
Abstract
Background:
Laparoscopic Kasai portoenterostomy (KPE) is generally considered to be technically challenging. A scarcity of studies has particularly focused on the learning curve (LC) of this technique. The present study was aimed to objectively evaluate the LC of laparoscopic KPE in a medical center with relatively low caseload of biliary atresia (BA).
Materials and Methods:
Thirty-five consecutive pediatric patients treated with laparoscopic KPE for BA by the same surgeon team between 2012 and 2018 were retrospectively enrolled in the present study. Operative time (OT) was selected as the surrogate marker. Cumulative sum (CUSUM) analysis was applied to describe the LC of laparoscopic KPE.
Results:
The turning point of the CUSUM curve occurred at the 21st case, which divided the curve into two distinct phases, phase 1 (the initial 21 cases) and phase 2 (the remaining 14 cases). The curve was best modeled as a second-order polynomial with equation CUSUM in minutes equal to −0.9161 × case number2 + 32.097 × case number + 7.8217 (R2 = 0.981). Age at surgery, sex, weight, and preoperative liver function were well balanced between the two phases (each P > .05). The OT was significantly decreased in phase 2 compared with phase 1 (P < .0001). Furthermore, the rates of early jaundice clearance and 2-year native liver survival were higher in phase 2. The rate of postoperative cholangitis was comparable between the two phases.
Conclusions:
Two characteristic phases of the LC for laparoscopic KPE were identified using CUSUM analysis and represented the initial learning period and the subsequent period of technical mastery, respectively. Surgeons are possible to acquire competency of laparoscopic KPE in relatively low-case centers.
Introduction
Biliary atresia (BA) is a rare but severe congenital anomaly. Epidemiological data show that the incidence of BA is around 1/5000 to 1/19,000 live births worldwide. 1 The pathology of BA is characterized by progressive inflammatory and fibrotic obliteration of intra- and extrahepatic bile ducts. 2 Without prompt treatment, the majority of affected children could eventually proceeded to fatal outcomes with end-stage liver disease.1,2
Kasai portoenterostomy (KPE) is generally recognized as the mainstay of therapy for BA 3 and aimed to achieve sufficient bile drainage, preserve the function of native liver as early as possible, and postpone or minimize requirement for liver transplantation. 4 Although the rapid development of laparoscopic equipment greatly promotes the popularity of minimal invasive techniques, laparoscopic KPE has not been widely accepted by surgeons.
In 2002, Esteves et al. 5 first reported their successful experience on laparoscopic KPE. However, a number of studies subsequently yielded conflicting conclusions on the superiority and inferiority between laparoscopic versus open KPE. Some experts ever founded that laparoscopic KPE had more advantages than open KPE and was more beneficial for future liver transplantation because of less postoperative adhesion.3,6,7 Whereas some experts reported that prognosis was not better, or even worse after laparoscopic KPE compared with open approach.4,8–10
Lishuang et al. 11 conducted a meta-analysis to compare clinical outcomes after laparoscopic versus open KPE with 11 comparative studies enrolled. They found that the rate of 2-year native liver survival (NLS) was lower after laparoscopic KPE and thus proposed that laparoscopic KPE could not replace open KPE. Considering lack of sufficient randomized cohort studies and marked heterogeneity among the studies enrolled in this meta-analysis, we think that caution is required in making definitive conclusions on the advantages and disadvantages of laparoscopic KPE.
As well known, KPE demands high level of technical precision and dexterity for surgeons. Compared with conditional laparotomy, surgeons lack stereoscopic vision, and spatial orientation could be impaired with utilization of two-dimensional image vision. High level of hand–eye coordination and excellent team cooperation between surgeons are always required during laparoscopic procedures. These limitations of laparoscopy could pose considerable challenges to surgeons and may extend the learning process of laparoscopic procedures, especially those technically demanding surgical maneuvers. 12
Because of the low incidence of BA and technical difficulty of laparoscopic KPE, it may take a long time for a surgeon to acquire technical competency. 4 Some experts ever anticipated that the learning curve (LC) of laparoscopic KPE was a possible reason for the unsatisfactory postoperative outcomes.4,8,9,11,13 Nevertheless, there is a scarcity of researches objectively evaluating the LC of this challenging technique, particularly regarding on performance of surgeons in low-caseload medical centers. The present study was designed to quantify the LC of laparoscopic KPE and to describe the correlation between learning process and patient prognosis using cumulative sum (CUSUM) analysis. Our findings may assist surgeons obtain more useful information and improve their insight on laparoscopic KPE.
