
Abstract
Background:
In this preliminary experience, the feasibility and effectiveness of surgical training with an animal model for transanal total mesorectal excision (TaTME) were evaluated.
Methods:
The training was conducted in two experimental animal laboratories in Italy authorized by the Italian Ministry of Health, using female Danish Landrace pigs under the supervision of surgeons with extensive experience in TaTME, animal laboratory training and cadaver laboratory training. The procedure was divided into separate steps, and all the participants were guided step-by-step throughout the entirety of the procedure.
Results:
During all the editions of the animal laboratory, all the procedures were completed with no major damage to the anatomical structures or intraoperative death of the animals. Live animal tissue is very similar to human tissue, helping trainees improve their tactile feedback. The bleeding effect improved the value of the training and taught the participants how to address this complication. The lack of mesorectal tissue in pigs compared with humans was the main difference. Animal laboratories should not be considered alternatives to cadaver laboratories but as complementary training activities due to their effectiveness and lower costs.
Conclusions:
Surgical training in animal models for TaTME seems to be effective and could be an opportunity to improve training alongside the use of a cadaver laboratory and proctoring.
Introduction
Transanal total mesorectal excision (TaTME) is considered one of the main developments in colorectal surgery during the past 10 years, with the potential to improve the quality of surgical mesorectal excision in patients with mid and low rectal cancers.
The execution of this procedure is, however, technically challenging due to the reduced working space, retraction capability, and visibility. In addition, the transanal time requires knowledge of the surgical anatomy in a completely different way than in the standard minimally invasive approach (laparoscopy and robotics).
For these reasons, training pathways have been described, 1 even national structured training programs such as those proposed in the Netherlands; Veltcamp Helbach et al. demonstrated that a structured training program for TaTME delivered safe implementation, even when surgeons had to undergo a learning curve period to improve the surgical outcomes, as demonstrated in other studies. 2
To improve the outcomes of these training programs, especially in terms of practical implications, the cadaveric training model has been purposed to improve the learning curve and provide surgeons with a more complete training package. 3 The cadaveric model was also mentioned at the St. Gallen Consensus Conference on the safe implementation of TaTME. 4
Unfortunately, cadaveric laboratories are not as widespread in European universities and hospitals, and the cost of this kind of training is high.
This preliminary study aims to describe the experience of two experienced colorectal centers involved in training programs on TaTME using animal model training as a complementary activity to cadaveric training.
Materials and Methods
Study design and outcomes
In this preliminary experience, the feasibility and effectiveness of training with an animal model for TaTME were evaluated. The experience was planned, developed, and conducted in the wet laboratory of two Italian high-volume centers with early and substantial experience with the TaTME technique: Fondazione Policlinico “A. Gemelli” IRCCS in Rome 5 and Ospedale San Raffaele, IRCCS in Milan. 6
The training experience was included in the theoretical–practical course on TaTME for colorectal surgeons under the supervision of 2 experts in TaTME: Prof. R. Persiani (Rome) and Prof. U. Elmore (Milan).
Wet laboratory
The training was conducted in experimental animal laboratories authorized by the Italian Ministry of Health and its ethics committee. The animals involved were female Danish Landrace pigs weighing 55–60 kg and were placed under general anesthesia and deep pain control, as assisted by an authorized veterinary anesthesiologist. The animals were sacrificed at the end of the procedure.
The wet laboratory was conducted with 4 animals, with 2 trainees for each animal. Every team was supervised by an expert colorectal surgeon with previous experience in the animal laboratory. The entire experiment was supervised by Prof. R. Persiani in Rome and Prof. U. Elmore in Milan.
The anastomosis construction step was performed only in Ospedale San Raffaele, IRCCS in Milan, because it was initially not included in the training program at Fondazione Policlinico “A. Gemelli” IRCCS in Rome.
Compliance with ethical standards
All procedures were previously authorized by the Animal Health Organization, within the University, and by the Italian Ministry of Health and were implemented in compliance with the provisions laid down by the Legislative Decree N. 26/2014 (implementation of the European Directive 63/2010).
