
Abstract
Purpose:
It is unclear whether the principles of open complete mesocolic excision (CME) can be safely applied to laparoscopic surgery. Furthermore, definitions vary over how radical optimal CME surgery should be. We report morbidity and oncological outcomes for laparoscopic CME without routine gastro-pancreatico-colic trunk (GPCT) dissection.
Materials and Methods:
An observational study with consecutive data for patients with Union for International Cancer Control (UICC) stage I–III colon adenocarcinoma who underwent elective laparoscopic resection between 2006 and 2015. Data were retrieved for demographics, tumor characteristics, treatment, and histology from prospectively maintained databases. Standardized, routinely video recorded, laparoscopic resections were performed in two United Kingdom centers from The National Training Programme for Laparoscopic Colorectal Surgery. Overall survival and disease-free survival (DFS) were reported using Kaplan–Meier curves and Cox regression.
Results:
Laparoscopic CME was performed in 567 patients, 52.7% (288/546) women, median (interquartile range [IQR]) age 73 (65–80) years. Median (IQR) length of stay was 4 (3–5) days with 4.0 (2.2–5.7)-year follow-up. Significant DFS predictors (hazard ratio [HR]) by multivariable Cox regression were age >80 years (1.9), American Society of Anesthesiologists (ASA) 3 and 4 (HR = 1.1), right colon cancer (1.7), UICC stage III (3.4), and intramesocolic grade (2.2). Overall 4-year DFS (95% confidence interval) was 81.3% (77–85). Four-year DFS by UICC grades I, II, and III was 94.6% (89–99), 83.4% (77–88), and 72.2% (66–78), respectively (log-rank P = .001). Morbidity by Clavien–Dindo grade was III 18 (3.2%), IV 4 (0.7%) and V 7 (1.2%).
Conclusion:
This large series suggests standardized laparoscopic CME without routine GPCT dissection has a low morbidity and achieves equivalent outcomes to the most radical open CME techniques.
Introduction
Colorectal cancer (CRC) is the fourth leading cause of cancer death worldwide. 1 In Europe it remains the third commonest cancer, with ∼432,400 new cases diagnosed in 2015. 1 Rectal cancer survival has markedly improved over the past three decades; however, outcomes for colon cancer have essentially been static. 1 Adjuvant chemotherapy has the potential to decrease disease recurrence for patients with stages II and III colon cancer,2,3 but radical surgery is the only curative treatment modality.
The key reason for the considerable improvement in rectal cancer survival is total mesorectal excision (TME), 4 a surgical technique popularized by Professor Heald, that allows complete removal of the rectum and, potentially metastatic, lymph nodes of the mesorectum. 5 The effectiveness of this technique is attributed to the ontogenetic compartment concept whereby tumor permeation is constant or “isotropic” within a permissive embryological compartment, but it is suppressed at the compartment border. 6 National training programs effectively trained surgeons to preserve the mesorectal embryological plane, which maximized node yield, minimized the risk of residual disease significantly, and improved cancer-related death rates. 4
This principle has been applied to colon cancer surgery through complete mesocolic excision (CME). 7 CME dissection is performed in the embryological mesocolic plane to create an intact envelope of mesocolic fascia, and all lymph nodes along the tumor supplying vessels are contained in the specimen. 7 Single center studies that apply this technique have demonstrated survival benefits.7,8 Bertelsen et al. reported superior oncological results for a center performing CME over other regional centers performing non-CME surgery (4-year disease-free survival [DFS]—CME 86% versus non-CME 76%, P = .0010) 8 ; however, relatively few cases were laparoscopic (n = 179). At present, in the multicenter setting it remains controversial as to whether the morbidity and mortality associated with the technique are justified.9,10 There is debate about how radical the optimal CME dissection should be and Benz and co-workers have produced defined steps as a foundation for a standardized technique. 11
Aim
The purpose of this study was to assess the morbidity, mortality, and long-term oncological outcomes for a standardized laparoscopic CME approach that does not routinely involve gastro-pancreatico-colic trunk (GPCT) dissection.
Materials and Methods
Study design and participants
Consecutive data were prospectively collected for all patients who underwent elective laparoscopic resection for Union for International Cancer Control (UICC) stages I–III colon adenocarcinomas in Poole and Portsmouth Hospitals. These were two United Kingdom NHS hospitals with experience from the National Training Programme for Laparoscopic Colorectal (LAPCO) Surgery and their combined catchment population is 800,000 people. Both institutions employed dedicated staff to prospectively maintained databases. Demographics, tumor characteristics, surgical management, use of chemotherapy, and histology (TNM 5) along with disease and survival status were retrieved for each patient.
