
Abstract
Background:
Surgical training emphasizes technical competence. Growing evidence indicates that nontechnical skills are also significant in determining performance. Critically, surgeons should be aware how performance is affected by pressure or distraction. We assessed the impact of novel auditory and visual stressors on performance during a simulated laparoscopic task. We hypothesized that the stressors would worsen performance, and that stress-induced diminution in performance would be inversely related to surgical experience.
Methods:
Twenty participants (10 surgeons and 10 medical students) completed a peg-threading task using a laparoscopic simulator: three times under control conditions, next with a visual distraction overlay (progressive red saturation of the surgical field, timing personalized to the user's index performance), and then with an auditory distraction overlay (operating theater environment noise). Task completion time and instrument tracking metrics (instrument tip distance traveled and instrument smoothness) were measured.
Results:
Under control conditions, surgeons completed the task significantly faster, with greater economy of movement, and improved instrument smoothness—compared with students. When exposed to distracting stimuli, the groups behaved differently. Surgeons completed the task more slowly, instrument movements became less smooth (significantly so under audio distraction conditions), but total distance traveled by instruments was unchanged. By contrast, student performance was not impaired and, in some ways, improved.
Conclusion:
The impact of visual and auditory distraction on surgical performance can be modeled in a laparoscopic simulation environment. The effect of distraction varies according to expertise. This environment may be an effective setting within which to learn to mitigate stress-induced diminution in performance.
Introduction
Surgical training emphasizes technical competence and knowledge,1,2 but nontechnical skills are in fact significant in determining patient outcomes. 3 Training in nontechnical skills for surgeons (NOTSS) leads to safer and more effective surgical care.2,4–6
Simulation is an established component of most surgical training programs. Laparoscopic “box trainers” are among the most common simulation tools that permit surgical task training in an abstract and risk-free environment. A growing literature provides evidence that simulators promote and accelerate skills development that translates into real-world scenarios.7,8
Simulation can also be used to train nontechnical skills, particularly in relation to developing communication and team dynamics9,10 used in a simulated operating theater to replicate a crisis event to assess the impacts of a stressful stimulus on the social skills of the surgical team. Surgical team members gain experience in high-pressure scenarios and learn without compromising patient safety. 11 However, there is little evidence regarding the impact of external stressors on individual technical performance during technique-centric simulation tasks.
The NOTSS framework developed by Yule et al. categorizes the key cognitive and social skills necessary for surgeons to perform effectively into four overarching themes: situational awareness, decision making, communication and teamwork, and leadership. 3 This framework was built on ideas and concepts from other professions where nontechnical performance had previously been identified as a crucial to safety and optimizing performance.12,13 For example, early models of nontechnical surgical assessment incorporated the Oxford NOTECHS (nontechnical skills) and ANTS (Anaesthetists' Non-Technical Skills) rating systems, which were derived from aviation and anesthetic models of training nontechnical skills.14,15
A central feature of these programs is to manage pressure and distraction so that they do not negatively impact performance. 16 Stressful stimuli originating from the operating environment and procedure-specific tasks can severely impact a surgeon's workflow and technical proficiency. 17 Distractions present similar challenges to surgical performance, with studies detailing negative impacts on both communication and concentration within the surgical team. 18 Pressure related to time management and auditory distractions are two of the most common stressors19,20 and both negatively impact technical surgical performance and nontechnical skills. 14
Auditory distractions can be classified as either equipment related or staff related. 21 It has been shown that auditory distraction can have a profound effect on surgical proficiency. 22 Auditory distraction leads to increased stress levels among surgical staff members and can contribute to lapses in concentration from surgeons, ultimately impacting on patient safety and surgical outcomes. 16 As such, it has been suggested that background noise levels in operating theaters be kept lower than 45 dB (decibels). 23 However, a study assessing theater volume during orthopedic surgery found that the average noise level was 65 dB and reached a maximum of 120 dB. 24 Distraction is one of the most significant cognitive factors contributing toward impaired decision making. 25
Incorporating appropriate stressors into an established technique-centric simulation platform represents an environment where surgeons can test their capacity to perform under pressure, and potentially enable development of resilience to such stressors in real-world settings.
