
Abstract
Background:
There are two approaches to single-incision laparoscopic appendectomy (SILA): intracorporeal (Intra) and extracorporeal (Extra). However, the differences in the efficacy between these procedures remain unclear. Thus, this systematic review and meta-analysis aimed to compare the safety and usefulness of these techniques with those of conventional laparoscopic appendectomy (CLA) in children.
Methods:
A systematic literature search was performed using the PubMed, CENTRAL, and Scopus databases. Studies comparing outcomes of “Intra-SILA and CLA” or “Extra-SILA and CLA” in children aged <18 years were included. Operative time, hospitalization duration, wound infection, intra-abdominal infection, conversion to open, additional ports, and narcotic doses were evaluated.
Results:
Overall, 20 studies (six randomized controlled trials [RCTs], one prospective non-RCT, and 13 retrospective cohort studies) (Intra-SILA: 322, CLA: 791 cases; Extra-SILA: 1318, CLA: 1313 cases) were included. Compared with CLA, Extra-SILA was associated with a shorter operative time (mean difference, −9.79 minutes; 95% confidence interval [CI], −18.34 to −1.24) and lower incidence of intra-abdominal infection (3.3% versus 4.6%, odds ratio [OR], 0.52; 95% CI, 0.33 to 0.82) and a higher rate of additional port (13.6% versus 0%, OR, 43.93; 95% CI, 14.79 to 130.50). Meanwhile, the outcomes of Intra-SILA were comparable with those of CLA. However, the participants in the Intra-SILA group received significantly lower doses of narcotics than those in the CLA group.
Conclusion:
Although the evidence was insufficient, both Intra- and Extra-SILA were comparable to CLA with respect to safety. Extra-SILA seems to have an advantage of a shorter operative time, but additional ports may be required.
Introduction
Laparoscopic appendectomy is preferred over open appendectomy in children owing to its lower incidence of surgical site infection, shorter hospitalization duration, and shorter time to oral feeding.1,2 Conventional laparoscopic appendectomy (CLA) has been performed using three laparoscopic ports as the reference standard.
The use of single-incision laparoscopic appendectomy (SILA) has gradually become widespread with the development of minimally invasive surgery.3–5 SILA is potentially less invasive and may accelerate recovery because it results in fewer wounds and lesser abdominal wall destruction than CLA. Furthermore, SILA has good cosmetic satisfaction as it eliminates scars, thus making it particularly useful in children. 6 However, SILA is yet to be established as a superior modality to CLA in children because of its longer operative time7–9 and higher incidence of wound infection. 10
There are two surgical techniques for SILA. First is the intracorporeal approach of SILA (Intra-SILA), which uses three ports through an umbilical incision and resects the mesoappendix and appendix intracorporeally, similar to the CLA procedure. 3 Second is the extracorporeal approach of SILA (Extra-SILA), which uses a laparoscope and one or two forceps through an umbilical incision to grasp and mobilize the appendix to the umbilicus. Then, the appendix is resected outside the abdominal cavity as in the open procedure.4,5 This technique is also known as transumbilical laparoscopic-assisted appendectomy.
The previous meta-analyses did not clearly distinguish between the two approaches of SILA. Outcomes may differ between Intra- and Extra-SILA as they are quite different techniques. A recent retrospective cohort study that directly compared between the Intra- and Extra-SILA approaches reported that Extra-SILA has a shorter operative time and lower complication rate. 11 Therefore, this systematic review and meta-analysis aimed to compare the safety and usefulness between Intra- and Extra-SILA in children. Toward this goal, specified outcome measures of these techniques were compared with those of CLA.
Materials and Methods
Protocol registration
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 12 The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO, registration no. CRD42021244341). The need for institutional review board approval was waived because of the systematic review nature of this study.
Search strategy
A systematic literature search was performed using the PubMed, Cochrane Central Register of Controlled Trials, Cochrane Library (CENTRAL), and Scopus databases for articles published between January 1, 1988, and March 31, 2021. There were no limitations on the language of the publication. The following search terms were used: (child* OR pediatric OR paediatric OR adolescent) AND (append*) AND (laparoscop*) AND (single incision OR single site OR single port OR single access OR single trocar OR single wound OR one incision OR one site OR one port OR one access OR one trocar OR one wound OR transumbilical).