Exclusion criteria from published CME studies were applied 8 : UICC stage IV disease, metachronous CRC, rectal cancer (≤15 cm from anal verge) without synchronous colon adenocarcinoma, tumor of the appendix, R2 resections, and patients treated with preoperative chemotherapy.
Hospital governance and ethics review boards approved prospective data collection, analysis, and reporting. The operative procedure was routinely recorded with additional patient consent for medical photography and videoing.
Procedures
All procedures were performed with, or by, 2 trainers (T.Q. and A.P.) who have undergone formal laparoscopic training including a National Fellowship and >90% of their elective practice is laparoscopic. The majority of cases were performed in part or completely by the acknowledged supervised senior colorectal trainees using goal-oriented, targeted teaching methods. 12 Electively, all patients with colon cancer were approached laparoscopically (Fig. 1).

Flow chart of eligible patients.
A laparoscopic right-sided resection included right and extended right hemicolectomies with an ileocolic anastomosis. The remainder of colonic resections were classified as left sided. Subtotal colectomies were defined as left sided when the tumor was distal, or at the level of, the left third of the transverse colon, the remainder was classified as right sided. The resection was classified as laparoscopic if it was not converted at any time.
Standardized, routinely video recorded, laparoscopic resections were performed according to CME principles (LapCME).7,13 The operative technique for right hemicolectomy and extended right hemicolectomy was applied as previously reported. 12 Consistent with the standardized approach recently outlined by Benz and co-workers, 11 (1) the visceral fascia was meticulous preserved without injury to mesocolon; (2) complete removal of the regional lymphatic vessels and lymph nodes; (3) division of the supplying arteries close to their origin (ileocolic artery [ICA], right colic artery, right branch of the middle colic artery); (4) removal of the lymphatic tissue along the right side of the superior mesenteric vein (SMV); (5) preservation of the GPCT including the pancreatic tributaries and the veins that merge into the SMV including right gastro-omental vein and pancreatic veins. However, we did not routinely ligate the anterior colonic branches distal to the ICV at the root of the GPCT.
Left-sided resection were performed according to previously published anterior resection methodology with central inferior mesenteric artery (IMA) ligation 1 cm from the aorta and inferior mesenteric vein ligation at the inferior pancreatic border. 14 TME dissection was only performed to aid mobilization and facilitate safe division and anastomosis with at least 5 cm of clearance distal to the tumor.
Pathological staging was performed according to UICC TNM system (5th edition). 15 The mesocolic plane was assessed as defined by West et al. after 2011, before this surgeon-reported specimen quality was used according to the principles of TME assessment.16,17 In summary the plane was graded: (A) Muscularis propria plane—muscularis propria exposed; (B) Intramesocolic plane—disruption of the mesocolon but the incisions do not reach down to the muscularis propria; (C) Mesocolic plane: smooth intact mesocolic excision. 17 An optimal dissection was defined as an R0 resection in the mesocolic plane. Adjuvant chemotherapy was predominantly offered to UICC III patients and selected UICC II following multidisciplinary discussion.
The oncological outcome was assessed by overall survival and DFS according to standardized definitions. 18 Cancer-related survival (CRS) was defined as death with recurrent locoregional or distant carcinoma; hence, this did not include noncancer deaths. Date of last follow-up was defined as the latest computed tomography (CT) or positron emission tomography/CT of thorax and abdomen and contrast-enhanced ultrasound of the liver, or the last laparotomy in case of suspicion of recurrence. Follow-up was standardized with 6-monthly carcinoembryonic antigen and annual CT surveillance for the first 5 years postsurgery. Colonoscopy was performed within the first postoperative year followed by 3-yearly surveillance. Radiological findings of metastases during follow-up were considered as recurrence even if histological verification was not obtained. Subsequent metachronous colon cancers were recurrences only if located in the anastomosis and with the same morphology as the primary tumor.
