
Abstract
Objective:
The purpose of this study was to compare the safety and efficacy of hand-sewn versus stapled anastomosis therapy in intestinal atresia neonatal patients.
Materials and Methods:
This was a prospective randomized controlled trial in which 90 neonates with intestinal atresia were randomly divided into the hand-sewn group and the stapled group. All patients were assigned to undergo intestinal anastomosis by hand-sewn or stapler. The primary outcome measure was to analyze the anastomotic complications between groups. The secondary outcome measures were operative time, blood loss, length to initial feeds, length to full feeds, length of hospital stay, the incidence of bowel obstruction, reoperation and mortality, and weight and height 1 year after operation.
Results:
A total of 82 patients were included (43 for hand-sewn and 39 for stapled group) for primary analysis. A total of 16 patients suffered from anastomotic complications in both groups. The incidence rate of anastomotic complications in the stapled group was significantly lower than that of the hand-sewn group (27.9% versus 10.3%, P = .044). There were no differences in anastomotic leak, stricture, and bleeding in the hand-sewn group compared with stapled group. The operative time in the hand-sewn group was longer than the stapled group (P < .001), the length to initial and full feeds in the stapled group was shorter than that of the hand-sewn group (P < .001). The length of hospital stay was significantly shorter in the stapled group than the hand-sewn group (P = .016). The bowel obstruction, reoperation, weight and height, and mortality had no differences between groups during follow-up.
Conclusion:
Study results demonstrate that stapled anastomosis is safe and effective for intestinal atresia with distal diameter >1 cm, as it can decrease the incidence of anastomotic complications. However, the risk of anastomotic failure should be considered among type III b atresia.
Clinical Trial Registration number: NCT03754907.
Introduction
Stapling devices were first introduced for intestinal anastomosis by Steichen and Ravitch in 1973. 1 Many studies have reported that the stapled intestinal anastomosis has advantages that it may decrease the related complications of intestinal anastomosis used in adults and children.2–4 Owing to the low matching degree of the size of stapling devices and the diameter of intestinal lumens in neonate, 5 the application of stapler in neonatal intestinal anastomosis was limited.
With the development of minimally invasive surgery and smaller staplers for laparoscopic or thoracoscopic surgery, stapled anastomosis is becoming possible again in neonates. At present, there were only a few reports including a small number of neonatal patients about the application of stapling devices in neonates with intestinal anastomosis.5–8 But there were no randomized controlled trials (RCT) studies to confirm this conclusion yet; the aforementioned studies also did not deeply explore the effects of intestinal diameter on stapled anastomosis in neonatal intestinal atresia.
To overcome the limitations of previous studies, we tested the hypothesis that stapled anastomosis can be successfully applied to neonatal patients with intestinal atresia by conducting a noninferiority RCT compared with conventional hand-sewn anastomosis.
Materials and Methods
This trial had been registered at ClinicalTrial.gov before initiation and was designed as a randomized controlled study. This study was approved by the regional Ethical Committee for Medical Research of Zunyi Medical University (approval no. 20180812081) and conducted in accordance with the Declaration of Helsinki. Patients with intestinal atresia who were surgically treated at the Affiliated Hospital of Zunyi Medical University from January 2018 to December 2020 were included into this clinical study chronologically. All possible patients were screened first by the research stuff.
Recruited patients for this trial should meet all the following inclusion criteria: age from 1 to 30 days; clinical diagnosis of intestinal atresia according to clinical presentations (vomiting, abdominal distension, and failure to pass meconium), abdominal ultrasound, and gastrointestinal radiography. Exclusion criteria included the following: duodenal atresia, membranous type atresia, intestinal atresia patients complicated with intestinal perforation, combined with two or more intestinal malformations, severe cardiopulmonary disease, and instability of vital signs.
A web-based system Stata software to generate random grouping numbers was used for randomization. Patients were randomized in a 1:1 allocation ration. Each randomized patient was given a unique study ID number. Randomization was performed the day before surgery. Based on the literature reported, 6 the incidence of anastomosis-related complications in the stapled group was assumed to be 30.8%, the incidence of anastomosis-related complications in the hand-sewn group was assumed to be 12.5%.