The reference lists of the included studies were also reviewed. The search strategy was confirmed by the clinical research expert of the Clinical Research Support Center at Kagawa University Hospital. Two reviewers (T.F. and A.T.) independently assessed the abstracts and full texts of all potentially relevant studies. Any disagreements were resolved by discussion between the 2 reviewers or with a third reviewer (R.S.).
Study selection
The inclusion criteria were as follows: (1) studies including pediatric patients aged <18 years who underwent laparoscopic appendectomy, (2) studies comparing “Intra-SILA and CLA” or “Extra-SILA and CLA,” and (3) studies with availability of at least one measurable outcome. The exclusion criteria were as follows: (1) studies in which the Intra- and Extra-SILA were not clearly distinguished; (2) animal study, review, letter, case series, or case report; and (3) duplicate publications or studies that contained the same patient group previously reported (in this case, we chose the most meaningful study).
Data extraction
Data on the characteristics of the study (study design, first author, country, year of publication, and sample size), patients (age, body weight, body mass index, and severity of appendicitis), and clinical outcomes were extracted. Complicated appendicitis was defined as gangrenous appendicitis, perforated appendicitis, or abscess formation. The outcome measures were the operative time, hospitalization duration, wound infection, intra-abdominal infection, conversion rate to open appendectomy, the rate of additional ports, and doses of narcotics. Data were extracted by 2 independent reviewers (T.F. and A.T.). After completing the data abstraction, disagreements were resolved through discussion.
Quality assessment
The quality of the included randomized controlled trials (RCTs) was evaluated using the Cochrane risk-of-bias tool for randomized trials (RoB 2). 13 Meanwhile, the quality of the nonrandomized studies of interventions was evaluated using the risk of bias in nonrandomized studies of interventions tool. 14 Each study was evaluated by 2 independent reviewers (T.F. and A.T.). The disagreements were resolved through discussion.
Statistical analysis
The mean differences (MDs) with 95% confidence intervals (CIs) were calculated for continuous variables. For continuous variables with different measurement scales in different studies, the standardized mean differences (SMDs) with 95% CIs were calculated. If the mean and standard deviation (SD) were unavailable, data for median and interquartile range or range were extracted and converted to means and SDs using the well-established method by Wan et al. 15 Odds ratios (ORs) with 95% CIs were calculated for dichotomous variables. Interstudy heterogeneity was assessed using the chi-squared test and was quantified using the I2 statistic. If the I2 value was <50%, a fixed-effects model was applied; otherwise, a random-effects model was applied. All statistical analyses were performed using Review Manager 5.4 software (Cochrane Collaboration, Oxford, United Kingdom). A P-value of <0.05 was considered significant.
Results
Study characteristics
A total of 884 studies were identified during the initial search (Fig. 1). After excluding the duplicates and screening the titles and abstracts, 51 studies remained. Of these, 31 studies were further excluded after a full-text review because the study included adults (n = 10), nonrelevant procedures or results (n = 10), did not clearly distinguish Intra- and Extra-SILA (n = 4), were noncomparative studies (n = 3), contained the same patient group (n = 2) and case series (n = 1), and had unavailable full text (n = 1). Finally, 20 studies (3744 cases) were included in the meta-analysis.3,4,16–32 Of these, six studies were RCTs, one was a prospective non-RCT, and 13 were retrospective cohort studies.

PRISMA flow diagram of this meta-analysis. Extra, extracorporeal approach; Intra, intracorporeal approach; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses; SILA, single-incision laparoscopic appendectomy. Color images are available online.