Statistical analysis
Continuous data are presented as medians with interquartile ranges (IQRs). Categorical variables were analyzed by Pearson's χ 2 tests and continuous variables by Mann–Whitney U-test. DFS was evaluated with Kaplan–Meier curves and log-rank tests for categorical data, and with univariable Cox proportional hazards regression models for all variables. Multivariable proportional hazards Cox regression models were used with purposeful selection. 19 Possible predictive variables were selected if P-values in the univariable regression models were <.50 based on Wald statistics, and multivariable models were fitted with the variables identified in the univariable analyses. After the stepwise elimination of all variables with P-values of >.10, the reduced Cox regression models were tested one by one with all variables eliminated, and if the tested variable had a P value of <.10, it was included in the final model. The adequacy and fit of the models were checked graphically and with partial residual plots (Schoenfeld test). 20 Clinically relevant interactions including time-dependent interactions were tested.
Results are presented as hazard ratios (HRs) with 95% confidence intervals (CIs). Where 95% CI overlapped oncological outcomes were regarded as equivalent, where no overlap was observed a significant difference in oncological outcome was assumed. Overall survival was analyzed with Kaplan–Meier curves and log-rank test. P values of <.05 was deemed to be significant, but all variables with P values of <.10 are shown in the final Cox regression models. All analyses were carried out using SPSS (version 22: 2013; IBM, NY, USA).
Results
Of 1079 patients who underwent colorectal surgery during the inclusion period, 567 were eligible for inclusion (Fig. 1). Nineteen (3.2%) of 586 patients were excluded owing to open, or conversion to open surgery. Quality indicators were not available in 129 of 567 cases. Optimal surgery was identified in 91.0% (403/443) of cases (suboptimal: 25 [5%], intramesocolic, and 15 [3%]) R1, resections).
CME procedures were undertaken or closely supervised by T.Q. and A.P. in 128 and 439 cases, respectively. Table 1 provides the baseline demographics, tumor characteristics, and surgical procedures performed, and Table 2 provides the data from the pathology reports along with length of stay and morbidity. Tumors from the right and left colon are reported separately.
Baseline Demographics, Tumor Characteristics, and Surgical Procedures Performed
Data are given as median (IQR) [range] or n (%).
Mann–Whitney U-test.
Pearson's χ 2 test.
Missing 34.
Missing 41.
ASA, American Society of Anesthesiologists; ASA 1, normal healthy patient; ASA 2, mild systemic disease; ASA 3, severe systemic disease; ASA 4, severe systemic disease that is a constant threat to life; BMI, body mass index; IQR, interquartile range; LIF, Left Iliac Fossa; LUQ, left upper quadrant; RIF, right iliac fossa; RUQ, right upper quadrant.
Histopathology, Length of Stay, and Morbidity
Mann–Whitney U-test.
R2 were excluded from analysis.
UICC, Union for International Cancer Control.
Adjuvant chemotherapy was given to 27 (10.7%) of 252 patients with UICC stage II disease and 152 (74.9%) of 203 UICC stage III patients, with no variation between the right and left colon. Preoperative chemotherapy was administered to 5 patients, all within FOxTROT trial; therefore, these patients were excluded from analysis (Fig. 1).
The median follow-up was 4.36 years (IQR, 2.68–6.29). Locoregional recurrences occurred in 42 (7.4%) of 567 patients, including 26 of 346 right and 16 of 221 left colonic tumors (7.4% versus 7.5%, respectively, P = .91). Distant recurrences occurred in 71 (12.5%) of 567 patients with no significant difference between right (47 of 346) and left (24 of 221) colonic cancers (13.6% versus 10.9%, P = .33). Locoregional recurrence was reported in 4 (16%) of 25 patients with an incomplete mesocolic excision (odds ratio 3.4 [95% CI, 1.0–10.6], P = .03) and 5 (20%) of 25 developed distant recurrence (P = .6). Recurrences occurred in 2 (1.8%) of 111 UICC stage I patients, 27 (10.7%) or 252 UICC stage II disease, and 42 (20.7%) of 203 UICC stage III disease patients (P < .001).
Overall and DFS are represented by Kaplan–Meier curves in Figure 2A, B . The overall 4-year DFS was 81.3% (95% CI, 77–85). Four-year DFS for right colonic cancers was 76.6% (95% CI, 73–82) compared with 87.3% (95% CI, 83–91) for left colonic cancers (log-rank P = .005; Fig. 2C). Four-year DFS for patients with UICC stage I disease was 94.6% (95% CI, 89–99) compared with UICC II 83.4% (95% CI, 77–88) and UICC III 72.2% (95% CI, 66–78) disease (log-rank P = .001; Fig. 2D). Multivariable Cox regression identified age, ASA, tumor site, UICC grade, and mesocolic grade to be the significant independent predictive factors for impaired DFS (Table 3). Locally weighted scatterplot smoothing lines for each variable were close to the horizontal 0 reference line for the y-axis suggesting an adequate model fit. 19 Multivariable Cox regression indicated that UICC III patients have a three-fold (HR = 3.4 [1.8–6.1]) greater risk of death or recurrence compared with UICC I patients and intramesocolic tumor specimens increased this risk by twofold (HR = 2.2 [1.2–3.8]). The multivariable analysis also reported a significantly lower DFS for right colon cancers (HR = 1.7 [1.1–2.5]).