The P value for the two-side test was .05, and the test power (1−β) was 80%. Thus, the power and sample size.com was used to calculate the optimal sample size was 76. Considering that 10% of the patients might be lost to follow-up, we calculated that at least 84 patients were needed for this study.
Surgical management for intestinal atresia was performed by laparotomy. Patients who received hand-sewn or stapled anastomosis for intestinal anastomoses were all performed by 1 of the 3 pediatric surgeons; surgeons were all skilled for intestinal anastomosis procedures in neonatal surgery. If necessary, resection of proximal dilated and atretic bowel with primary end-to-end anastomosis. Hand-sewn intestinal anastomoses were performed using a single layer of interrupted 5/0 vicryl in an end-to-end manner.
Stapled intestinal anastomoses were done using the EC60A endoscopic linear cutting stapler and two 2.6 mm staple height staplers (Ethicon Endo-surgery, Inc., Chihuahua, MEXICO) in a side-to-side (Fig. 1A), functional end-to-end technique (Fig. 1B). The dilated proximal intestine was cannulated with the larger anvil of the endoscopic linear cutter. Likewise, the distal intestinal lumen was cannulated with the smaller anvil of the endoscopic linear cutter (Fig. 1A). Before firing the cutter and completing the anastomosis, the cutter was positioned onto the no vascular area on the side of the intestinal lumen. The mesenteric defect was closed with 5/0 vicryl, completing anastomosis (Fig. 1C).
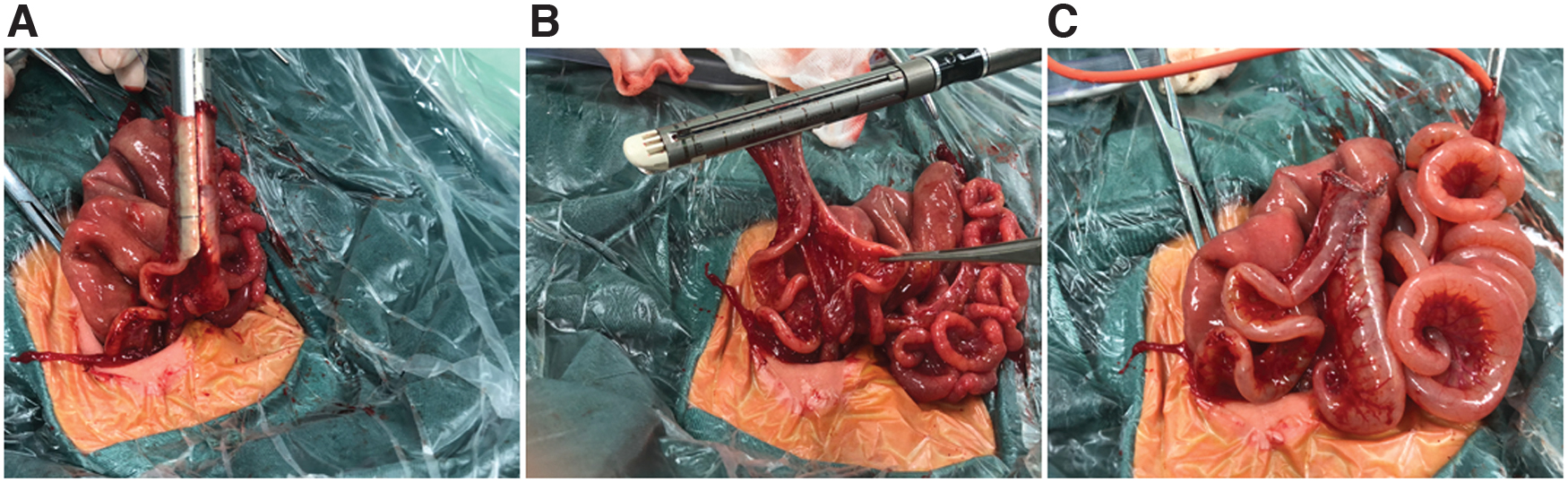
Stapled anastomosis procedures.
