
Abstract
Background and Aim:
The distribution of board-certified pediatric surgeons (BCPSs) in Japan is highly biased. While Prefecture M has one of the smallest numbers of BCPSs per pediatric population, neighboring Prefecture K has one of the largest numbers of BCPSs per pediatric population. We examined the effect of BCPSs population on laparoscopic surgery and postoperative management and outcomes.
Materials and Methods:
We compared postoperative duration to full-dose enteral nutrition, postoperative hospital stay, and complications of neurologically impaired patients who underwent laparoscopic fundoplication in two prefectures from 2006 to 2019.
Results:
Laparoscopic fundoplication was performed in 17 patients in Prefecture M and 63 in K. The mean operative time was 248.8 ± 79.9 minutes in Prefecture M and 260.8 ± 94.8 in K (P = .64). The median number of days to full-dose enteral nutrition was 11.5 in Prefecture M and 10 in K (P = .29). The median postoperative hospital stay was 14 days in Prefecture M and 15 days in K (P = .38). Postoperative complications occurred in 7 cases in Prefecture M and in 10 in K. The incidence was significantly higher in Prefecture M than in K (P = .041).
Conclusion:
Areas with insufficient numbers of BCPSs have a higher risk of complications in laparoscopic surgery than areas with sufficient numbers.
Introduction
In 2019, the number of pediatric surgeons certified by the Japanese Society of Pediatric Surgeons (JSPS) was 3.88 per 105 people younger than 15 years of age nationwide; however, this distribution is highly biased depending on the region and prefecture.
Both Prefecture M and Prefecture K are located next to each other in the southernmost part of the Kyushu region in Japan. According to 2019 statistics, Prefecture M had a population of 10.72 × 105, of which 1.42 × 105 (13.3%) were younger than 16 years of age. 1 Neighboring Prefecture K had a population of 16.02 × 105, of which 2.12 × 105 (13.2%) were younger than 15 years of age. 2 There is one national university faculty of medicine in each prefecture. Prefecture M has one of the lowest numbers of board-certified pediatric surgeons (BCPSs) per 105 people younger than 15 years of age in Japan at 1.41, while Prefecture K has one of the highest numbers at 5.66 in 2019. We speculated that the risk of operative complications would be higher in areas with fewer BCPSs because of a significantly greater individual workload than in regions with more BCPSs.
The number of neurologically impaired patients (NIPs) is increasing in Prefecture M as well as in other prefectures, although increasing numbers of lives are being saved because of advances in perinatal care, neonatal intensive care, and pediatric emergency medicine. The demand for surgical interventions for NIPs is therefore likely to increase in both prefectures, as in other regions.
In the present study, we compared the operative outcomes of laparoscopic fundoplication for NIPs and the frequency of postoperative complications of fundoplication in both prefectures. In addition, we examined the effect of the number of BCPSs on complications of laparoscopic fundoplication for NIPs.
Materials and Methods
Study design
We compared the pediatric population and the number of BCPSs in Prefectures M and K annually. We retrospectively reviewed the medical records of severe NIPs who underwent laparoscopic fundoplication for gastroesophageal reflux disease at the university hospitals in Prefectures M and K between January 2005 and December 2019. All procedures were laparoscopic Nissen fundoplication.
The patient characteristics and outcomes that were analyzed included the age at the time of surgery, underlying disease, surgical procedure, operative time, presence or absence of gastrostomy in advance, postoperative complications, postoperative duration of hospital stay, postoperative duration until enteral feeding at full dose, and mortality. Complications were defined as Grade ≥II according to the Clavien-Dindo Classification.3,4
Statistical analyses
The Mann–Whitney U test was used for group comparisons of the age at surgery, postoperative duration of hospital stay, and postoperative duration to enteral feeding at full dose. A t-test was used to compare the operative time. The relationship between the incidence of complications and the number of pediatric surgeons per pediatric population was analyzed with Fisher's exact test.
