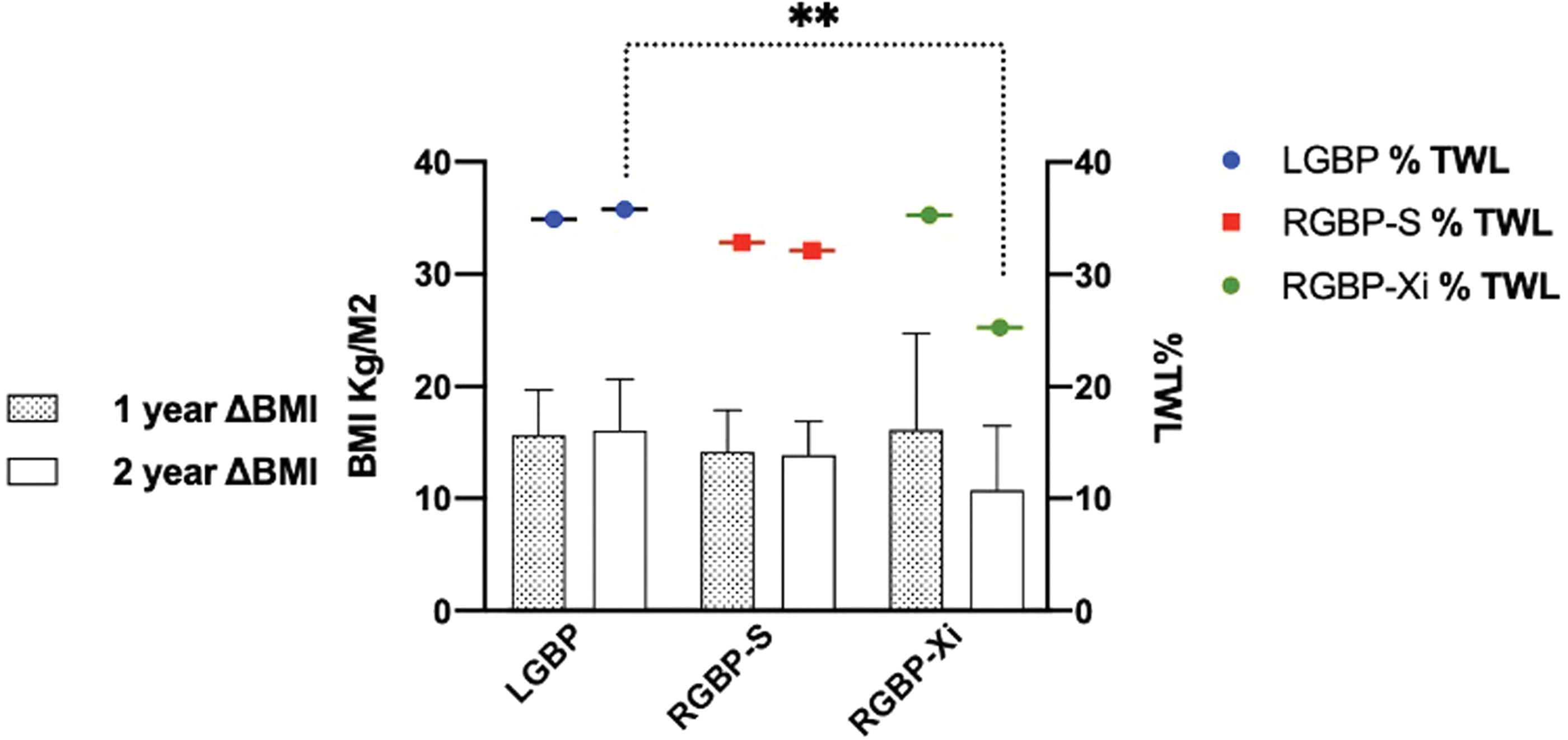
ΔBMI at 1 and 2 years among the groups (bar graphics) associated with %TWL at 1 and 2 years (scatter dot plot colorful). ** P = .001. ΔBMI, variation of body mass index; %TWL, percentage of total weight loss. Color images are available online.