Overall survival
Univariable and Reduced Multivariable Cox Regression Model Analysis of Disease-Free Survival in All Patients
R2 excluded.
ASA, American Society of Anesthesiologists; BMI, body mass index; UICC, Union for International Cancer Control.
Discussion
This is the largest reported series of laparoscopic colonic resections to be performed according to CME principles (LapCME). The most striking finding from the study is that standardized laparoscopic resections, performed with emphasis on meticulous technique and preservation of the optimal resection plane, have a low morbidity and offer comparable long-term oncological survival to open CME dissection with routine GPCT dissection. Furthermore, the multivariable analysis indicates that impaired DFS is predicted by: being an octogenarian or older; having severe systemic disease, including disease that is a constant threat to life (ASA 3 and 4); a right-sided colon cancer; node-positive disease; and, an intramesocolic dissection.
The laparoscopic technique we practice places fundamental emphasis on standardization, dissection in the embryological plane, and preservation of the mesocolon. Preservation of the mesocolic fascia has been reported as a key determinant of oncological outcome by West et al. and Hohenberger et al. previously.7,17,21 Compromise to the mesocolon was an uncommon event in this series with no recorded cases of muscularis propria exposure and intramesocolic exposure in 16% of cases. Nevertheless, beaching the mesocolic plane was associated with more than a twofold reduction in DFS.
An adequate pedicle length is a key determinant for a favorable oncological outcome. 21 Spasojevic and co-workers used postoperative CT angiograms to highlighted extreme variations in postoperative length of the ICA stump following a right hemicolectomy. 22 In this series, a high ligation, with division of the supplying arteries close to their origin (ICA, right colic artery, right branch of the middle colic artery and IMA), was routinely performed. This standardized approach removed the variation reported by Sposojevic and co-workers and in conjunction with mesocolic plane preservation, facilitated optimal removal of the regional lymphatic vessels that is likely to have contributed to our favorable outcomes.
Some advocate a more radical approach for right hemicolectomy; however, the optimal degree of radicality for vessel ligation and peripancreatic dissection remains unclear.11,23,24 Recently, Benz and co-workers have taken the principles described by Hohenberger and co-workers to define the steps of a laparoscopic “radical CME” and developed the critical view concept for CME. 11 Our approach, described in the methodology, is consistent with the steps outlined by Benz and co-workers; however, we did not routinely ligate the anterior colonic branches proximal to the ileocolic vein (ICV) at the root of the GPCT. Benz and co-workers have developed their approach based on a consensus view of anatomists and experienced surgeons and not on clinical outcomes data per se. They are currently evaluating the morbidity and oncological outcomes in a multicenter trial (DRKS-ID: DRKS00012369) German Consortium for Cancer Research (DRKS) that began recruitment in 2017. 11 We believe that the morbidity and oncological outcome data presented in this series will be an important benchmark for such trials.
The mortality rate of 1.2% in this series was lower than the available data for the open CME technique; Hohenberger et al. and Bertelsen et al. reported a 3.1% and 5% 30-day mortality rates, respectively.7,8 We reported a morbidity rate of 13.9% compared with 19.7% in the Hohenberger series; however, morbidity assessment was not standardized between studies. Bertelsen et al. highlighted significant morbidity for 258 laparoscopic CME cases with routine GPCT dissection compared with 1172 “conventional” laparoscopic resections. CME with routine GPCT dissection was associated with threefold more intraoperative injuries compared with other organs (9.1% versus 3.6%; P < .001), including more splenic (3.2% versus 1.2%; P = .004) and SMV (1.7% versus 0.2%; P < .001) injuries. 25 Small case series have also reported fatal SMV injuries. 26 We believe that avoiding routine GPCT dissection may reduce morbidity from major bleeding and intraoperative organ injury. Our highly selective approach to GPCT dissection may partly explain the favorable morbidity and mortality outcomes in this series.
