
Abstract
Background:
Management of symptomatic pancreatic pseudocysts poses a unique challenge to minimally invasive surgeons. Despite the predominance of endoscopic management of pancreatic pseudocysts, the laparoscopic approach remains a critical skill in the armamentarium of surgeons.
Methods:
This report details a laparoscopic intragastric approach to create a pancreatic cystgastrostomy using intraoperative ultrasound and endoscopy.
Conclusion:
Laparoendoscopic techniques for pancreatic pseudocysts are still required in selective cases when endoscopic management is not available or fails. Using this technique provides patients with same clinical benefits of an endoscopic approach.
Introduction
Pancreatic pseudocysts are a well-known complication of both acute and chronic pancreatitis. Although most pseudocysts resolve spontaneously, symptomatic cysts are treated typically with internal drainage. Historically, this was achieved using an open surgical technique. However, minimally invasive approaches are more common due to advances in endoscopic and laparoscopic techniques. Indications for intervention include gastrointestinal obstruction, bleeding, infection, pain, and rarely rupture. 1 The choice of treatment is dictated by pseudocyst chronicity, potential complications, cyst location, status of the pancreatic duct, and surgeon experience.1,2
Using a stepwise approach, endoscopic fistula creation is usually the initial treatment of choice. However, endoscopic management has limitations and is not always successful.3–5 If an endoscopic approach is not successful or available, minimally invasive laparoscopic approaches may be employed. To date, multiple case reports and small case series exist that describe a laparoendoscopic approach. 6 This report documents a laparoscopic intragastric approach using a stapled cystgastrostomy with concomitant endoscopy and intragastric ultrasound.
Methods
A 66-year-old male presented with diffuse abdominal pain. His medical history included hypertension, prostate cancer status postradiation therapy, and polysubstance abuse including alcohol dependence for ∼40 years before sobriety in 2011. During the 1980s and 1990s, he reported multiple episodes of pancreatitis from heavy drinking that required several hospital admissions. Each admission was treated nonoperatively with intravenous fluids. In 2019, the patient noted unintentional weight loss, early satiety, and vague abdominal pain. A computed tomography (CT) of the abdomen demonstrated pancreatic atrophy and diffuse coarse calcifications throughout the pancreas consistent with chronic pancreatitis.
In addition, there were two cystic masses: one in the head measuring 4.2 × 4.7 cm and the other in the body measuring 2 × 1.9 cm. Subsequently, magnetic resonance imaging (MRI) revealed main pancreatic ductal dilatation to 1.5 cm in diameter with a pancreatic head cyst that was 5.6 cm in diameter without septations, mural nodules, or debris. The patient continued to abstain from alcohol, and surveillance MRI 1 year later demonstrated that the cyst in the pancreatic head had increased in size to 9.3 × 6.9 cm with a mass effect on the gastric antrum. The patient was lost to follow-up for 1 year.
He returned 1 year later with similar complaints of weight loss, abdominal discomfort, early satiety, and intermittent nausea and vomiting. Repeat imaging showed an increase in the cystic pancreatic head lesion to 8.8 × 9.3 cm (Fig. 1). Due to the increase in size, associated mass effect, and dilated pancreatic duct, an endoscopic ultrasound (EUS) was performed that demonstrated extrinsic compression of the posterior stomach wall, pancreatic atrophy with multiple calcifications, a dilated pancreatic duct to 1.5 cm, a 1.8 cm cyst in the pancreatic tail, and a large cyst in the pancreatic head measuring 9.5 × 9.7 cm without septations, mural nodularity, or debris. After discussing the case in a multidisciplinary conference and the patient, an endoscopic cystgastrostomy was recommended.