Weight Loss During the Follow-up Period According to the Laparoscopic and Robotic Groups with Roux-en-Y Gastric Bypass
ΔBMI, variation of body mass index; %TWL, percentage of total weight loss; L-RYGB, laparoscopic RYGB; RA-RYGB, robot-assisted RYGB; RYGB, Roux-en-Y gastric bypass; S and Xi, generations of the da Vinci system.
Discussion
Bariatric procedures represent a challenge for many reasons, mainly due to anthropometrical characteristics of patients and the complexity of procedures. The robotic platform can help surgeons to perform procedures and present similar results found for L-RYGB. The Consensus statement promoted by the EAES on the use of robotics in general surgery stated that Robot-assisted bariatric surgery presents comparable clinical outcomes with standard laparoscopic surgery. 10
We present our initial experience as the Unit of Bariatric and Metabolic Surgery with the robotic program for gastric bypass. The learning curve and limitations of the platform used at that time (the da Vinci S system) were the main points that led to an unfortunate result among the RA-RYGB groups. The robotic program started in 2011 with robotic SG (more than 100 cases) before moving to more complicated procedures such as RA-RYGB. 10 For those patients, no different criteria were used to select a patient for a robotic or laparoscopic approach, although demographic data were similar in all the groups.
The longest LHS was found in the RA-RYGB-S group (4.3 ± 11 days), although it did not present statistical significance. It reflects the higher rate of major complications of this group (11.9%), which increased the average of LHS.
For the 30 days of outcomes, a higher rate of complication was identified, with reintervention incidence of 11% in the RA-YGB-S group versus only 2.2% in the RA-RYGB-Xi and L-RYGB groups (P = .001). Bleeding and perforation were higher in RA-RYGB-S as intraoperative complications, but they did not reach statistical significance. Three reasons can be listed to explain the higher rate of “da Vinci S platform” complications: the learning curve for robotic gastric bypass procedures, injuries produced by the da Vinci instrument (forceps), and inadequate maneuver during of stapler application on the upper part of the gastric pouch, including reinforcement of the pouch.
The gastrojejunal anastomosis was performed in hand-sewn manner, which presents a higher level of difficulty and needs a longer personal learning curve. In the literature, the learning curve for RA-RYGB is around 10–15 procedures.11,12
We believe that the number of procedures can vary among surgeons because of personal skills and interest in the robotic approach. Overall, surgeons with excellent laparoscopic skills have less appealing to robotic procedures due to a longer operative time than laparoscopic procedures. However, the robotic learning curve for RYGB is shorter than that for L-RYGB. 13 We analyzed surgical results (4 surgeons) and found that a learning curve for RYGB equals 15 procedures, and complications decreased drastically, especially acute complications, after an amount of 60 cases of RA-RYGB performed on the service. The analysis of L-RYGB showed a decrease in 30 days of complications after 100 procedures (25 procedures by the surgeon). During the second period, an increase in postoperative complications, 1–4 cases for every 50 cases period, was noticed and due to a new member learning curve and variability in the working teams.
Additionally, some injuries occurred on the small bowel on the same group (RA-RYGB-S), and we believe that injuries arise due to double-fenestrated grasper used on that robotic platform “S,” which presented unsuitable features and did not allow careful management of small bowels. It is quite right that in other generations (DV-Si and Xi), this double-fenestrated grasper was replaced by Tip-Up fenestrated grasp that presents suitable features for small bowel manipulation.
Likewise, atypical leaks occurred in RA-RYGB-S on the upper part of the pouch, and it can be explained by the model of stapler used from 2011 to 2016, named ATS45 (Articulating Linear Cutter), which had a length of 34 cm. The assistant surgeon fired staplers from the right side of the patient to perform the gastric pouch, and it was a tricky maneuver, especially the last two fires of the pouch (Hiss angle) because of the length of that stapler (34 cm). All the staples were placed from the right side of the patient, and the longest distance between the abdominal wall and the upper part of the pouch was sometimes too long for the length of the stapler (especially in high patients). That situation was solved with the long stapler, which allowed us to perform the last stapling with tractions. The previous technical aspects could explain the rate of pouch leaks at the level of Hiss angle (9 cases of the RA-RYGB-S group), which is an uncommon site for gastric bypass leakage, and in 2016, only endoscopic staplers with a length of 45 mm had been used. Another issue encountered in the learning process with the robotic technology was the pouch reinforcement, which allowed non-sensitive tractions of the pouch to do the vertical reinforcement and adding trauma and ischemia to the tissue and pouch. This would lead to inadvertent postoperative complications in some cases.