Table 1 shows the characteristics of the included studies. Intra-SILA was analyzed in nine studies (1113 cases; Intra-SILA: 322 cases, CLA: 791 cases), while Extra-SILA was analyzed in 11 studies (2631 cases; Extra-SILA: 1318, CLA: 1313 cases). In seven studies, severe cases (e.g., complicated appendicitis, diffuse peritonitis, or seriously compromised condition) were excluded.16,18,19,22,25,27,32 In three studies, there were significantly more severe cases in the CLA group than in the SILA group.23,26,31 Conversely, in one study, the SILA group had significantly more severe cases than the CLA group. 5
Characteristics of the Included Studies
Mean (range); bMean (SEM); cMedian (range); dThe number of perforated appendicitis; eMedian (IQR); fBMI; gMonths; hThe number of peritonitis/abscess; iThe severity of appendicitis was evaluated using appendicitis staging (stage 1; early stage, stage 2; suppurative, stage 3; gangrenous, stage 4; perforated, phlegmonous, or abscess). Data are presented as mean (standard deviation).
CLA, conventional laparoscopic appendectomy; Extra, extracorporeal resection of the appendix; Intra, intracorporeal resection of the appendix; IQR, interquartile range; PNR, prospective non-randomized controlled study; R, retrospective comparative study; RCT, randomized controlled trial; SILA, single-incision laparoscopic appendectomy.
Risk of bias
The quality of the included RCTs was evaluated using RoB 2 (Table 2). There were some concerns regarding bias arising from the measurement of the outcome because the blinding of participants or outcome assessors was unclear or not performed in all but one study.3,19,29,30,32 Table 3 shows the risk of bias assessment in the included cohort studies. Nine studies had a serious risk of bias regarding confounding factors such as disease severity because they did not appropriately control for potentially confounding factors and did not perform statistical analysis.5,16–18,21,23,26,27,31 The other five studies had a moderate risk of bias because they had inadequate methods to control for potentially confounding factors.4,22,24,25,28
Risk of Bias Assessment of the Included Randomized Controlled Trials (ROB 2)
Risk of Bias Assessment of the Included Cohort Studies (ROBINS-I)
Eleven studies had a moderate to serious risk of bias in patient selection because there was no description of how surgical procedures were selected or whether they were determined based on the surgeon's preference.5,16–18,22,23,25–28,31 All studies had a moderate risk of bias in the measurement of outcomes because they were nonblinded.4,5,16–18,21–28,31 Eleven retrospective studies had a moderate risk of bias in the selection of the reported result because there was no evidence of preregistered protocols.4,5,16–18,22–28,31
Outcomes
Operative time
No significant difference was found in the operative time between the Intra-SILA and CLA groups in eight studies (MD, 4.54 minutes; 95% CI, −0.27 to 9.35; P = .060; I2 = 94%) (Fig. 2A).3,18,20,21,27–30 The operative time was significantly shorter in the Extra-SILA than in the CLA group in eight studies (MD, −9.79 minutes; 95% CI, −18.34 to −1.24; P = .020; I2 = 96%) (Fig. 2B).5,16,17,19,24–26,31

Forest plot displaying the operative time and hospitalization duration.