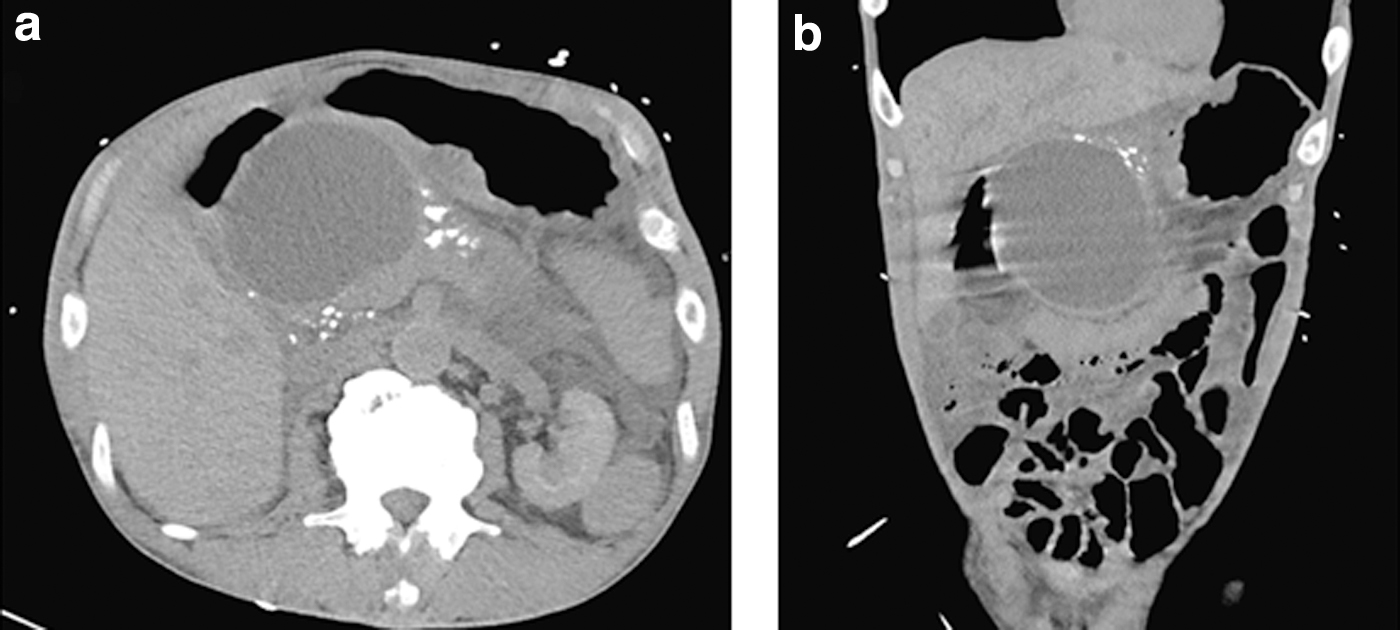
Preoperative computed tomography of abdomen/pelvis demonstrating a large pseudocyst in the pancreatic head and pancreatic calcifications.
At the time of the endoscopic procedure, a 9 cm cyst was identified posterior to the distal antrum consistent with CT imaging (Fig. 2). A cystotome system was advanced and access into the pancreatic cavity was achieved with a 6F catheter. Cystic fluid was aspirated, and a guidewire was advanced through the system and looped inside the cavity. A 10F catheter was advanced toward the cavity, however, the approach became unstable and the cystotome catheter appeared to migrate outside the cystic cavity. EUS identified extraluminal fluid and air and the endoscopic procedure was aborted. At this point, a laparoendoscopic cystgastrostomy was recommended.

Preoperative computed tomography of abdomen/pelvis, sagittal view demonstrating proximity of cyst wall to the posterior stomach.
The room setup is shown in Figure 3. The abdomen was entered using a Hasson technique through an infraumbilical incision and a pneumoperitoneum of 15 mmHg with carbon dioxide was established. Diagnostic laparoscopy did not discern any evidence of abnormal pathology and the pneumoperitoneum was reduced to 8 mmHg. A 5 mm balloon tipped trocar was placed along the subcostal region through the abdominal wall. Endoscopy was then performed that easily documented the location of the pseudocyst at the distal aspect of the antrum. Excellent endoscopic one-to-one congruence was obtained by palpating directly below the costal margin.