When we consider only RA-RYGB-Xi cases (after 134 cases performed), the rate of the leak was 2.2%, and it is similar to that found in the literature (between 0.2% and 2.13%).14,15 Otherwise, a matched cohort study compared RA-RYGB with L-RYGB and revealed a significant reduction of anastomotic leaks of the robotic approach (0.5%) against the laparoscopic approach (0.9%).16,17
Different follow-up periods were identified among the groups, and L-RYGB/RA-RYGB-S had an average of follow-up period of more than 5 years, but RA-RYGB-Xi had a shorter follow-up (9.1 ± 8 months). It should reflect on the frequency of registered complications in the RYGB-Xi group, first, the overall morbidity, all types of complications rates were in the RA-RYGB-S group compared with the other two groups. However, these are acceptable rates of complications. In a systematic review, Fourman and Saber identified the same standard of complications on RA-RYGB and L-RYGB (from 0% to 20%) and did not differ from the results found in this study. 13 Second, RA-RYGB-Xi presented a lower rate of complications (2%), and we consider that this percentage is low due to a shorter period of follow-up of this group, and it probably will have similar results of other groups when it reaches a long-term follow-up (>5 years). The same explanation can justify the lower rate of reoperation and weight regain presented on that follow-up period in the RA-RYGB-Xi group. Some long-term complications of the patients in the Xi group are still not reported because of the shorter follow-up period of the patients.
The main chronic complication observed in this study was hypoglycemia, and it was more found in the L-RYGB group. It corresponds to a considerable percentage of patients after gastric bypass (5.8%), and it is understood as complication until now, it has been investigated in our service together with the endocrinologist team, sure it will be an issue for future publications.
At the beginning of our experience, cases of RA-RYGB corresponded 30% of the gastric bypass, but when the robotic system was replaced by the da Vinci Xi system (2016), the number of RA-RYGB procedures were increasing when surgeons gained confidence with this new platform. Although the inadequate result obtained at the beginning of our robotic program with generation S and additional good results of L-RYGB (a considerable number of cases performed throughout the period), an opposite situation has been found in our service. The laparoscopic approach corresponds to only 30% of gastric bypass cases against robotic procedures, which resulted for 70% of gastric bypass since 2018. This phenomenon has also occurred on other services and has been reported. 18 We believe that robotic will continue to be a good option for bariatric surgery in our unit due to the improvement of that technology with “da Vinci Xi platform” and our experience gained during the past 10 years in the robotic program for bariatric surgery. 19 Additionally, future data of comparison RA-RYGB with L-RYGB, without considering the learning curve for robotic procedures and generation S, can bring good results with an acceptable frequency of complications on 30 days and follow-up period. 20
The study limitation relies on the retrospective character, use of different robotic generations for same approach, which decreases the strength when they are compared with the standard laparoscopic approach and the heterogeneity of the result in the robotic generations that make difficult to extrapolate robotic results. Also, there are only 2-year data on the RA-RYGB-Xi patients' follow-up at the time of the data analysis and could give some limitation when discussing mid-term follow-up. Also, the changing habits introduce an enhanced recovery program for bariatric surgery during the study period and including surgeons' learning curve could bias some of the overall results.
Conclusions
In this study, the L-RYGB group presented the most comparable results, which are similar to the medical literature with an acceptable rate of complications and adequate weight loss (ΔBMI and %TWL). Comparison between L-RYGB and two different generations of the da Vinci system (S and Xi), through 7 years of study, showed that da Vinci S presented unsuitable results due to some reasons related to instrument features and robotic learning curve, which led to the highest major complication rate at 30 days. However, in the follow-up period, RA-RYGB-S presented similar results in weight loss and compared complications rate with L-RYGB. Conversely, the RA-RYGB-Xi group showed the lowest complication rate on 30 days of outcomes and follow-up period for most of the variables analyzed; however, the follow-up of this group was considered short and can lead to an underestimation of RA-RYGB-Xi findings (mainly complications, reoperation, and weight regain rate).
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.