The 4-year overall survival and DFS results in this study are summarized in Figure 3. The 4-year overall survival of 0.86 and the DFS of 0.81 appear to be significantly better than current population data (Fig. 3) both before and after regional CME surgeon training; however, the population data report right-sided cancers only. 27 The confidence intervals for 5-year CRS outcomes for this series overlaps with the CME cohort (1995–2002) in the original Hohenberger et al. study, which may indicate equivalent oncological outcomes. 7
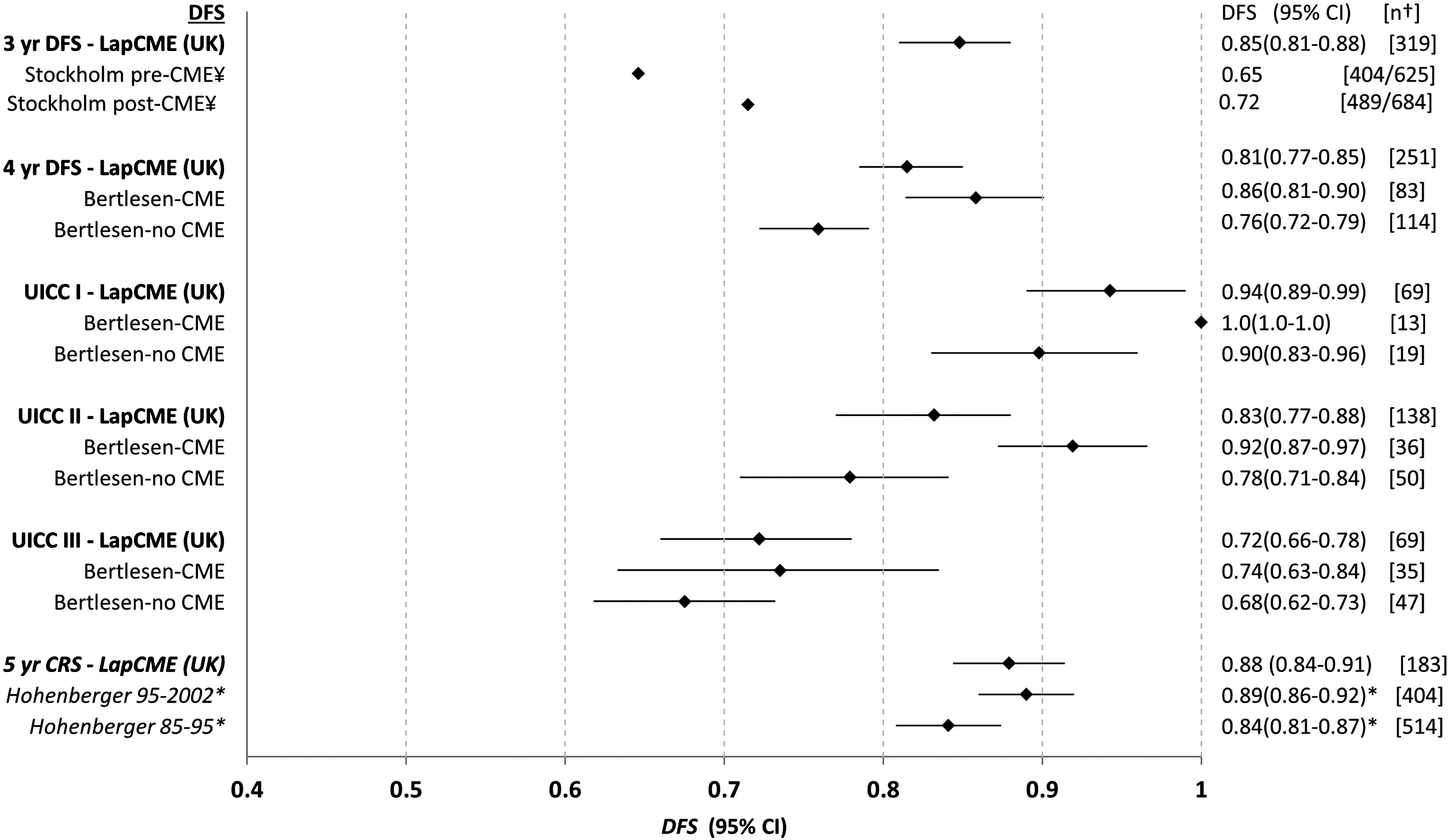
A simple descriptive chart summarizing outcomes from the CME series (Red Diamonds) compared with previously reports DFS outcomes (black diamonds) (95% CI). The DFS outcomes for this laparoscopic CME series are reported at 3–5 years. The 4-year DFS is split according to the UICC grade and compared with data from the Bertlesen study. 8 ¥Stockholm-wide DFS before (January 2001–December 2003) and after (January 2006–December 2008) the “Stockholm Colon Cancer Project”—data are reported for right-sided colon cancers only. 27 *Hohenberger reported CRS rather than DFS. 7 †Number of cases available at the reported time point. CI, confidence interval; CME, complete mesocolic excision; CRS, cancer-related survival; DFS, disease-free survival; UICC, Union for International Cancer Control.