The animals were maintained under deep general anesthesia and complete analgesia for the entire duration of the surgical intervention in accordance with current laws. Euthanasia was performed at the end of the procedures with the animal under general anesthesia.
Instruments
Every surgical table was equipped with an HD laparoscopic rack connected to a 30° scope. A standard insufflator was used with an insufflation pressure of 14 mmHg. The transanal port (Gel Point Path, Applied Medical) was used and connected to the insufflator with a reservoir bag to stabilize the insufflation air flow.
Every surgical table was equipped with one monopolar laparoscopic hook, one laparoscopic johann, one laparoscopic needle-driver, basic surgical instruments for open surgery, Prolene 0 and Silk 1 stitches, lubricant and sponges, as shown in Figure 1.

Surgical instruments. Color images are available online.
Surgical Steps
Port installation
The transanal port was installed and blocked with two Silk 0 stitches in the skin of the animal. Before installing the port, a wet sponge was deeply inserted into the anus of the animal to clean the rectum and limit air insufflation into the bowel. Limiting air insufflation into the bowel of the animal decreased abdominal distention and systemic effects. It also provided a much more stable surgical field (Fig. 2).

Surgeon's position and port installation. Color images are available online.
First purse string
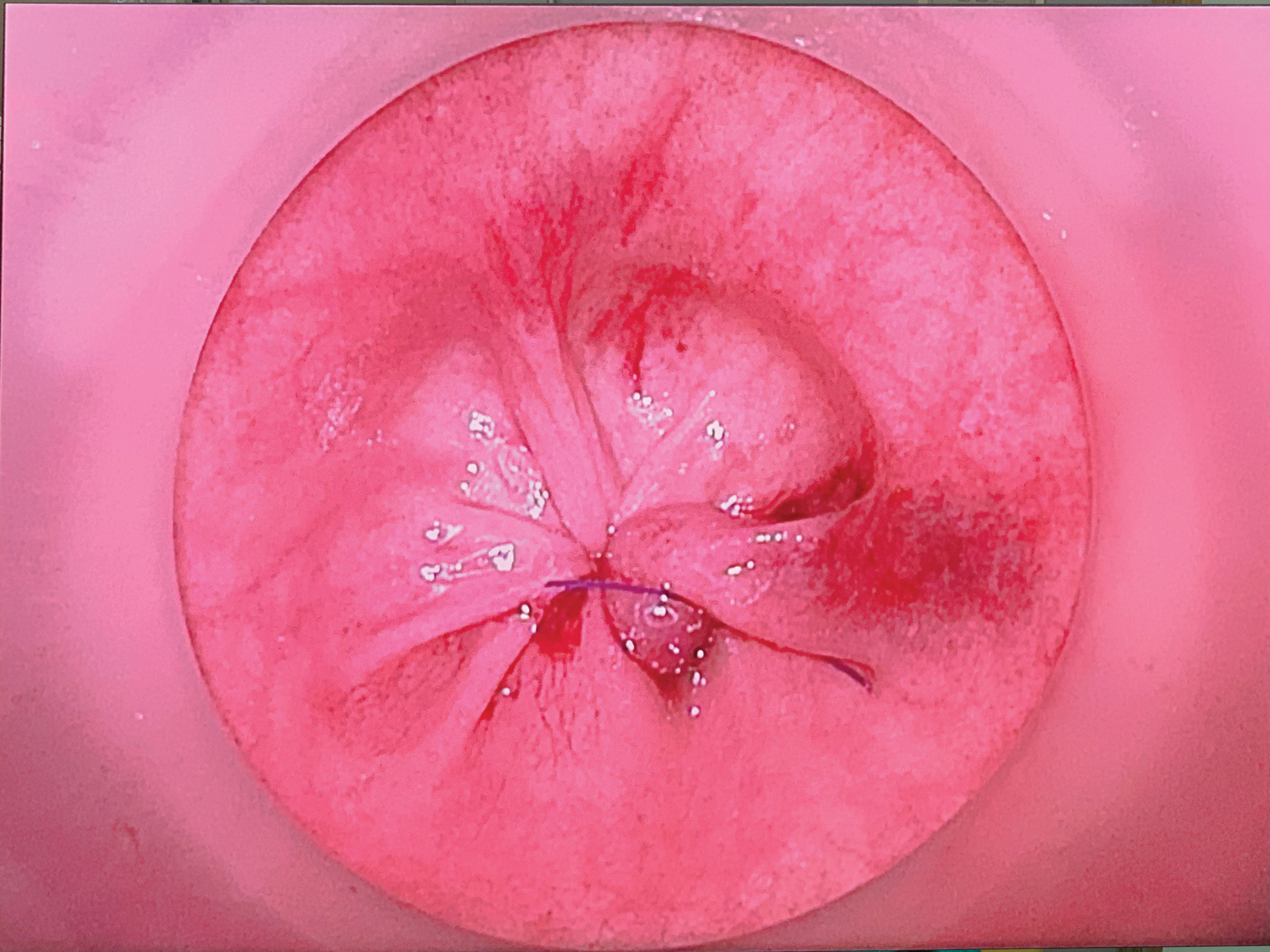
The first purse string, to close the rectum, was performed endoscopically with a Prolene 0 wire circumferentially, starting at the 5 o'clock position and finishing with an overlap of the stitches (Fig. 3). The knot was performed by hand, removing the cap of the transanal port.

First purse string. Color images are available online.
Rectotomy
Once the transanal port was reinstalled, the quality of the purse string was evaluated (Fig. 4). Rectal transection was performed with a monopolar laparoscopic hook. Rectotomy was started at the 5 o'clock position, layer by layer until the perirectal soft tissue was reached (Fig. 5). Then, the rectotomy was completed circumferentially with small steps, layer by layer.