The primary outcome measure was to compare the anastomotic complications of intestinal atresia (leak, stricture, and bleeding) after hand-sewn or stapled anastomosis in neonates. Secondary outcome measures were length to initial feeds, length to full feeds, length of hospital stay, the incidence of bowel obstruction and reoperation, postoperative complications and prognosis were investigated, weight and height at 1 year, all patients were followed-up for at least 1 year.
Statistics analysis was performed with statistical package for social science (SPSS) software for windows, version 22.0 (SPSS, Inc., Chicago, IL). Normally distributed variables were compared using t-tests and expressed as mean ± standard deviation, in situations of non-normality, t-tests were replaced by nonparametric equivalents (Mann–Whitney U or Kolmogorov–Smirnov test). Categorical data were compared using Pearson's chi-square test or Fisher's exact test as appropriate and expressed by percentage frequency. A P value <.05 was considered statistically significant.
Results
From January 2018 to December 2020, we screened 113 neonates who had planned for intestinal anastomosis surgeries. According to the inclusion and exclusion criteria, 90 patients were included and randomly assigned to the hand-sewn group or the stapled group. There were no significant differences between the hand-sewn and stapled group in clinical characteristic information such as gender, age, weight at surgery, type of atresia, and the anastomotic levels (Table 1).
Comparison of Clinical Characteristics of Patients
Pearson's chi-square and #independent-sample t-test were used to compute P value.
Two patients in hand-sewn group were excluded from this study, because 1 patient lost follow-up and 1 patient complicated with Fallot's tetralogy died at sixth month after operation, leaving 43 patients in the hand-sewn group included in the primary analysis. Six patients in the stapled group were excluded from this study because 5 type III b atresia patients were changed to hand-sewn due to the diameter of distal intestinal canal of atresia was <1.0 cm, and 1 ileal atresia patient complicated with HSCR in 3 months postoperatively, which was not diagnosed in her neonatal period. Eventually, 39 patients in the stapled group were included into the primary analysis (Fig. 2).