Study aim
We sought to assess the impact of superimposed auditory and visual stressors on surgeon performance during a simulated laparoscopic task. We hypothesized that auditory or visual stress would worsen performance. Secondarily, we hypothesized that stress-induced diminution in performance would be inversely related to surgical experience and capability.
Methods
A previously validated26,27 laparoscopic simulation platform with in-built instrument motion tracking software (eoSim™ with SurgTrac™, eoSurgical™ Ltd., Edinburgh) was used. The movement of both instruments is tracked during task performance through color tracking of the distal instrument shafts (Fig. 1). This study was approved by the research ethics review board of the University of Edinburgh medical school and informed by the UK Policy Framework for Health and Social Care Research.
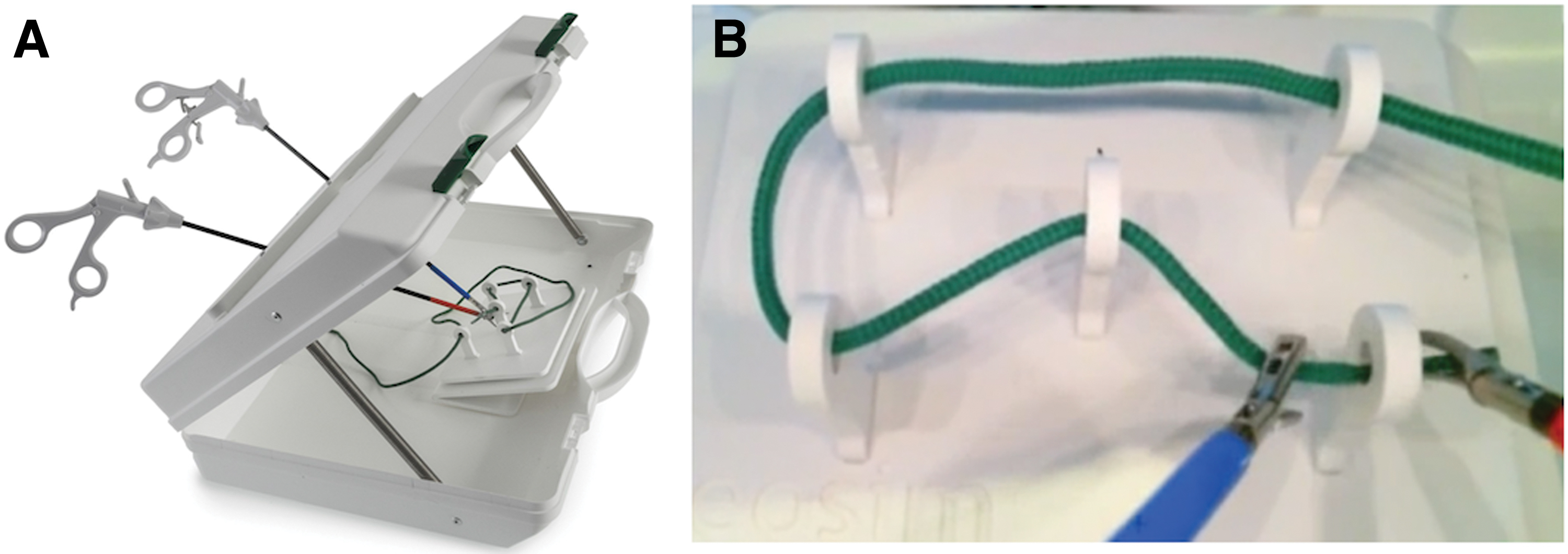
eoSim laparoscopic simulator box and a screenshot of the completed peg-threading task. Color images are available online.
Twenty participants took part in the study: 10 medical students with minimal experience of laparoscopic simulation, 10 surgeons (5 registrars and 5 consultants) with experience of both laparoscopic simulators and of performing laparoscopic procedures. A basic “thread transfer” task was chosen as it can be completed by novice users, but is also a sensitive measure of elite performance. 28 Each participant watched a short instructional video (available here: https://app.surgtrac.com/#/courses-information/37).
Experimental sequence
Each participant first performed the peg-threading task three times, sequentially, under controlled conditions with noise-canceling headphones and no interruption nor distraction. Time to complete the task, total distance traveled by both instruments, and instrument smoothness metrics were recorded for each effort.