Hospitalization duration
No significant difference was noted in the hospitalization duration between the Intra-SILA and CLA groups in seven studies (MD, −0.13 day; 95% CI, −0.62 to 0.35; P = .59; I2 = 83%) (Fig. 2C).3,18,21,22,27,29,30 In addition, no significant difference was found in the hospitalization duration between the Extra-SILA and CLA groups in seven studies (MD, −0.40 day; 95% CI, −0.92 to 0.11; P = .13; I2 = 93%) (Fig. 2D).5,17,19,24–26,31
Wound infection
The rate of wound infection was not significantly different between the Intra-SILA and CLA groups in all studies (2.8% versus 2.3%, OR, 1.55; 95% CI, 0.67 to 3.59; P = .30; I2 = 0%) (Fig. 3A).3,18,20–22,27–30 The rate of wound infection was also not significantly different between the Extra-SILA and CLA groups in all studies (3.3% versus 3.5%, OR, 0.93; 95% CI, 0.58 to 1.51; P = .78; I2 = 5.0%) (Fig. 3B).4,5,16,17,19,23–26,31,32
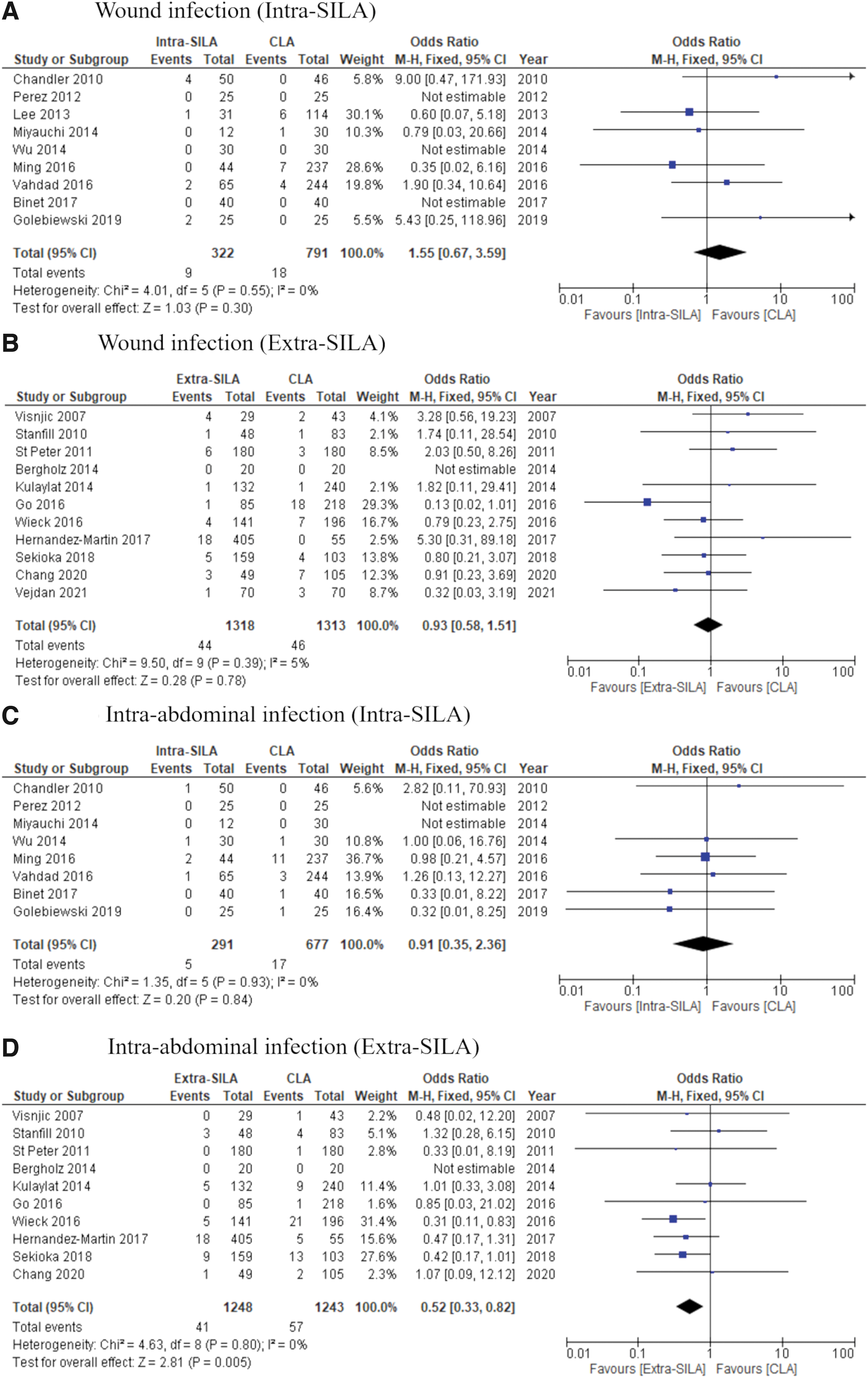
Forest plot displaying the results of wound infection and intra-abdominal infection.