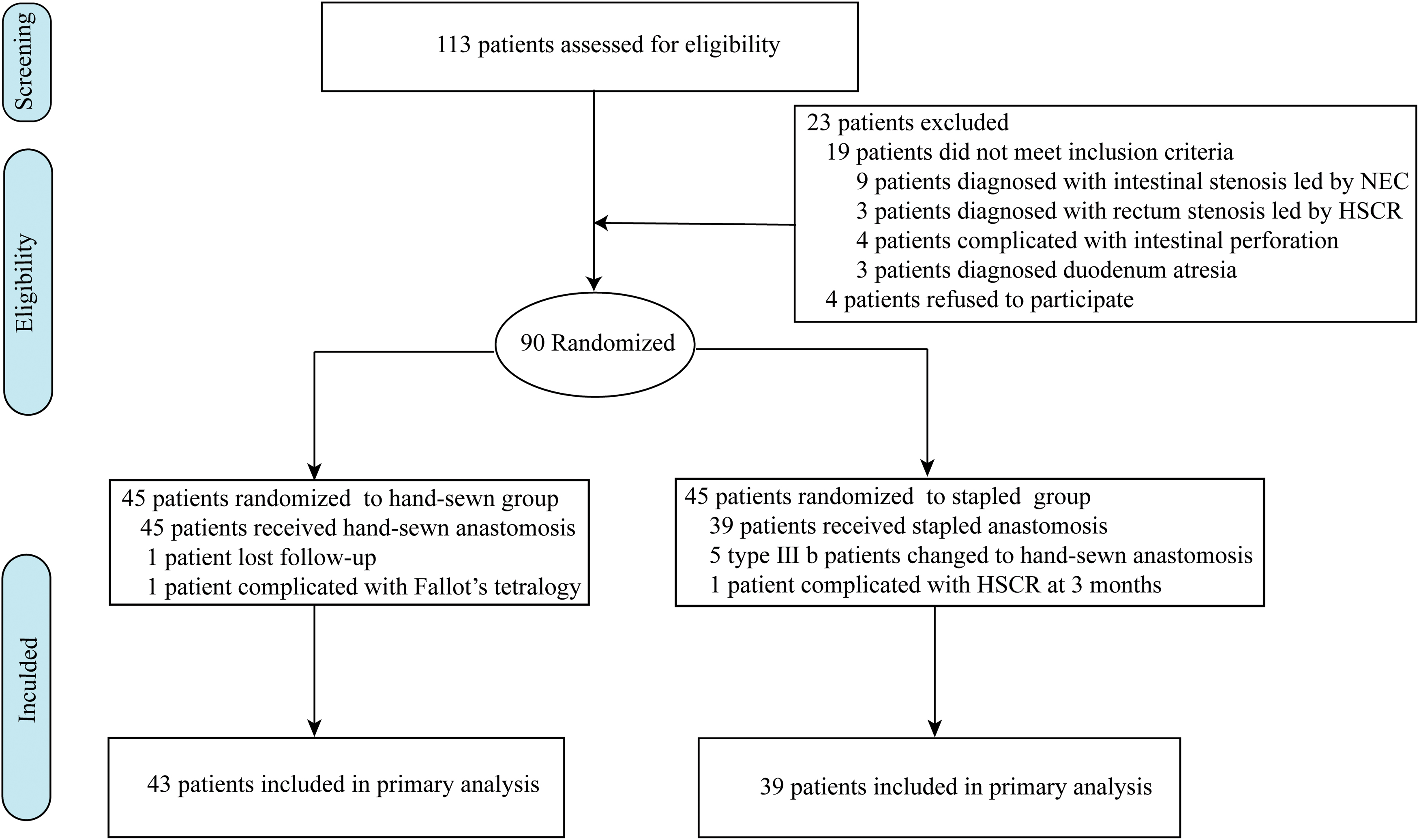
Flow diagram for patients randomized to hand-sewn group and stapled group. Color images are available online.
Anastomotic complications occurred in 12 patients in the hand-sewn group and 4 patients in the stapled group. Among the 12 patients in the hand-sewn group, 3 patients developed anastomotic leak, 7 patients developed anastomotic stricture, and 2 patients suffered from both anastomotic leak and stricture. There were 2 anastomotic stricture and 2 anastomotic bleeding in the stapled group, resulting in an anastomosis-related complication rate of the hand-sewn group significantly higher than that of the stapled group (27.9% versus 10.3%, P = .044).
The incidence rate of anastomotic leak in the hand-sewn group had no significant difference compared with the stapled group (7.0% versus 0%, P = .243). There was no significant difference between the incidence rate of anastomotic stricture and bleeding in hand-sewn group compared with the stapled group, respectively (Table 2).
Primary Outcomes in Hand-Sewn and Stapled Group
Chi-square and &Fisher's exact test were used to compute P value.
In terms of secondary outcome measures (Table 3), the operative time in the hand-sewn group was longer than the stapled group (108.8 ± 16.1 versus 90.7 ± 10.1 minutes, P < .001), there were no significant differences in blood loss between two groups (12.3 ± 5.5 versus 11.3 ± 4.4 mL, P = .409). The length to initial and full feeds in hand-sewn group was longer than the stapled group, patients in the stapled group tolerated feeds early (length to initial feeds: 5.4 ± 1.8 versus 2.5 ± 0.8 days, P < .001; time to full feeds: 11.3 ± 2.1 versus 8.9 ± 2.1 days, P < .001). The length of hospital stay was significantly shorter in the stapled group than hand-sewn group (16.6 ± 4.0 versus 18.5 ± 2.9 days, P = .016).
Secondary Outcomes in Hand-Sewn and Stapled Group
Independent-sample t-test, *chi-square, and &Fisher's exact test were used to compute P value.