After a brief (2 to 3 minutes) pause, each participant completed the same task with a visual distraction overlay. Participants performed the peg-threading task as previously, but, as time progressed, the laptop screen displaying the surgical field progressively became obscured by a red filter, until the entire screen was completely obscured (Fig. 2). The time to complete red saturation was personalized based on the participant's completion time for the three prior attempts under normal conditions, such that complete red saturation occurred at the mean completion time for their three control trials.
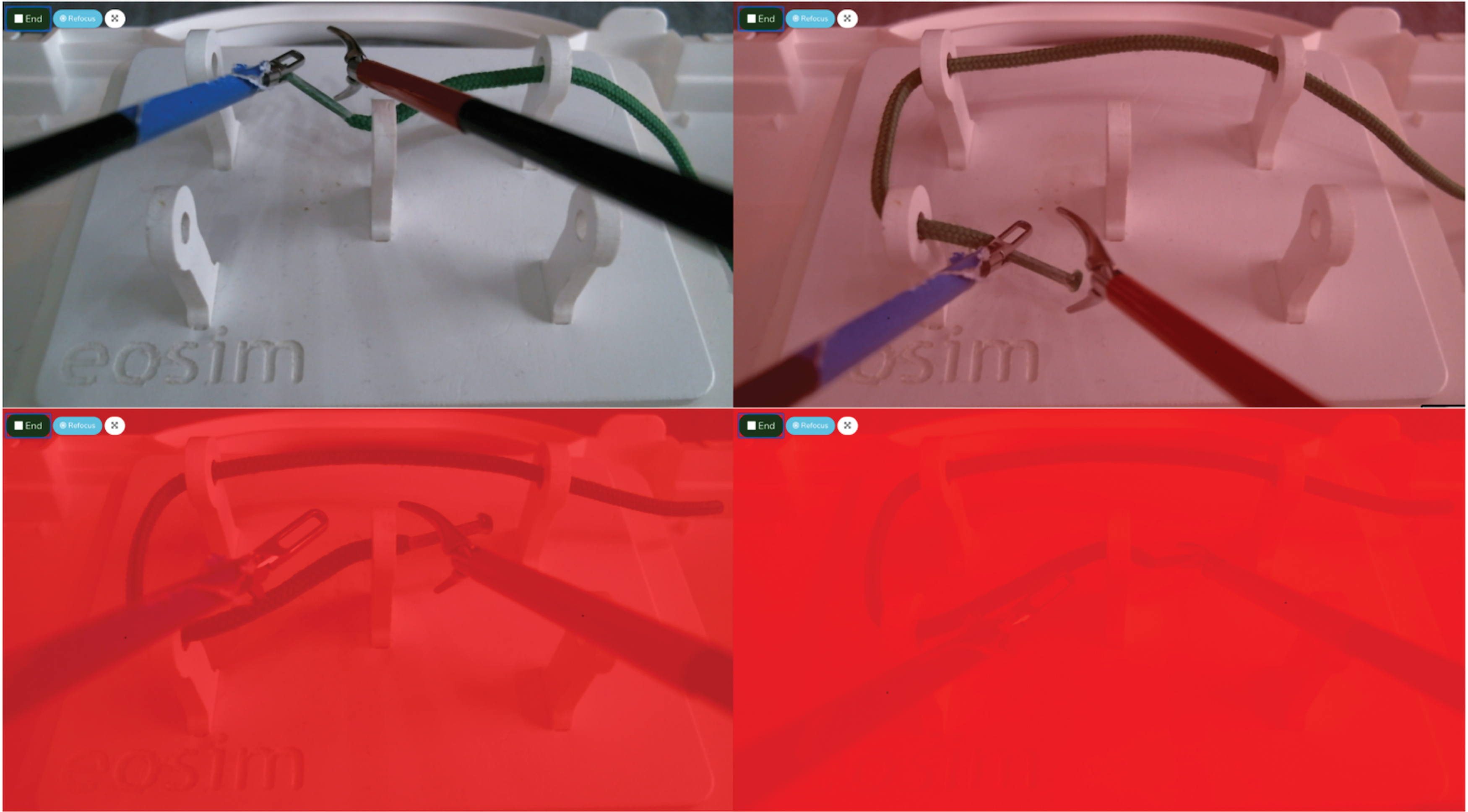
Progression of “fade-to-red” distraction overlay as the screen becomes red saturated. Color images are available online.