Patients and Methods
Study design
The present study retrospectively enrolled 35 consecutive children who were diagnosed with BA and underwent laparoscopic KPE performed by the same team at Huai'an Women and Children's Hospital (Jiangsu, China) from 2012 to 2018. Children were excluded if they were treated with open KPE operation. This study was approved by the institutional review board of Huai'an Women and Children's Hospital and conducted in compliance with the principles of Declaration of Helsinki. Before surgical therapy, written informed consent was obtained from patients or legal guardians of each child.
Baseline characteristics, intraoperative, and postoperative data of all children enrolled were retrospectively reviewed through searching medical database. Preoperative liver function included total bilirubin (TBIL), direct bilirubin (DBIL), alanine aminotransferase (ALT), aspartate aminotransferase (AST), and gamma-glutamyl transferase (GGT). Intraoperative parameters included date of surgery, operative time (OT), and estimated blood loss (EBL). Postoperative parameters included early clearance of jaundice, the occurrence of cholangitis, the length of follow-up, survival status, and the rate of 2-year NLS. The OT was calculated as the time duration from the skin incision to the final closure. The early clearance of jaundice was defined as the TBIL level <20 μmol/L within 6 months after laparoscopic KPE.
Surgical procedures
A previous study has described the major surgical strategies of laparoscopic KPE in the medical center of the present study. 14 In brief, first, a percutaneous suture was introduced below the xiphoid process to snare the round ligament and retract the liver. Then, the gallbladder was mobilized, and a percutaneous suture was introduced to the remnant of the fundus to further expose the porta hepatis. The gallbladder and the distal biliary remnant were dissected; the fibrous remnant of the common bile duct was isolated and ligated at the superior margin of the duodenum. The right and left hepatic arteries and portal veins were isolated, and then, two elastic rubber bands were placed, respectively, around the two branches of portal veins and the hepatic artery for better exposure of the porta hepatis. The portal fibrous cord was meticulously dissected and transected with laparoscopic scissors.
Bleeding was controlled through direct pressure, and electrocautery was avoided because of its thermal damage on the liver surface.
After the identification of the ligament of Treitz and the proximal jejunum, pneumoperitoneum was released, and a Roux-en-Y jejunal loop was created extracorporeally. Then, pneumoperitoneum was re-established, and the jejunal loop was sutured to the hilum continuously. The peritoneal cavity was routinely explored to ensure no active bleeding.
Statistical analyses
The CUSUM analysis is widely used in quantifying the LC of various surgical procedures.15,16 All cases enrolled were ordered chronologically, from the earliest to the latest surgery date. The OT was selected as the learning index to formulate the performance-based CUSUM chart. The CUSUM value for the first case was the difference between the OT for the first case and the average OT for all cases. The CUSUM value for the second case was the CUSUM value for the previous case plus the difference between the OT for this case and the average OT for all cases. This recursive process continued until the CUSUM value for the last case was calculated as zero. In the CUSUM chart, the slope of the curve is >0 if the OT value for a case is more than the overall average, and <0 if the OT value for a case is less than the overall average.
All statistical analyses were conducted using STATA version 12.0 Software. Categorical data are expressed as numbers and percentages (%). Continuous data are expressed as mean ± standard deviation (SD), or median with range. For comparison between phases identified by CUSUM analysis, the Fisher's exact test was used for categorical data; the unpaired t-test or the Mann–Whitney test was used for continuous data as appropriate. Statistical difference was considered to be significant if a two-tailed P value was <.05.
Results
Patients
Table 1 summarizes baseline characteristics, intraoperative, and postoperative parameters of all children enrolled in the present study. For the entire cohort, the average OT was 226.3 ± 22.4 minutes. The rates of early clearance of jaundice and cholangitis were 68.6% and 52.6%, respectively. One case was lost to follow-up at the second year after Kasai operation and was thus excluded for statistical analysis of the rate of 2-year NLS. Overall, the rate of 2-year NLS was 70.6% for this case series.
Pre-, Intra-, and Postoperative Parameters of All Children Enrolled
One case was lost to follow-up within 2 years after Kasai operation.
Within 2 years after Kasai operation
ALT, alanine aminotransferase; AST, aspartate aminotransferase; DBIL, direct bilirubin; EBL, estimated blood loss; GGT, gamma-glutamyl transferase; NLS, native liver survival; OT, operative time; TBIL, total bilirubin.
Learning curve
Figure 1 demonstrates the LC of laparoscopic KPE obtained by plotting CUSUM values for the OT chronologically against case number. The CUSUM learning curve was best modeled as the equation: CUSUM (minutes) = −0.9161 × case number 2 + 32.097 × case number + 7.8217. This equation had a high R2 value of 0.981.