There were no significant differences in the incidence of bowel obstruction (9.3% versus 5.1%, P = .678) or reoperation (7.0% versus 2.6%, P = .617) between the two groups during the follow-up. Three patients in the hand-sewn group underwent reoperation in which 1 patient developed bowel obstruction 5 months postoperatively and received enterolysis at the age of 6 months and 2 patients developed anastomotic stricture at the age of 2 and 7 months postoperatively and recovered by stapled anastomosis at the age of 4 and 7 months, respectively. One patient in the stapled group complicated with adhesive bowel obstruction and recovered by enterolysis at the age of 9 months.
There were 2 cases of death in the hand-sewn group during follow-up: 1 patient died on the 12th postoperative day caused by peritonitis and 1 patient died on the fourth month due to gut failure. One patient died on the 35th postoperative day of pulmonary infection in the stapled group. The mortality rate had no significant difference between two groups. All the patients were measured for the growth and development at 1 year after surgery. No significant differences were observed with regard to weight (8.5 ± 0.9 versus 8.5 ± 1.0 kg, P = .755) and height compared between groups (68.4 ± 2.9 versus 67.3 ± 3.4 cm, P = .142).
Discussion
Traditionally, hand-sewn with an end-to-end anastomosis technique was the most popular pattern in intestinal atresia. 3 Stapled anastomoses of gastrointestinal tract were rarely performed in newborns. In 1995, Powell 9 first reported a study that used an intestinal stapler for intestinal anastomosis for 7 newborns and infants with an average weight of 3.7 kg and an average age of 72 days.
The development of smaller stapling devices for neonatal procedures presented an opportunity to evaluate the efficacy of such anastomosis. So far, only a few researches focused on this issue.3,6,10,11 However, the available literature fails to demonstrate the superiority of stapled over traditional hand-sewn techniques by RCT studies, also not taking into consideration the matching of different stapler model size and the diameter of intestines in neonatal intestinal atresia.
In our study, the EC60A endoscopic linear cutting stapler was used as the stapling device, which consisted of two parallel anvils. The guarantee of successful anastomosis was the smaller anvil of the stapler, which was enough to fit into the atresia of distal intestinal canal. Before anastomotic operation, the diameter of the atresia distal intestine needed to be evaluated by inserting catheter 22, which required the diameter of intestinal canal at least exceeding 1.0 cm.
When the diameter of intestinal lumen in distal bowel was <1.0 cm, stapled anastomosis was not performed, but hand-sewn was used for intestinal anastomosis. In our study, 5 premature patients diagnosed with type III b intestinal atresia presented with “apple peel” defects of the mesentery. During the operation, we found that their intestinal canal was <1.0 cm. We changed the anastomotic methods to hand-sewn anastomosis temporarily. Therefore, the stapled anastomosis should be carefully selected for type III b intestinal atresia.
The anastomotic complications presented as anastomotic leak, stricture, and bleeding in this study were the most important primary outcomes. The type and model aspects of the stapled intestinal anastomoses are important factors affecting the anastomotic effect. In our study, we used endoscopic linear cutting stapler with opened-form 2.6 mm staple height or closed-form 1.0 mm staple height as the only stapling device, which limited the popularization of stapler in all types of intestinal atresia.
Glenn et al. 2 reported that the 5 mm stapler was designed for small bowel anastomosis in animal model. However, it was not popularized and commonly applied in China. Hintz et al. 3 performed the endoscopic cutter with three rows of 3.5 mm and two rows of 3.8 mm staple for pediatric intestinal anastomosis, 1 of the patients occurred anastomotic leak. Aforementioned research results suggest that the height of staple was an important factor affecting the occurrence of anastomotic leak and bleeding.
Previous studies identified no anastomotic leak when endoscopic cutting stapler with opened-form 2.5 mm staple height or closed-form 1.0–1.5 mm staple height were used.3,8,11 The researcher found that the thickness of intestinal wall increased with age. 12 The mean thickness in the small bowel were from 0.7 to 1.1 mm, and the mean thickness in the large bowel were from 1.0 to 1.4 mm. 12 In our study, we found the wall diameter of the expanded and thickened proximal bowel could reach 1.5 mm, and the wall diameter of the distal bowel was only 0.7 mm in intestinal atresia. Therefore, we recommend that endoscopic cutter with three rows of 2.6 mm staples height for intestinal atresia was safe with no anastomotic leak occurred in our study.