Ethical approval
This study was performed in accordance with the Ethical Guidelines for Clinical Research from the Japanese Ministry of Health, Labor, and Welfare. This study was approved by the Institutional Review Board of the University of Miyazaki.
Results
The distribution of BCPSs
The annual trend in the number of BCPSs per pediatric population in both prefectures is shown in Figure 1. The annual average number of BCPSs was 0.93 ± 0.62 in Prefecture M and 3.75 ± 1.08 in Prefecture K, significantly higher in Prefecture K (P < .001).

The number of BCPSs per 105 population younger than 15 years of age. The line graphs show the annual trend in the number of BCPSs per 105 population younger than 15 years of age in two prefectures from 2006 to 2019. Black dots and line: Prefecture M; white dots and line: Prefecture K. BCPSs, board-certified pediatric surgeons.
Patients' characteristics
The patient characteristics are shown in Table 1. A total of 17 NIPs (male, n = 11; female, n = 6) with gastroesophageal reflux in Prefecture M and 63 patients (male, n = 51; female, n = 12) in Prefecture K were registered in the present study. The median age at surgery was 12.14 years old in Prefecture M and 13.57 years old in Prefecture K (P = .60). There were 3 patients with gastrostomy in advance in Prefecture M and 8 such patients in Prefecture K (P = .69).
Patient Characteristics
Table 2 shows the underlying diseases. Hypoxic encephalopathy was seen in the largest number of patients in both prefectures. Other underlying diseases, such as malformation syndromes, a low birth weight, accidents, and metabolic diseases, were prominent in both prefectures.
Underlying Diseases (Some Overlap)
The operative time and postoperative courses
The operative time and postoperative courses are shown in Table 3. The average operative time was 248.8 ± 79.9 minutes in Prefecture M and 260.8 ± 94.8 minutes in Prefecture K. There was no significant difference (P = .64).
Operative Results and Outcomes
The median duration to full-dose enteral nutrition was 11.5 days (range: 5–45) in Prefecture M and 10 days (range: 3–39) in Prefecture K. There was no significant difference (P = .29).
The median postoperative hospital stay was 14 days (range: 2–103) in Prefecture M and 15 days (range: 7–39) in Prefecture K. There was no significant difference (P = .38).
Postoperative complications
Table 4 shows the postoperative complications. Postoperative complications occurred in 7 cases (41.2%) in Prefecture M and 10 cases (15.9%) in Prefecture K. The incidence was significantly higher in Prefecture M than in Prefecture K (P = .041). Prefecture M reported the following complications: delayed gastric emptying, 3 (17.6%); ileus, 2 (11.8%); sepsis, 2 (11.8%); and hiatal hernia (recurrence), 1 (5.9%). Prefecture K reported the following complications: sepsis, 2 (3.2%); ileus, 1 (1.6%); pneumonia, 5 (7.9%); surgical site infection, 1 (1.6%); dumping, (1.6%); and skin ulcer around gastrostomy, 1 (1.6%)
Complications of Prefecture M and Prefecture K
Regarding mortality, one patient in Prefecture M and two patients in Prefecture K died during hospitalization. The patient in Prefecture M died of sepsis at postoperative day 2. One patient in Prefecture K died of sepsis at postoperative day 36, and the other died of severe necrotizing enterocolitis at postoperative day 11.
The trends in the number of BCPSs per pediatric population, surgeries, and complications in each prefecture are shown in Figure 2. There was no significant correlation between the incidence of complications and the number of BCPSs per pediatric population due to the wide variation in the number of surgeries and complications per year.