Room setup and port placement. Color images are available online.
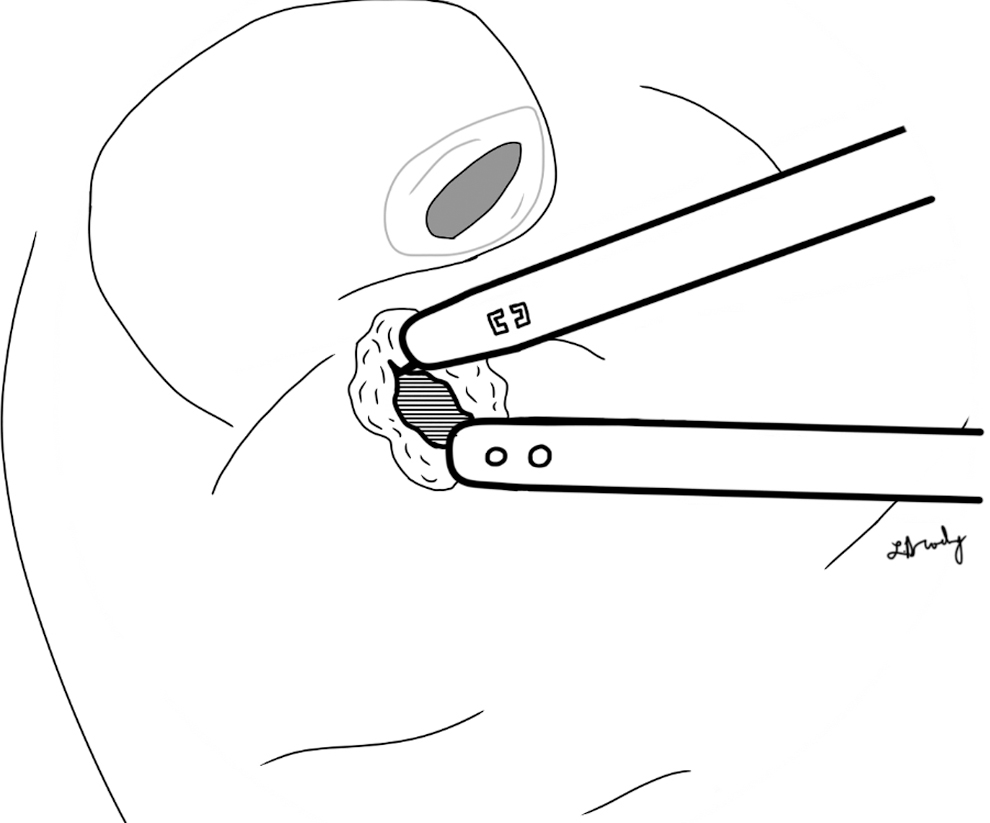
A hook cautery was introduced through the 5 mm port and scored the serosa of the stomach along the greater curvature that correlated with the endoscopic view. The balloon-tipped trocar was then inserted directly through the gastric wall at the scored area. The balloon was inflated and tightened to pull the stomach anteriorly and temporarily tack it to the abdominal wall (Fig. 4). The placement of the laparoscopic ports through the gastric wall was facilitated by decreasing the laparoscopic insufflation pressure while simultaneously increasing the intragastric endoscopic insufflation. This process was performed again for one more 5 mm and one 12 mm balloon tipped trocars.

The stomach is secured to the abdominal wall using balloon tipped trocars.