Intra-abdominal infection
No significant difference was observed in the rate of intra-abdominal infection between the Intra-SILA and CLA groups in eight studies (1.7% versus 2.5%, OR, 0.91; 95% CI, 0.35 to 2.36; P = .84; I2 = 0%) (Fig. 3C).3,18,20,22,27–30 The rate of intra-abdominal infection was significantly lower in the Extra-SILA group than in the CLA group in 10 studies (3.3% versus 4.6%, OR, 0.52; 95% CI, 0.33 to 0.82; P = .005; I2 = 0%) (Fig. 3D).4,5,16,17,19,23–26,31
Conversion rate to open appendectomy
All studies compared the conversion rate to open appendectomy between the Intra-SILA and CLA groups (0% versus 0%) (Fig. 4A).3,18,20–22,27–30 Nine studies reported information on the conversion rate to open appendectomy between the Extra-SILA and CLA groups (3.2% versus 0.56%) (Fig. 4B).4,5,16,17,19,23,24,31,32
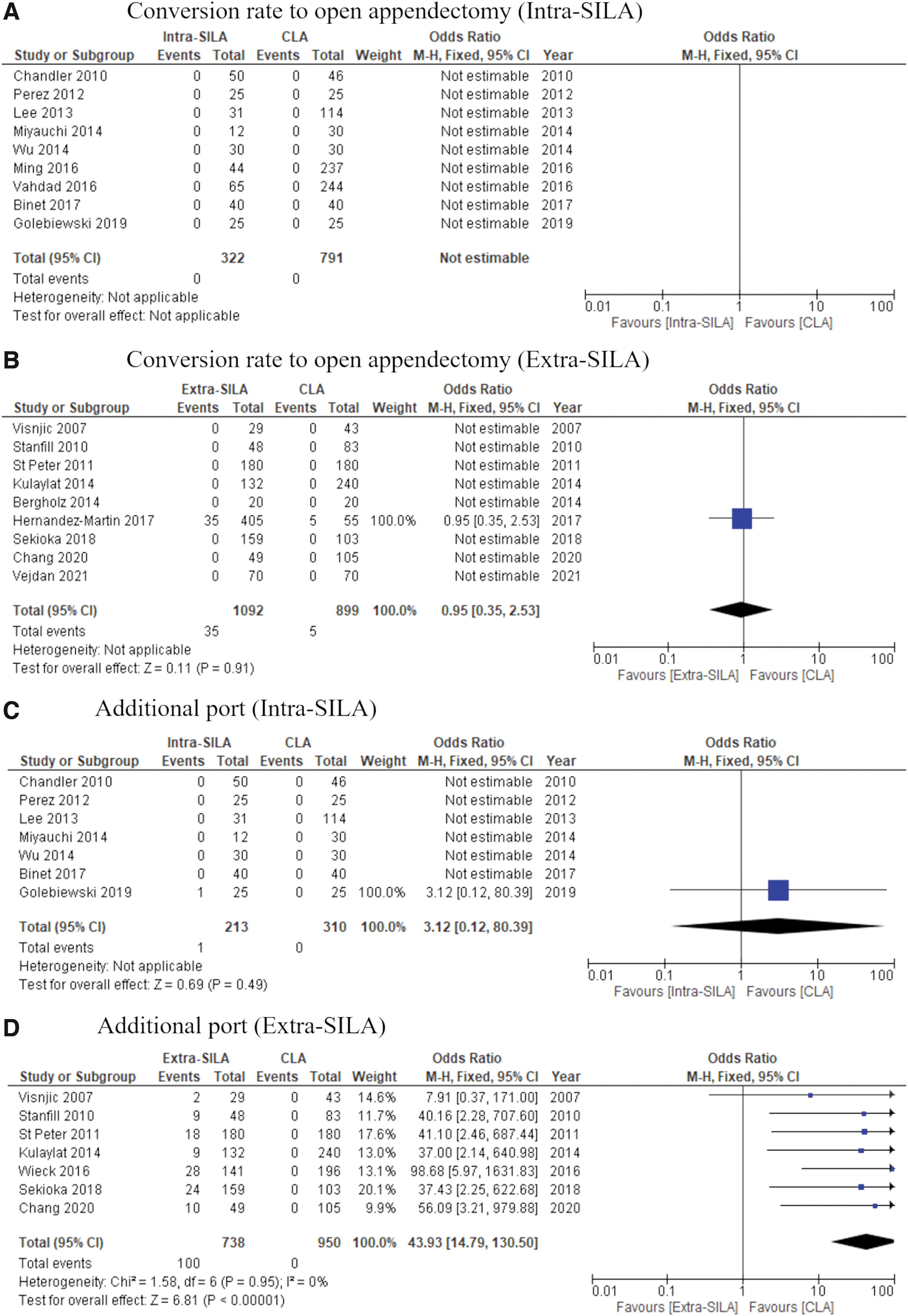
Forest plot displaying the results of conversion rate to open appendectomy and additional port.