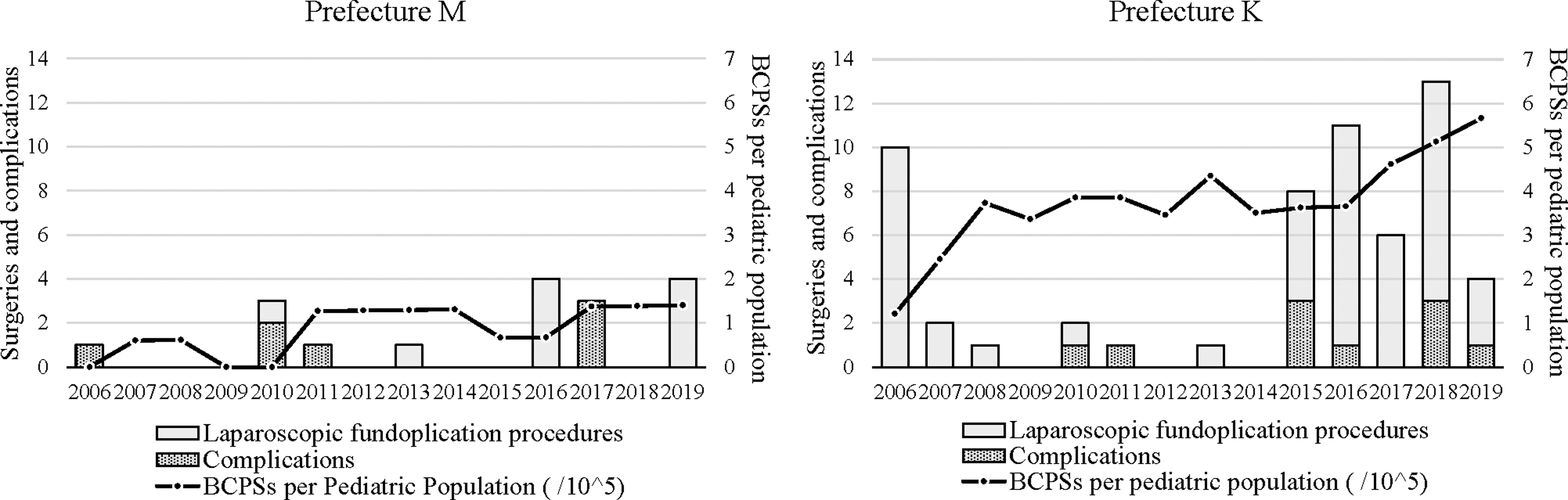
The number of laparoscopic fundoplication procedures, complications, and BCPSs per 105 population younger than 15 years of age.. The bar graphs show the annual number of laparoscopic fundoplication and complications in each prefecture from 2006 to 2019. Gray bars: laparoscopic fundoplication; meshed bars: complications. The line graphs show the annual trend in the number of BCPSs per 105 population younger than 15 years of age in each prefecture from 2006 to 2019. BCPSs, board-certified pediatric surgeons.
Discussion
In Prefecture M, there are only two hospitals in the prefectural capital where pediatric surgeons are stationed, and the university hospital mainly provides surgical intervention for NIPs. In the northern part of Prefecture M, surgeries are sometimes performed at hospitals in other prefectures due to accessibility issues, but because of the small pediatric population in the area, our hospital is believed to cover the majority of surgical interventions for NIPs in Prefecture M. In contrast, in Prefecture K, there are five hospitals in the prefecture where pediatric surgeons are stationed, although surgical interventions for NIPs are performed only at the university hospital.
The present study clarified the following: (1) The annual average number of BCPSs in Prefecture K was significantly higher than that in Prefecture M; (2) there were no significant differences in operative time, postoperative duration to enteral feeding at full dose, and postoperative hospital stay between the two prefectures; and (3) the incidence of complications was significantly higher in Prefecture M than in Prefecture K.
In the present study, there were no significant differences between the two prefectures in operative time, postoperative stay in the hospital, or postoperative duration until enteral feeding at full dose. Ru et al. performed a systematic review and meta-analysis to compare laparoscopic Nissen fundoplication with open Nissen fundoplication for children with gastroesophageal reflux disease. 5 According to their analysis, the laparoscopic group had a significantly longer operative time than the open group. In contrast, there was no significant difference in the time to full feeding. Although not included in the meta-analysis, the postoperative hospital stay was not significantly different or was longer in the open laparotomy group than in the laparoscopic group.6–10
The present study did not include open surgery cases. The lack of any marked difference in the operative time, duration to full enteral nutrition, and hospital stay between the prefectures in this study was attributed to laparoscopic surgery expert board-certified instructors in pediatric surgery from Prefecture K visiting Prefecture M to provide surgical guidance and instruction in cases for which there were few or no specialists in Prefecture M.