First purse string closed. Color images are available online.
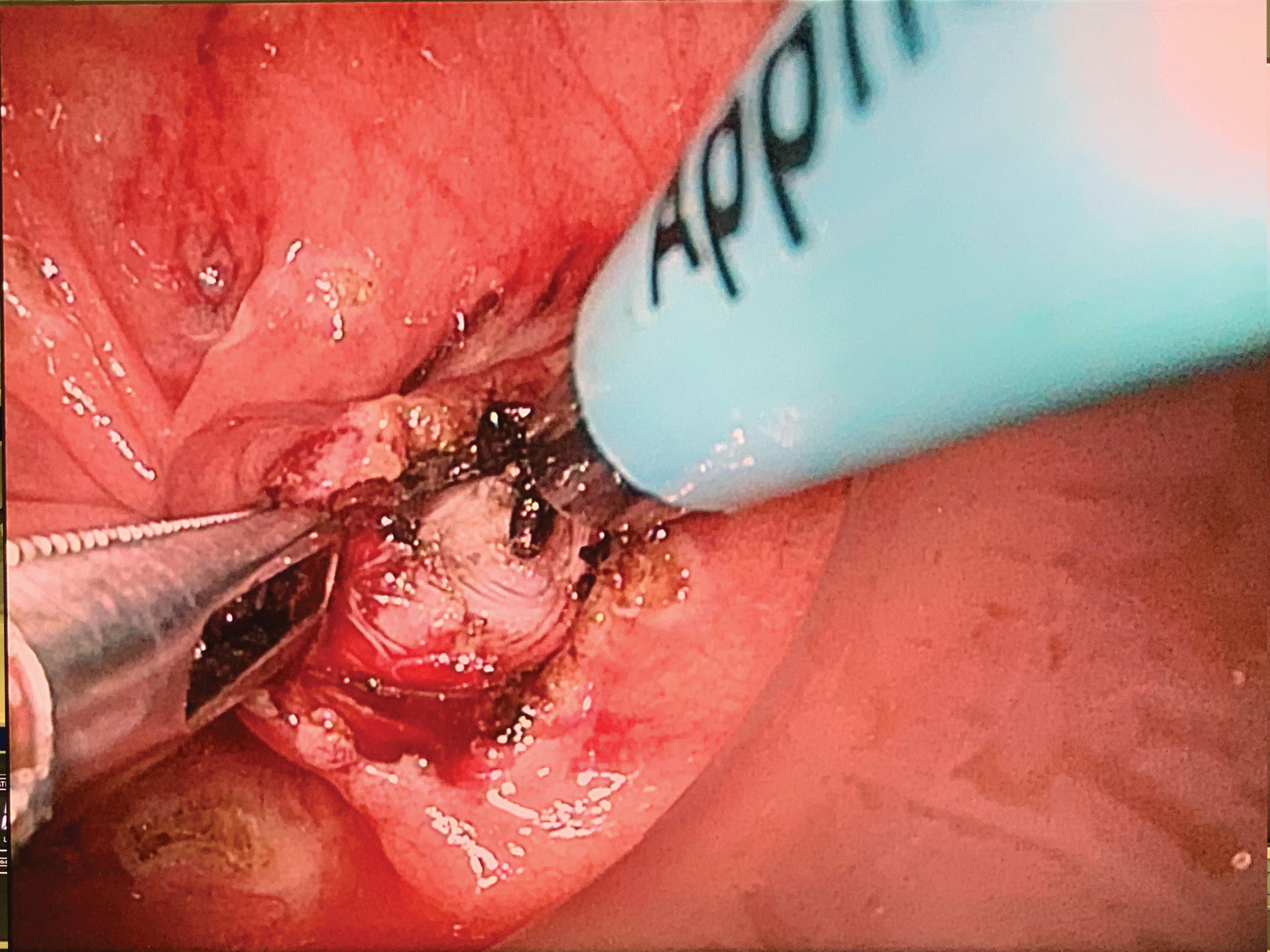
The beginning of the rectotomy. Color images are available online.
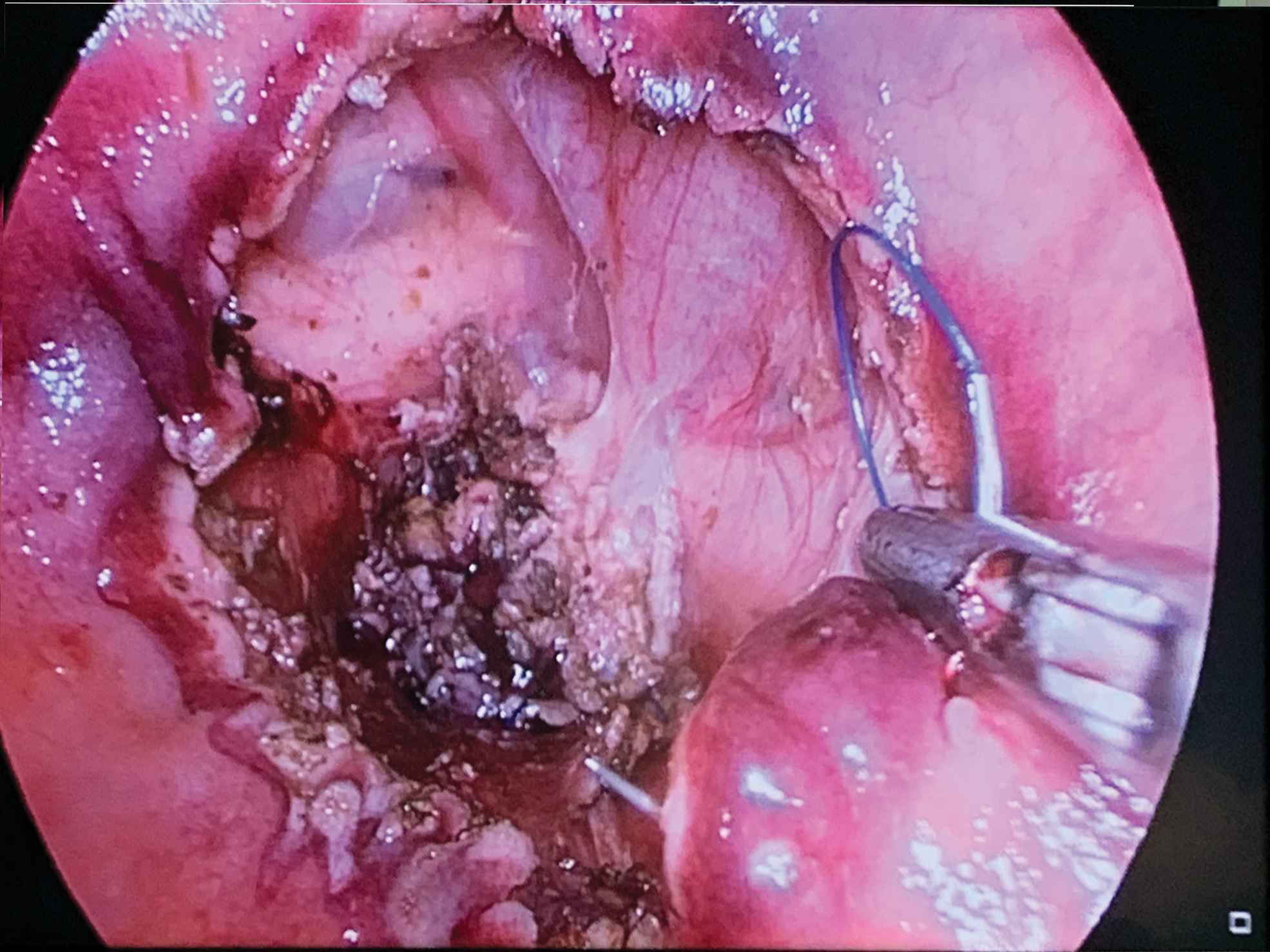
Dissection
The dissection phase was performed in a bottom-up manner through the soft tissue surrounding the rectum. Danish Landrace pigs have no real mesorectum but a thin layer of soft tissue composed of a mix of fat and connective tissue. In this phase, dissection was conducted following the lateral walls of the pelvic floor, leaving the soft tissue around the rectum (Fig. 6).

The end of the rectotomy and the beginning of the mesorectal dissection. Color images are available online.
Second purse string
The second purse sting, to close the rectal stump before the anastomosis, was performed endoscopically with a Prolene 0 wire, circumferentially, starting at the 5 o'clock position (Fig. 7). Every stitch had to include all the layers of the rectal wall because this purse string was to be used for anastomosis construction.
Second purse string. Color images are available online.
All the stitches needed to be passed from the mucosal side of the wall to the muscular side of the wall, except the last one, which had to be passed from the muscular side to the mucosal side. This method leaves both sides of the suture on the same side, and the knot can lay on the mucosa. (Fig. 8).

The final check before the anastomosis. Color images are available online.
Anastomosis
A small abdominal incision was performed, and the rectum was resected. The anvil of a 28 EEA stapler (Ethicon) was inserted into the proximal segment of the colon and secured using the purse-string suture, which was previously constructed. The proximal colon with the anvil was repositioned in the pelvis. The anvil on the proximal colon was pulled into the distal rectal ring, and the distal purse-string suture was tied around it. The stapler was introduced through the rectal stump, connected to the anvil, closed and fired. Once the anastomosis was fashioned, it was inspected transanally by the trainees.