Finally, participants completed the peg-threading task under conditions of auditory distraction. This was generated by playing a bespoke soundtrack consisting of distractions commonly heard in operating theaters for the duration of task completion. The recording consisted of a varying rate heart rate monitor, background noise from operating machinery, work-unrelated conversations between surgical staff, and a ringing telephone. The average volume was 74.3 dB and peak 83.1 dB.
For both distraction tasks, time to complete the task, total distance traveled by both instruments, and instrument smoothness metrics were recorded. Finally, each participant provided a self-reported Likert score 29 of subjective feeling of pressure and distraction while performing the visual and audio distraction tasks (score of 1, no pressure; score of 5, extreme pressure).
Data collection and statistical analysis
Participant data were collected and stored anonymously on the simulator manufacturer's servers, before being exported into excel (Microsoft). Each participant was then assigned an identifier number and the data were analyzed using GraphPad.
The fastest performance during the three control condition trials was used as the benchmark performance for subsequent comparison with distraction conditions.
A t-test (one tailed) was used to compare differences in control condition benchmark performance metrics (time, total distance traveled by both instruments, and instrument smoothness) between the surgeon and student groups. Benchmark control performances were then compared, within each group, with performance under each of the distraction conditions.
Results
Time to task completion under control and stress conditions
Under control conditions, the mean benchmark surgeon completion time was significantly faster than that of the student group (mean 63 seconds for surgeons, 137 seconds for students, t = 4.61, P = .00012, see Fig. 3a).
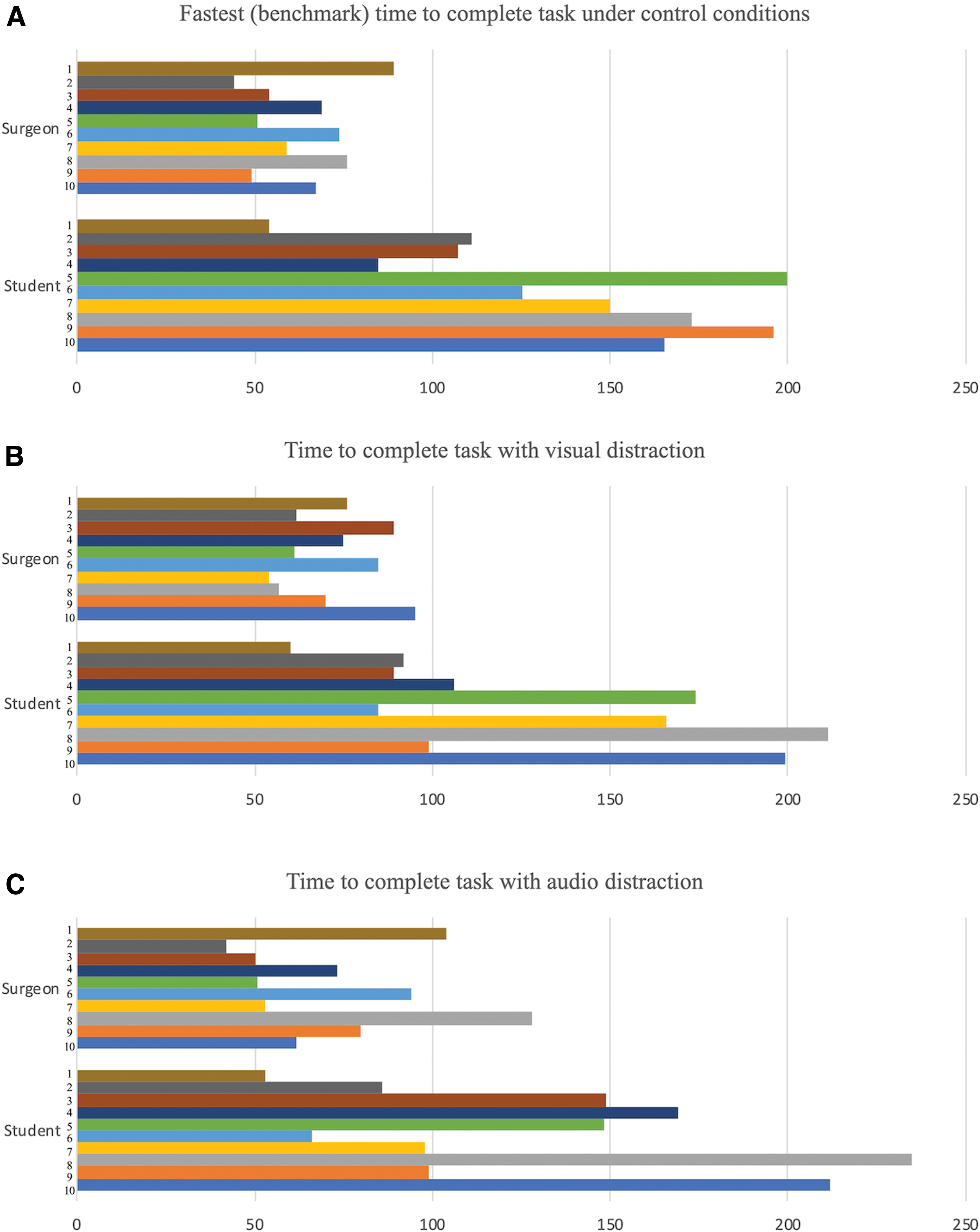
Time (s) to task completion under control
Time to complete the task under visual distraction conditions is shown in Figure 3b. Mean completion time by surgeons was 72 seconds, that for students was 128 seconds. Mean surgeon completion time slowed by 9 seconds (14%) compared with mean benchmark time under control conditions (t = −1.45, P = .081). The student cohort, in contrast, completed the task 9 seconds (7%) faster with visual distraction (t = 0.371, P = .357) than under control conditions.
Time to complete the task under audio distraction conditions is shown in Figure 3c. Mean completion time by surgeons was 74 seconds, that for students was 132 seconds. Surgeons slowed by a mean of 11 seconds (17%) compared with mean benchmark time under control conditions (t = −1.06, P = .151). The student cohort was slightly faster under audio distraction conditions (by 5 seconds or 4%, t = 0.206, P = .419) compared with control conditions.