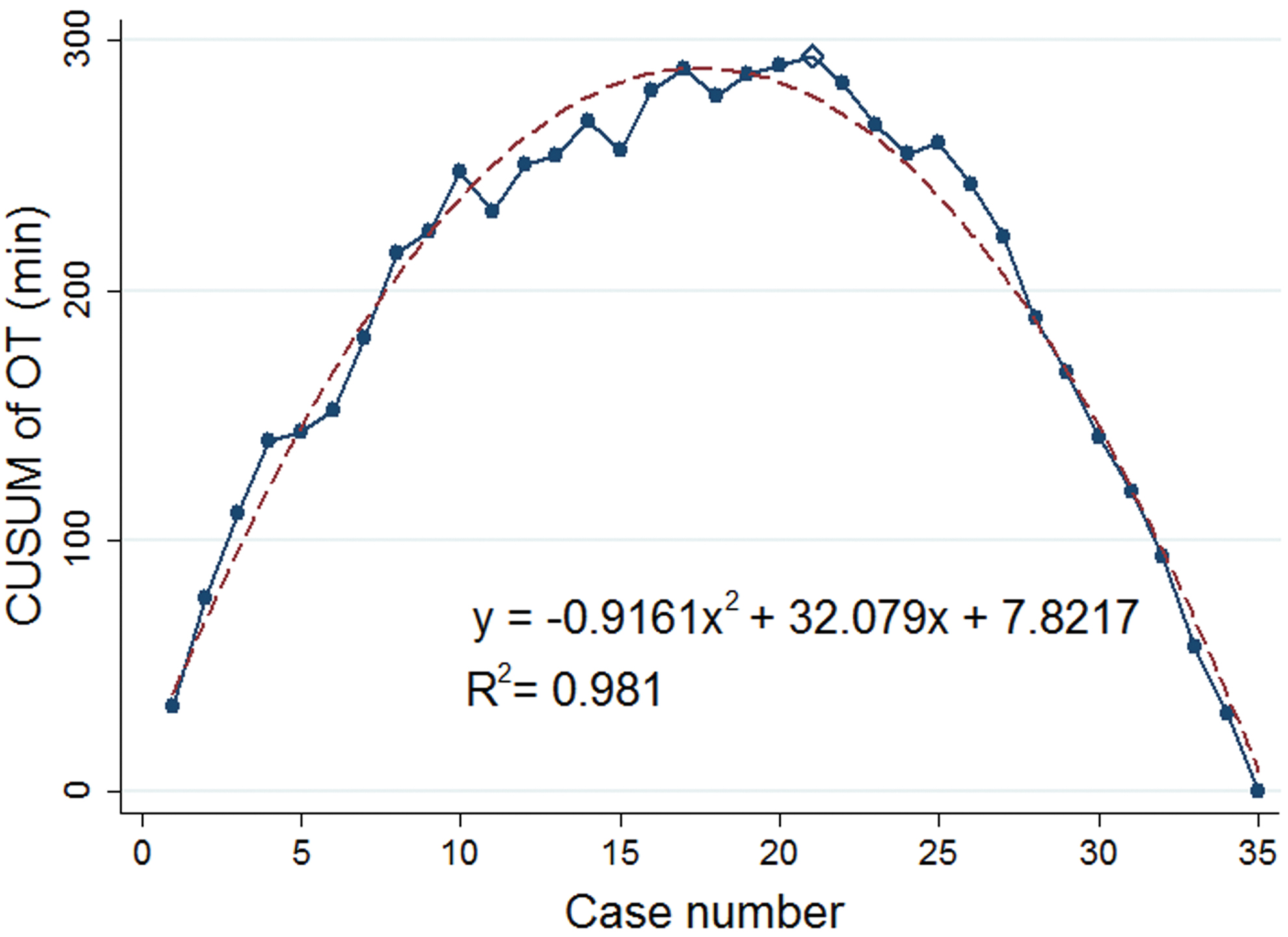
Learning curve using CUSUM of the OT plotted chronologically against case number (solid line). The curve peaked at the 21st case. The dashed line represents the curve of best fit for the plot using a second-order polynomial with equation: CUSUM = −0.9161 × case number 2 + 32.097 × case number + 7.8217 (R 2 = 0.981). CUSUM, cumulative sum; OT, operative time. Color images are available online.
The changing point of the CUSUM curve occurred at the 21st case, which divided the curve into two characteristic phases with distinct slopes. The regression lines of best fit for the curve in phase 1 (the initial 21 cases) and phase 2 (the remaining 14 cases) are demonstrated in Figure 2A, B, respectively. A positive slope in phase 1 and a negative slope in phase 2 were further proved by linear regression.