Discussion
TaTME is the most recent evolution of transanal oncological surgery, 7 and it was developed in 2010 to overcome some of the challenges associated with minimally invasive TME.8,9 Since then, it has been suggested to be an efficient and safe technique for the treatment of rectal cancer. 10 However, as with any new surgical technique, new complications and new issues related to this technique have been described in the literature.11–13
The incidence of postoperative complications is demonstrated to be related to the experience of surgeons, and TaTME requires a learning curve of 40/50 cases. 14 In this scenario, the training of the surgeon seems to be fundamental for the safe use of this new surgical technique with a new view on anatomical landmarks. 15 For this reason, even consensus on structured training programs has been developed. 16
In 2018, the St. Gallen Consensus conference on TaTME recognized the cadaveric model as the main model for the practical training of surgeons approaching TaTME. 4 The aim of this preliminary experience was to analyze the efficiency of the animal model to train surgeons in TaTME.
The choice of Danish Landrace pigs was made for their pelvic anatomy, and their wide use in surgical training laboratories is related to the wide availability of these animal and the similarity of their tissues to live human tissues.
The main advantage noted during this early experience was the similarity of the rectum in terms of the texture and elasticity between these pigs and humans. This similarity makes purse-string suture construction and rectotomy very similar to the experience in human patients. Considering the importance of the first purse-string suture in the surgical management of the procedure and on the surgical outcomes, training with tissue similar to human tissue can increase the efficiency of training.
In the human cadaveric model, unfortunately, the preservation of a corpse by freezing or by the Thiel embalming technique 17 can negatively influence the structure of the tissue, which can be more fragile and less elastic than live human tissue.
Live animal tissue needs to be treated with care because, as in humans, mistakes in the surgical technique can cause bleeding. This adverse event is extremely useful for teaching a trainee how to gently move instruments in such a small surgical field and how to address the bleeding event. Bleeding events are not reproducible in the cadaver laboratory.
Considering rectotomy, the pig rectum is thinner than the human rectum; for this reason, the importance of being very gentle and proceeding layer by layer to avoid full rectotomy with limited use of the monopolar scalpel should be explained to trainees to decrease the didactical power of the experiment.
This anatomical characteristic, at first glance, can be considered a negative aspect of the animal model; in contrast, if explained well to trainees, careful layer-by-layer dissection in a small field can improve the quality of training.
The main anatomical difference between Landrace pigs and humans is the exiguity of the mesorectal tissue. The pig has very few fibers of connective tissue between the rectum in the pelvic walls. For this reason, the animal model cannot be considered a complete alternative to the cadaver laboratory.
During these preliminary experiments, the trainees were invited to continue dissection of the rectum from the pelvic wall to practice the dissection movements in the transanal field, even if the pig anatomy was slightly different from the human anatomy.
The construction of the second purse-string suture and the anastomosis can be efficiently trained in the animal model for the aforementioned reasons, with good similarity to the technique used in humans. The anastomotic time in Landrace pig appears to be shorter than that in cadavers due to the large pelvis of the animal and the wideness of the abdominal cavity. This characteristic can help trainees with less experience in low colorectal reconstruction.
The results of these preliminary experiments, supervised by surgeons with great expertise in TaTME and cadaver laboratories, suggest the animal laboratory as an opportunity to improve training for TaTME.
In all the editions of the animal laboratory, all the procedures were completed with no major damage to the anatomical structure or intraoperative death of the animal. All the participants could complete the procedure with only oral suggestions of the supervisors, and all of them confirmed complete satisfaction from the training received.
Animal training is easier to organize due to the rarity of institutions with cadaver laboratories in Europe and provides a cost-saving method. In Italy, the cost of the wet laboratory is ∼800 € for each animal, whereas the cost of the cadaver laboratory is ∼1500 € for every frozen cadaver.
Conclusion
Surgical training with animal models seems to be effective and useful for surgeons approaching the first steps of training in TaTME. Owing to its anatomical limitations, the animal laboratory is not a complete alternative to the cadaver laboratory but can be an opportunity to improve training alongside cadaver laboratories.
Animal laboratories can be considered a complementary activity to cadaver laboratories and proctoring to increase the effectiveness of training in TaTME.
Ethical Approval
This study follows the ethical standards and was approved by the institutional ethics committee and conducted according to the declaration of Helsinki.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.