Many researchers indicated that resection of proximal dilated and atretic bowel with primary end-to-end anastomosis with or without tapering enteroplasty of the proximal bowel could reduce the incidence of anastomotic stricture.13,14 The difference in the diameter of the proximal and distal intestinal canal, and the reduction of interstitial cells of Cajal in the proximal and distal atretic ends of intestinal atresia 15 were the main reasons of anastomotic stricture. Studies reported that one of the reasons for stricture was a staple line that was either too long, precipitating torsion or too small, leading to a part stricture and proximal dilation. 16
Some researchers recommended that the stapled anastomotic length should be wider than the minimum lumens, but no longer than twice the maximum of the lumens.6,16 In our study, we resected the proximal dilated intestine about 5 cm, using the EC60A endoscopic linear cutting stapler to expand the anastomotic diameter to 1.5 cm, resulting in a staple line to be 30 mm, which exceeded the diameter of hand-sewn anastomosis. After the aforementioned treatment, no patients occurred anastomotic torsion caused by staple line too long found in reoperation.
We found anastomotic bleeding was rare with stapled treatment; however, it was usually cured without any invasive intervention. 5.1% patients presented anastomotic bleeding in the stapled group with colocolostomy in our study, was significantly lower than other study, 16 speculating the reason was that the bleeding in the stapled group had a history of neonatal necrotizing enterocolitis. 16 This suggested that the reasons of bleeding might be due to the patients' original pathology rather than the type of anastomosis accepted.
Although the risk of bleeding did not increase in the stapled group compared with the hand-sewn group, 2 patients with colon atresia occurred anastomotic bleeding in stapled anastomosis, which presented to be blood streak in stool. We found that 2.6 mm staple was not completely closed to the colonic wall tissue, owing to the wall diameters in proximal and distal large bowel in colon atresia were thinner than the dilated jejunum. In addition, the inflammatory stimulation caused by foreign bodies of staple may lead to long-term bleeding at the anastomosis. Therefore, we suggest that the 2.0 mm staple or even smaller staple are suitable for colon anastomosis.
Bowel obstruction was the main complication and the main cause of reoperation during follow-up. In the early stage of our study, there were 2 patients presented with bowel obstruction during postoperative follow-up. X-ray and reoperation surgical field showed significant dilation of the proximal anastomosis. We suggest that the resection of the dilation proximal intestine, to keep the diameter of the lumens on both sides of the anastomosis as consistent as possible.
Jackson et al. 17 detailed 2 patients who had partial bowel obstruction related to dilation in the proximal limb undergoing a stapled side-to-side anastomosis. Studies reported that a stapled side-to-side functional end-to-end anastomosis may be easy to expand anastomosis, possibly because it can produce a “pouch.” 10 It seems reasonable that creating an overly long stapled anastomosis may be prone to stagnation and subsequent expansion.
Unfortunately, three neonates died of pulmonary and abdominal infections complications. We should be more attentive to the prevention of perioperative pulmonary complications, and the gut nutritional function for some premature or low weight children with intestinal atresia. For some neonates in a critical condition, ostomy creation with secondary anastomosis may be used to obtain better curative effect.
This study had several limitations. If the diameter of distal intestine was not suitable for stapled anastomosis, the patient would be transferred to the hand-sewn group. Second, stapled anastomosis was performed by 3 surgeons at our institution, there may be factors that influenced the decision to operative technique. Next, similar to the other pediatric surgery, this is an initial and single institution report that may have limited generalizability. Further study, ideally multicenter study, and appropriate size staplers are needed to extend these findings.
Conclusions
In summary, our results show that stapled anastomosis is safe and effective for intestinal atresia, as it can shorten operative time, with decreased intraoperative duration, early return of peristalsis, early start of feeds, and shorter duration of hospital stay. We also conclude that the weight of neonates is not a limitation for using endoscopic linear cutting stapler.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Fund of the Department of Guizhou Science and Technology of China (No. 20204Y005).