Instrument smoothness under control and distraction conditions
Under control conditions, the surgeon benchmark efforts were achieved with significantly smoother instrument movements than that of the student group (mean 0.115 for surgeons, 0.026 for students, t = −4.56, P = .000121, see Fig. 4a).

Instrument smoothness (m/s
3
) under control
Instrument smoothness under visual distraction conditions is shown in Figure 4b. Mean instrument smoothness for surgeons was 0.081, demonstrating an attenuation of instrument smoothness of 0.034 (30%) compared with benchmark performance under control conditions (t = 1.68, P = .055). The student cohort, in contrast, deployed nonsignificantly smoother movements under visual distraction conditions (0.033, i.e. 0.007 [27%], t = −0.731, P = .237) than their control benchmark.
Instrument smoothness under audio distraction conditions is shown in Figure 4c. Mean instrument smoothness for surgeons was 0.073, an attenuation of instrument smoothness of 0.042 (37%) compared with control benchmark. This deterioration was statistically significant (t = 1.962, P = .033). The student cohort deployed smoother movements under visual distraction conditions (0.045, i.e. 0.019 [73%] smoother compared with benchmark), though not quite statistically significant (t = −1.48, P = .078).
Total instrument movement during control and distraction conditions
The surgeon control benchmark performance involved significantly lower combined instrument movements than the student group (surgeon mean 1.63 m, student mean 3.37 m, t = 2.22, P = .020, see Fig. 5a).

Total instrument movement (m) during control
In visual distraction conditions, the surgeon cohort combined instrument movement increased minimally compared with their benchmark score (mean distance 1.64 m, 1% increase, t = −0.0223, P = .491). For students, there was a minimal reduction in total instrument movements under visual distraction conditions (mean distance 3.28 m, t = 0.0798, P = .469) compared with the mean student benchmark score.
In audio distraction conditions, the surgeon cohort combined instrument movement distance reduced minimally compared with benchmark under control conditions (mean distance 1.52 m, 7% reduction, t = 0.418, P = .340). For students, there was again a minimal reduction under visual distraction conditions (mean distance 3.29 m, t = 0.0537, P = .479) compared with student benchmark score.
Subjective sensation of distraction during visual and audio augmented tasks
The mean Likert score for subjective distraction for visual overlay was 2.4/5 for surgeons and 2.9/5 for students. The mean Likert score for subjective distraction induced by the auditory overlay was 2.9/5 for surgeons and 3.1/5 for students.