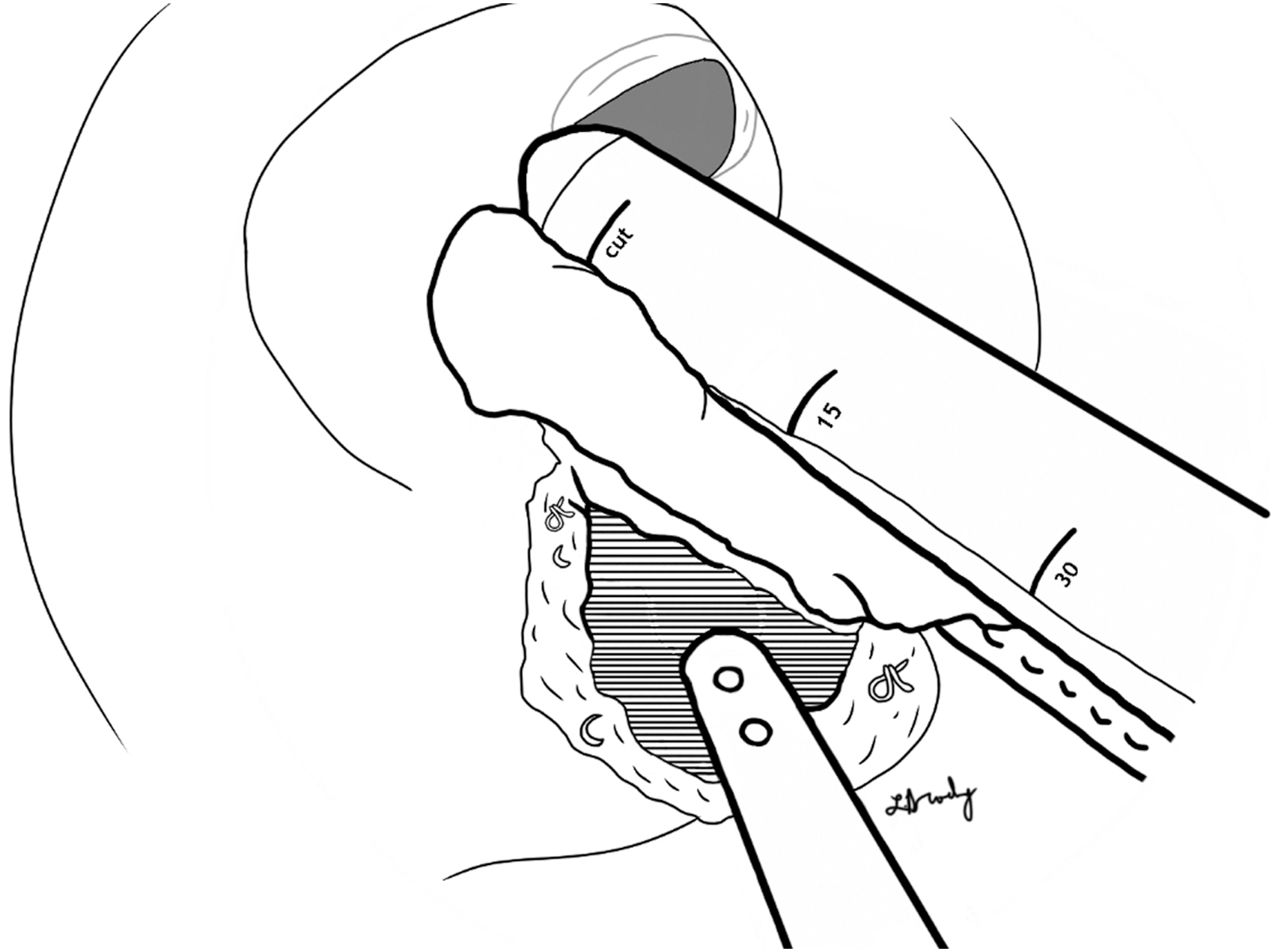
Once the transgastric ports were placed, the pneumoperitoneum was desufflated completely and the insufflation was connected to an intragastric port and maintained at 10 mmHg. Intragastric ultrasound confirmed the location and borders of the pseudocyst and electrosurgery was used to mark the pseudocyst (Fig. 5). The cautery was then used to directly puncture the posterior gastric wall and enter the pseudocyst cavity. The cystgastrotomy was extended bluntly using the hook cautery and suction catheter, making a space large enough to accommodate the linear cutting stapler (Fig. 6). The 45 mm blue load (3.5 mm staples) laparoscopic linear cutting stapler was inserted into the cystgastrostomy and deployed.