The incidence of postoperative complications was significantly higher in Prefecture M than in Prefecture K. Laparoscopic fundoplication for NIPs is sometimes technically difficult due to body deformity and malposition of the organs. In addition, perioperative management demands specific care and support due to respiratory problem, malnutrition, and underlying disease. Numerous previous studies have demonstrated close relationships between the number of pediatric operations performed at institutions and improved patient outcomes.11–14 The relationship between the pediatric surgical volume and outcomes may be due to the high level of familiarity of pediatric surgeons as well as anesthesiologists, nurses, and other ward staff with pediatric-specific anatomical and physiological differences and pediatric-specific pathological and surgical procedures.
Saka et al. compared the frequency of postoperative complications between centers with (Group A) and without (Group B) pediatric surgeons qualified by the endoscopic surgical skill qualification system (ESSQS) established by the Japanese Society for Endoscopic Surgery (JSES) and found that Group A had a significantly higher frequency of complications than Group B. 15 This result may have been due to the tendency for “advanced” endoscopic surgery to be performed more aggressively in Group A centers than in Group B centers and the small number of ESSQS-certified pediatric surgeons, which accounted for only 10% of the BCPSs recognized by the JSPS and thus may have biased the results significantly. In the present study, the BCPSs did not include ESSQS-certified surgeons in either prefecture.
There have been several reports on regionalization of pediatric surgical care. Taking biliary atresia (BA) as an example, in 1999, the management of BA was centralized in the United Kingdom to three centers. Davenport reported that this centralization improved the native liver survival and overall survival. 16 Even for diseases other than BA, Salazar shows that different types of pediatric surgeries tend to be concentrated in high-volume centers. 17
However, critiques of the overcentralization of pediatric surgery cannot be ignored. In the debate at the 48th Annual Meeting of the Canadian Association of Pediatric Surgeons in 2016, Mueller pointed out issues with the regionalization of pediatric surgical care, including an increased financial burden on families, psychological stress associated with separation from family members, delays in treatment due to a long travel distance, and loss of regional expertise. 18
In both prefectures, M and K, access to pediatric surgical facilities across the border is time-consuming because of poor-quality highway networks and public transportation, due to the mountainous terrain of the regions. Apart from a few large metropolitan areas, the makeup of these two prefectures does not markedly differ. Therefore, standard pediatric surgical care should be completed within the prefecture whenever possible, apart from cases requiring a high level of expertise in perioperative management, such as organ transplantation and tracheal surgery. As centralizing pediatric surgical cases across prefectures is not ideal, a sufficient and equalized number of BCPSs per pediatric population is necessary to provide safe pediatric surgical care.
Limitations
Several limitations associated with the present study warrant mention, including the small number of cases, the retrospective nature, and inadequate information concerning risk factors, such as the preoperative nutritional status. We need to improve these aspects when conducting further analyses in the future.
Conclusions
The present study showed that insufficient numbers of BCPSs correlated with an increasing risk of postoperative complications in laparoscopic fundoplication for NIPs compared with areas with sufficient numbers of BCPSs. A sufficient and equalized number of specialists is necessary to ensure that pediatric surgeries are performed as safely as possible.
Footnotes
Acknowledgment
We thank Mr. Brian Quinn for his comments and help with the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (JSPS: 20K10403, 19K09150), research grant from the Kyushu Society Endoscopic and Robotic Surgery, research grant from The Mother and Child Health Foundation, and research grant from the Kawano Masanori Memorial Public Interest Incorporated Foundation for Promotion of Pediatrics.