Lines of best fit for the CUSUM of the OT in each phase:
Interphase comparison
The two characteristic phases consisted of the biphasic appearance of the LC of laparoscopic KPE. Table 2 demonstrates baseline characteristics, intraoperative, and postoperative parameters in phase 1 and phase 2, respectively. In comparison, age at surgery, sex, weight, and preoperative liver function, including TBIL, DBIL, ALT, AST, as well as GGT, were well balanced between the two phases (all P-values > .05).
Comparison Between the Two Phases Identified by Cumulative Sum Analysis
Within 2 years after Kasai operation.
One case in phase 1 was lost to follow-up within 2 years after Kasai operation.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; DBIL, direct bilirubin; EBL, estimated blood loss; GGT, gamma-glutamyl transferase; NLS, native liver survival; OT, operative time; TBIL, total bilirubin.
Corresponding with the biphasic characteristics of the LC, phase 2 was observed to have shorter OT than phase 1 (240.2 ± 16.5 minutes versus 205.3 ± 10.4 minutes), and the difference was statistically significant (P < .001). Besides, less intraoperative EBL was observed in phase 2 (P = .0029).
The child lost to follow-up, who had been mentioned above, was in phase 1. The rate of 2-year NLS was higher in phase 2 compared with phase 1 (85.7% versus 45.0%; P = .030). The rate of early clearance of jaundice was higher in phase 2 than in phase 1(47.6% versus 78.6%), but the statistical difference was also borderline (P = .089). Furthermore, the rate of cholangitis was comparable between the two phases (P = .745).
Discussion
KPE is a well-established approach for surgical treatment of pediatric patients suffering from BA. Although minimal invasive surgery is more popular than conventional laparotomy nowadays, debate still persists on laparoscopic KPE. 11 The LC has been widely used to describe the relationship between a surgeon's experience and individual performance for a certain procedure. 12 As for any new surgical technique, there is an LC for laparoscopic KPE.16,17 An accurate understanding of the LC for laparoscopic KPE may improve surgeons' insight and facilitate the promotion of laparoscopic KPE. In present study, we provided quantitative assessment of the LC for laparoscopic KPE using CUSUM analysis.
CUSUM is a graphical tool for monitoring sequential measures and has gained popularity in researches on LC of various surgical procedures.16,18 It transforms raw data of a process parameter into the running total of data deviations from the overall average. A trend to a constant higher or lower value will produce a positive or negative slope, respectively. 19 CUSUM allows investigators observe changes over time, gives proof of ongoing competency in a particular procedure, displays a objective picture of individuals' experience from novice to experienced surgeons, and quantifies the process how they become proficient.15,18,19 The degree of the slope indicates the speed of surgeon's progress in mastering the new skill: the greater the slope, the slower the progress. 20
To the best of our knowledge, only two studies have particularly focused on the LC for laparoscopic KPE.16,17 Li et al. 17 summarized data of 80 children undergoing laparoscopic KPE in their medical center and divided all children chronological into four equal groups (20 cases in each group). They found that the OT was significantly decreased in group 3 compared with group 2. Ji et al. 16 enrolled 100 cases of laparoscopic KPE. Using CUSUM analysis, they found that the turning point occurred at the 50th case, and the OT was significantly decreased after the first 50 cases.
Furthermore, better prognosis after laparoscopic KPE was observed in both studies when the initial learning period was completed. Of note, the two studies were conducted in medical centers with relatively high caseload of BA. Given that surgeons in low-caseload centers face a lack of sufficient cases to master this complicated procedure, 16 experience of surgeons in high-caseload centers appears to be hardly applied to surgeons in low-caseload centers. However, no study has particularly investigated the learning course of laparoscopic KPE in medical centers with relatively low caseload of BA.
The OT is a most widely used benchmark for quantitative assessment of the LC of various surgical procedures.16–18,21 Besides, previous literature has revealed that the OT is also an important index in investigating the correlation between learning process and patient prognosis. 21 In the present study, the CUSUM analysis demonstrated that the LC of laparoscopic KPE consisted of two distinct phases: phase 1 represented the initial learning period with insufficient proficiency, and phase 2 represented the subsequent period with increased technical competency.
The upward slope of phase 1 indicated a series of OT values above the overall average, and the gradually decreased magnitude of the gradient indicated that the deviations tended to decrease, which is potentially correlated with the accumulated familiarity of laparoscopic KPE. Further analysis proved that the OT was significantly reduced in phase 2 compared with phase 1. Corresponding with previous studies,16,17 we also found that the rates of 2-year NLS and early clearance of jaundice were higher in phase 2 compared with phase 1, which suggested that prognosis of BA after laparoscopic KPE could be improved with surgical experience accumulating.