The pancreatic pseudocyst is identified using intragastric ultrasound.
Cautery and suction are used to enter and widen the cystgastrostomy.
Subsequently, four reloads were utilized to create a 4 cm wide cystgastrostomy (Figs. 7 and 8). The cyst and its contents were irrigated, and debris was removed. The staple line was reinforced using 2–0 Vicryl sutures to ensure hemostasis (Fig. 9). The balloon tipped trocars were removed from the stomach and the gastrostomies were closed sequentially using the laparoscopic stapler. The fascia was closed at the Hasson and 12 mm port sites along the abdominal wall.
Laparoscopic staplers are used to widen the cystgastrostomy toward antrum.

A final stapler reload is used to resect the final piece of the cystgastrostomy.

A completed cystgastrostomy with clips and sutures to ensure hemostasis.
The patient was advanced to clear liquids on postoperative day (POD) 1 and a regular diet on POD 2. The patient was stable for discharge on POD 2. The patient continues to abstain from alcohol and remains asymptomatic at 6 months postoperatively. Postoperative imaging demonstrates resolution of the pseudocyst (Fig. 10).

Six months postoperative CT of abdomen/pelvis demonstrating absence of the pseudocyst.
Discussion
Laparoscopic management of pancreatic pseudocysts has been utilized for approximately 20 years.1,4 Multiple approaches are necessary to treat pancreatic pseudocysts or walled off necrosis, since these lesions may be located in anatomically difficult positions. Due to the complexity of pancreatic pseudocysts, a one-size fits all approach may not account for the diversity in pathology. Despite advances in endoscopic equipment and highly skilled endoscopists, endoscopic management may fail in certain patients or hospital systems where this highly specialized skill set is not available. In addition, cysts with thick internal debris may not be amenable to an endoscopic procedure.
The debris may simply clog the small stents, or the tiny endoscopic instruments may not be strong enough to debride the tenacious material of some pseudocysts. As well, some cysts may be located along the distal aspect of the pancreatic tail and may not be amenable to endoscopic drainage. Also, some patients may have a higher risk of bleeding and a laparoendoscopic approach affords multiple resources to manage this risk. For example, patients with gastric varices may not warrant an endoscopic approach. Finally, some patients with persistent inflammation may have a pseudocyst wall that is too thick to penetrate endoscopically.
The laparoendoscopic approach is recommended as a step-up procedure in instances when a purely endoscopic approach has failed, is not available, or is simply not suitable. The value of the laparoscopic component lies in the ability to mitigate complications, specifically bleeding. Using laparoscopic staplers enables the surgeon to place three rows of well-conformed staples for hemostasis. In addition, the laparoscopic access allows the surgeon to apply surgical clips or oversew areas with persistent oozing or frank bleeding. The intragastric component improves visualization as the procedure is performed directly inferior to the intragastric ports and minimizes the size of the gastrotomy.
A purely laparoscopic approach usually entails a much wider gastrotomy to accurately identify the pseudocyst and perform the necessary drainage. Placement of the intragastric ports may be one of the more difficult steps of this technique. This aspect of the procedure is facilitated by decreasing the pneumoperitoneum and scoring the gastric serosa. In addition, the stomach may be sutured or tacked to the abdominal wall before inserting the intragastric balloon-tipped trocars. Finally, intraoperative ultrasound is useful to enhance and define the cyst anatomy and ultimately determine the optimal location for cystgastrostomy.
Footnotes
Authors' Contributions
All persons who meet authorship criteria are listed as authors and all authors certify that they have participated sufficiently in the study to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in the Journal of Laparoendoscopic and Advanced Surgical Techniques.
Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
The authors received no specific funding for this study.