Additional port
Seven studies reported comparison of the additional port between the Intra-SILA and CLA groups (0.47% versus 0%) (Fig. 4C).3,18,20–22,29,30 The rate of additional ports was significantly higher in the Extra-SILA group than in the CLA group in seven studies (13.6% versus 0%, OR, 43.93; 95% CI, 14.79 to 130.50; P < .001) (Fig. 4D).4,16,17,19,23,26,31
Doses of narcotics
The doses of narcotics were significantly lower in the Intra-SILA group than in the CLA group in two studies (SMD, −0.52; 95% CI, −0.82 to −0.22; P < .001; I2 = 0%) (Fig. 5A).18,29 No significant difference was observed in the doses of narcotics between the Extra-SILA and CLA groups in two studies (MD, 0.49; 95% CI, −0.46 to 1.45; P = .31; I2 = 74%) (Fig. 5B).5,19

Forest plot displaying the results of doses of narcotics.
Discussion
The safety and usefulness of Intra- and Extra-SILA in comparison to those of CLA are yet to be clarified. This systematic review and meta-analysis found that compared to CLA, Extra-SILA was associated with a shorter operative time and a lower incidence of intra-abdominal infection. However, it was also associated with a higher rate of additional port. Meanwhile, the participants in the Intra-SILA group received significantly lower doses of narcotics than those in the CLA group. The other outcomes of Intra-SILA were comparable to those of CLA.
Previous meta-analyses have reported that SILA required a longer operative time than CLA in children.7–9 In contrast, this study revealed that the operative time was shorter in Extra-SILA than in CLA. In general, Intra-SILA requires high-level surgical skills because instruments tend to clash with each other because of insufficient triangulation, and the same procedure in CLA is performed in the small abdominal cavity of children. Meanwhile, Extra-SILA is a relatively easy procedure because the only procedure in the abdominal cavity is to mobilize the appendix in many cases. 11 In addition, the distance from the cecum to the umbilicus is short, and the abdominal wall is flexible in children, which enables easy exteriorization of the appendix to the umbilicus.33,34
Previous cohort studies that compared Intra- and Extra-SILA have reported shorter operative times in Extra-SILA.11,35 Further, Intra-SILA was found to be an independent factor of a longer operative time. 35 An important advantage of Extra-SILA is that the operative time can be shortened.
However, Extra-SILA was also associated with a higher need for additional ports. This is probably attributed to cases, in which mobilization of the appendix is difficult because of adhesions around the cecum or anatomical fixation to the retroperitoneum. In such cases, some authors converted Extra-SILA to Intra-SILA or performed the “Mix-SILA” procedure, in which the adhesions are dissected, the mesoappendix is resected intracorporeally, and the appendix is resected extracorporeally.34,36 Importantly, if the appendix is severely swollen, there is a risk of iatrogenic perforation when it is exteriorized through the umbilicus. Thus, Intra-SILA instead of Extra-SILA and the use of a specimen retrieval bag are recommended. 35 Therefore, it is important to consider benefits of both Intra- and Extra-SILA based on intraoperative findings to perform the surgery faster and more safely.