Additionally, the rate of cholangitis was comparable between the two phases in our study. Since the pathogenesis of BA has not been fully understood, 22 it is difficult to determine the exact mechanism. Although surgeons could achieve more proficient laparoscopic anastomosis of extrahepatic bile duct with experience accumulating, intrahepatic obliteration could not been solved through laparoscopic or open KPE,10,23 which may be a vital explanation. However, considering the relatively small size of study cohort in the learning period, the relationship between the rate of cholangitis and surgical competency is required to be proved by larger cohort.
For inexperienced surgeons or novices, a certain number of surgical cases are required to obtain technical competency.15,21 Given that complicated procedures necessitate more surgical cases, it appears to be difficult for surgeons to complete the LC of laparoscopic KPE owing to disease rarity of BA, especially for those in low-caseload medical centers. The present study demonstrated the learning process of laparoscopic KPE in a relatively low-caseload center, and the turning point occurred at the 21st case. Actually, in addition to the number of surgical cases, some other aspects could also influence the length of the LC of a certain procedure.12,18,20,21
For example, experience accumulated from other surgical procedures is a vital impact factor and may help surgeons complete the learning process more rapidly.15,20,24,25 First, surgeons could have a better understanding of the anatomy from open KPE and other operations for hepatobiliary disorders.15,17,25 Second, individual's practice in other laparoscopic procedures is valuable to improve proficiency in common laparoscopic manipulations and compensates the limitation of low caseload. 15
Particularly, the surgeon team in the present study have accumulated a lot of experience on open KPE before they started to perform laparoscopic KPE, which may assist them in understanding and mastering the key techniques of laparoscopic KPE. Furthermore, we also agree with Ji et al. 16 that training in animal models and laparoscopic simulators of BA could contribute to shorten the LC of laparoscopic KPE. Thus, it is possible for surgeons in low-caseload centers to obtain technical proficiency with an inferior number of surgical cases compared with existing researches in high-caseload centers.
A higher proficiency in surgical performance is often regarded to be associated with superior prognosis.12,21 In the present study and previous study,16,17 clinical outcomes of BA were observed to be improved after the initial learning phase of laparoscopic KPE. A recent meta-analysis, which we have mentioned above, suggested that superior survival was better after open KPE compared with laparoscopic KPE. 11 Of note, the majority of studies identified in this meta-analysis have small sample sizes (<20 cases), and the effect of the LC is not considered particularly in these studies. Since inferior survival after laparoscopic KPE is a major aspect hindering the recommendation of this technique, we think that it is necessary to take relevant conclusions with caution.
On one hand, results regarding clinical outcomes tend to be disadvantageous to laparoscopic KPE when surgeons have not completed the learning period and mastered this technique. On the other hand, the true differences between open and laparoscopic approaches are potentially covered by bias on occasion that surgeons perform open KPE earlier and have more experience on open approach. Thus, to accurately determine the inferiority and superiority of laparoscopic KPE, it is of great significance to consider the influence of surgical competency on clinical outcomes and evaluate whether surgeons have complete the LC.
The purpose of LC analysis is not only to determine an absolute number but also to reveal important information regarding the process of learning a new technique. The present study describes the LC of laparoscopic KPE in a low-caseload center and provides some new insight on this technique, which may inspire surgeons to reassess this technique. There are several limitations in our study. First, the literature on the LC of KPE is still scarce, and this study is performed in a single study. The external validity of our findings needs to be validated by multicenter studies. Second, the surgical team in our study had accumulated experience of open KPE before they started laparoscopic approach. The learning process may be different in surgeons with little experience of conventional laparotomy. Third, longer follow-up is required to further prove our conclusions.
Conclusions
The present study demonstrated two characteristic phases of the LC for laparoscopic KPE using CUSUM analysis. The first phase, including 21 cases, represented the initial study period, and the second phase represented the subsequent period of technical mastery. With surgical proficiency improved, shorter OT, less EBL, and better 2-year NLS were achieved. Our findings suggested that it is possible for surgeons to obtain technical competency in medical centers with relatively low caseload of BA.
Footnotes
Authors' Contributions
S.W. and J.W. conceived and designed this study. S.W. and X.H. contributed significantly to data acquisition, data analysis, and interpretation. S.W. wrote the first draft of article. J.W. contributed to reviewing and revising. All authors approved the final version.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study is funded by the Key Research and Development Plan (Social Development) of Huai'an City (Grant No. HAS201615).