This study also identified a survival discrepancy between right- and left-sided colon cancers. This is demonstrated by Kaplan–Meier survival curve (Fig. 2C). The multivariate analysis for DFS found a 70% (HR = 1.7 [95% CI, 1.1–2.5]) greater chance of recurrence or death for right-sided cancer than left-side colon cancer. Impaired survival for right-sided colon cancer is a well-recognized problem.
Advocates for the most radical CME approach may argue that this survival discrepancy is owing to inadequate GPCT dissection and suboptimal lymph node yield. However, in this study we found no significant difference in locoregional recurrence rates between right- and left-sided cancer resections (7.4% versus 7.5%, respectively) and the lymph node count was significantly higher in favor of right-sided resections. A meta-analysis by Petrelli et al. 28 reported several key contributory factors for the survival discrepancy including a greater median tumor size and immune stimulation by microsatellite unstable tumors. West et al. also described greater anatomical variation between the vascular arcades in right-sided specimens compared with left-sided specimens. 21
Radical CME advocates may also argue this survival difference is an indication for routine CME with GPCT dissection and that radiological staging to preoperatively select high-risk cases in inaccurate. 29 However, there is increasing evidence to suggest CT and magnetic resonance imaging are reliable methods for preoperatively identifying locally advanced tumors 30 and metastatic lymph nodes. 31
Strengths and limitations
The primary aim of this study was to report the oncological outcomes when CME principles were applied to laparoscopic surgery. The inclusion criteria and treatment strategies are similar for comparative studies. 8
Historic laparoscopic studies such as Conventional Versus Laparoscopic-Assisted Surgery in Colorectal Cancer (CLASICC), 32 Clinical Outcomes of Surgical Therapy (COST), 33 and Colon Cancer Laparoscopic or Open Resection (COLOR) 29 have shown equivalent or noninferior oncological outcomes between laparoscopic and open surgery. The major criticism of these studies has been significant case selection and lack of generalizability. 34 The broad inclusion criteria and our flow diagram demonstrate that generalizability is a key strength of this study. The majority of patients were eligible for laparoscopic surgery with elective open surgery or conversion to open in only 2.5% (19/637) of cases.
A.P. was a forerunner in laparoscopic surgery and director of EARCS (European Academy of Robotic Colorectal Surgery) and T.Q. is LAPCO trainer 35 and lead robotic surgeon at an Intuitive Surgical® epicenter. Therefore, generalizability may be limited by exacting standards. However, laparoscopic fellows performed a large proportion of the cases in total or in part. Therefore, with adequate experience and training we believe these results are reproducible.
Conclusion
In the modern era colon cancer survival outcomes have not improved to the same extent as for rectal cancer. The need for standardized optimal colonic resection is widely accepted. To our knowledge this is the largest reported series of laparoscopic colonic cancer resections performed according to CME principles.
We believe that the reported technique is safe and reproducible, enabling standardized, optimal, laparoscopic surgery, that achieves excellent oncological outcomes with a relatively short length of stay and acceptable morbidity. Future work should focus on evaluating whether marginal gains can be achieved with more radical precision surgery in selected radiologically high-risk tumors.
Footnotes
Acknowledgments
The authors thank all the senior fellows who contributed data during their proctorship: Atif Alvi, Robert Clarke, Sudeep Thomas, Adnan Alam, Mohammed Farooq, Danilo Mascovic, Andy King, Laeeq Khan, Manfred Odermatt, Anil Hemandas, and James Bromilow. The authors also thank Janice Jones and Karen Flashman for their rigorous efforts in meticulously following up patients and maintaining the prospective database.
Disclaimer
The funders had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Disclosure Statement
No competing financial interests exist.
Funding Information
The funding sources were The Champalimaud Foundation, University of Portsmouth, and Poole Hospital NHS Foundation Trust provided salaries for the individuals are their respective institution. However, no specific funding or grants were obtained.