There is a potential concern regarding increasing wound infections in SILA. 10 A retrospective study of 1208 cases reported that the incidence of wound infection was higher in the Intra-SILA than in the CLA group. 37 The authors suggested that the result may have been attributed to adverse effects of hypoxia on wound healing caused by excessive traction on the small incision and prolonged procedure. To support the hypothesis, an RCT that compared the surgical trauma between Intra-SILA and CLA reported a higher increase in serum interleukin-6 and C-reactive protein levels in Intra-SILA. 30 Meanwhile, there is a concern that wound infection may occur because of the exteriorization of the infected appendix through the umbilicus in Extra-SILA.
However, a recent meta-analysis of RCTs reported that no significant difference was observed in the rates of wound infection between the SILA and CLA groups. 7 Similarly, in this study, no significant difference was found in the proportion of wound infection between Intra-SILA and CLA or between Extra-SILA and CLA, indicating the safety of both procedures.
The overall rate of intra-abdominal infection was significantly lower in the Extra-SILA group. However, in three studies, the CLA group included more severe cases compared to the Extra-SILA group.23,26,31 This may have been attributed to selection bias and might have affected the outcomes. Meanwhile, the Extra-SILA group in four studies included a sufficient number of complicated appendicitis cases, and no difference was noted in the frequency of intra-abdominal infection.4,5,17,24 Thus, we presume that the rate of intra-abdominal infections in Extra-SILA is equal to or less than those in CLA. However, further studies are needed to verify this.
Postoperative pain was evaluated by various indicators, such as the number of days or frequency of administration of analgesics,4,22,24,30 or pain scales. 30 The number of studies that could be incorporated into this meta-analysis was limited, and the results needed to be carefully interpreted. Conflicting findings have been reported on the postoperative pain of SILA. An RCT conducted by St Peter et al. reported that Extra-SILA needed higher doses of narcotics than CLA. 19 The authors advocated that longer transumbilical incision may lead to more postoperative pain. Similarly, an RCT conducted by Golebiewski et al., reported that patients who underwent Intra-SILA had a higher severe pain score and longer opiate usage than those undergoing CLA. 30
Conversely, an RCT conducted by Vejdan et al. found that Extra-SILA required lesser analgesic use and resulted in smaller size scars than CLA. 32 Moreover, an RCT conducted by Binet et al., showed that the amount of narcotics usage was significantly reduced in Intra-SILA. 29 SILA required a longer operative time compared to CLA in the studies of St Peter et al. and Golebiewski et al., but had a shorter operative time in those of Vejdan et al. and Binet et al.19,29,30,32 Therefore, the intensity of postoperative pain may vary with multiple factors, such as the operative time or size of scar, rather than the difference between the Intra- and Extra-SILA approaches by itself.
This study had some limitations that could affect the generalizability of the results. First, the number of patients in the Intra-SILA group was limited, which may have resulted in insufficient statistical power to detect outcomes. Second, many of the studies included were non-RCTs, and there was an overall moderate to severe risk of bias due to confounding factors or selection bias. Their influence on operative time and postoperative outcome cannot be ignored. Third, there was statistical heterogeneity in operative time and hospitalization duration.
Despite these limitations, to our best knowledge, this study was the first systematic review and meta-analysis to evaluate the efficacy of SILA in children according to its specific type (Intra- and Extra-SILA). A well-designed RCT should be performed to provide a higher level of evidence. Furthermore, given the limited number of studies that directly compared Intra- and Extra-SILA, studies that directly compare their safety and advantages are needed.
Conclusions
Although the evidence was insufficient, this study revealed that Intra- and Extra-SILA have different safety and usefulness profiles; however, both strategies are comparable to CLA with respect to safety. Extra-SILA has an advantage of a shorter operative time, but it may also occasionally require additional ports. Importantly, surgeons should consider conversion to Intra-SILA according to the operative findings.
Footnotes
Authors' Contributions
All authors contributed to the conception and design of the study. Literature search, data collection, and analysis were performed by T.F., A.T., and R.S. The first draft of the article was written by T.F. and R.S., and all authors commented on the previous versions of the article. All authors have read and approved the final article.
Acknowledgment
The authors thank Dr. Jun Kunikata for his useful advice on the systematic literature search.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by JSPS KAKENHI (grant no. JP 20K17555).