Discussion
This study provides evidence that a box trainer and instrument tracking environment can be used to assess the effect of external stressors on technical performance. Visual and auditory distractors impacted performance of expert surgeons, underscoring the impact and potential risk of these events during live surgery.
Under control conditions, surgeons completed the simulated laparoscopic task significantly faster, with fewer instrument movements (i.e., greater economy of movement), and with greater instrument smoothness than students, as would be expected. When exposed to auditory or visual distracting stimuli, the two groups behaved differently. Surgeons completed the task somewhat slower; their instrument movements became less smooth (significantly so under audio distraction conditions), but the total distance traveled by instruments was unchanged.
The clinical impact of impaired instrument smoothness is difficult to quantify, but it is unlikely to be positive. The increased time taken to complete the task under distraction conditions was not statistically significant. The time increase was modest, but the assessed task was brief and a similar percentage increase for a longer surgical task would have significant implications on workflow in the operating theater.
Both the visual and auditory overlays used here aimed to increase pressure on the participant. Pressure may not always be detrimental to performance. Some surgeons report that small amounts of pressure can be beneficial, heightening focus and helping concentration. 18 The ability to utilize pressure to enhance performance has been documented as one of the eight core elements of surgical leadership. 30 Indeed, in professional sport, multi-Grand Slam tennis champion Billy Jean King noted “pressure is a privilege.”
Some surgeons actively suppress feelings of stress to prevent it from visibly affecting their performance. 31 Surgical trainees have also reported that they can feel ill equipped to adequately deal with stress, often developing their own coping mechanisms to perform under pressure. 18 Both of the distraction overlays resulted in largely similar subjective feelings of distraction among surgeons and students. Learning how to manage that stress is crucial to safe performance.
In contrast with surgeons, student laparoscopic simulator performance was not impaired under distraction conditions; in some ways it improved. The explanation for this likely lies in their learning curve being particular steep at this stage. Iterative improvement in performance with sequential task repetition likely dominates or obscures any attenuation that may come with distraction. For established surgeons, working on a flatter learning curve with a much higher baseline performance capability, distraction results in a discernible aberration.
This analysis has been based on mean performance among the two different cohorts. It is important to highlight the marked variation in the impact of distraction upon individual performances:
- One surgeon had a benchmark time of 59 seconds but improved to 54 seconds with visual distraction and 53 seconds with audio distraction. Motion smoothness was essentially unaffected by distraction (0.08 benchmark, 0.1 visual distraction, 0.08 audio distraction). Total instrument distance was lower under audio distraction conditions (1.41 m benchmark, 1.43 m visual distraction, 1.03 m audio distraction). They reported a relatively low (2/5) subjective perception of distraction. As such, they appear unhindered—if not improved—under distraction conditions. - This compares with another surgeon: benchmark time of 49 seconds, slowing to 70 seconds with visual distraction and 80 seconds with audio distraction. Motion smoothness was negatively impacted by distraction (0.17 benchmark, 0.1 visual distraction, 0.07 audio distraction). Total instrument distance also increased under distraction conditions (1.85 m benchmark, 2.49 m visual distraction, 2.15 m audio distraction). They reported a higher (3/5) subjective perception of distraction.
Detecting this difference is important as it highlights a potential opportunity to improve the second surgeon's performance under conditions of distraction or pressure. Further studies, with larger cohorts and more assessments, are needed to explore these observations further. It should then be possible to explore whether training in simulated situations that incorporate stressors can mitigate the negative impact of the distraction, and whether and how these nontechnical skills translate into real-word performance.
In conclusion, visual and auditory distraction affecting surgical performance can be modeled in a laparoscopic simulation environment. The impact of distraction appears to vary according to expertise. This simulation environment may be an effective environment in which to develop mitigation strategies for stress-induced diminution in performance.
Footnotes
Disclosure Statement
Lewis Swan and Caitlyn L. Taylor have no conflicts of interest nor financial ties to disclose. Mark A. Hughes, Roland Partridge, and Paul M. Brennan are founders of eoSurgical Ltd., the manufacturers of the eoSim simulator, eoSurgical Ltd. Razvan Ilin is an employee of eoSurgical Ltd.
Funding Information
This research did not receive any funding from agencies in the public, commercial, or not-for-profit sectors.