
Abstract
Background:
In patients with recurrent inguinal hernia (IH) after totally extraperitoneal (TEP) hernioplasty, re-TEP hernioplasty is difficult because of fibrotic adhesions. Re-laparoscopic hernioplasty is possible by changing the approach from extraperitoneal to transabdominal. If iliopubic tract repair (IPTR), mainly used in the past for the open approach, is added as a laparoscopic procedure, re-laparoscopic hernioplasty is possible when treating recurrent IH. We aimed to evaluate the safety and feasibility of alternate transabdominal preperitoneal (TAPP) hernioplasty supplemented by IPTR for treating recurrent IH after TEP hernioplasty.
Methods:
We retrospectively evaluated 2600 patients with IHs who underwent TAPP hernioplasty from January 2015 to December 2020. Among patients with recurrent IH, those who underwent primary TEP were included in the study. For reoperation, TAPP hernioplasty was performed and IPTR was added. IPTR was performed by suture closure of the internal inguinal ring by the iliopubic tract and medial aponeurotic arch of the transversus abdominis muscle.
Results:
Of the 35 patients (33 males and 2 females) with recurrent IH after primary TEP hernioplasty, 51% (18/35) of patients had recurrence within 2 years of the first operation. There were 28 recurrent IHs of the same type as the original, and 7 cases of a different type. The mean TAPP operation time was 41 minutes. Chronic inguinodynia and re-recurrence was not observed. One patient had inferior epigastric vessel injury, which was successfully repaired.
Conclusion:
Adding laparoscopic IPTR to TAPP hernioplasty is safe feasible treatment for recurrent IH after TEP hernioplasty.
Introduction
Inguinal hernia (IH) is a condition commonly encountered in the field of general surgery. Laparoscopic repair is currently widely used for IH treatment, and the representative surgical methods are transabdominal preperitoneal (TAPP) hernioplasty and totally extraperitoneal (TEP) hernioplasty. 1 Although TAPP and TEP have different approaches, the method of mesh implantation after wide dissection of the preperitoneal space is the same. The recurrence rate after laparoscopic IH repair is reported to be low regardless of whether TAPP or TEP is used.2,3
The current guidelines recommend a laparoscopic operation and large-size mesh for the treatment of recurrent IHs originally repaired with a primary open approach and an open approach for the treatment of recurrent IHs originally repaired with a primary laparoscopic operation.1,4 Successful treatment of recurrent hernias using laparoscopic procedures for subsequent hernia repairs after a primary laparoscopic operation has also been reported. 5 If herniation recurs after TEP hernioplasty, it is difficult to access the preperitoneal space with the same method as the previous extraperitoneal approach because of fibrotic adhesions. Therefore, in the treatment of recurrent IH after TEP hernioplasty, it is necessary to have a surgical method that utilizes a different approach.
There are two different approaches: open repair and TAPP hernioplasty. In previously published reports, open surgery was mainly performed for recurrent IH after TEP hernioplasty. 4 Compared with open repair, TAPP hernioplasty has the advantages of reduced acute pain, faster time to recovery, smaller incision, and more accurate anatomical assessment. 1
We assume that TAPP hernioplasty may be a favored treatment in patients with recurrent IH after TEP hernioplasty. Because TAPP hernioplasty is a transabdominal approach, there is no concern about existing fibrotic adhesions. The TAPP hernioplasty requires a wide preperitoneal dissection. However, dissection of the existing mesh is difficult because of fibrotic adhesions. We considered a method with dissection of only the preperitoneal space centered on the site of recurrence without dissection of the preperitoneal space covered by the pre-existing mesh.
However, new mesh implantation is difficult because of insufficient preperitoneal space. Therefore, we added iliopubic tract repair (IPTR) to TAPP, preserved the existing mesh, and performed an operation to cover the whole myopectineal orifice using new mesh along with the previous mesh. IPTR was performed by suture closure of the internal inguinal ring by the iliopubic tract and medial aponeurotic arch of the transversus abdominis muscle. Adding laparoscopic IPTR to TAPP hernioplasty may not be ideal for low-volume centers and less-experienced surgeons; IPTR is mainly performed in open preperitoneal hernioplasty. Although IPTR may be difficult to perform in laparoscopic hernioplasty because of the challenge of intra-abdominal suturing, we assume that this technique can be useful for complicated hernias such as recurrent IHs after TEP hernioplasty.
Nyhus reported the efficacy of IPTR for treating primary and recurrent IH by open surgery.6,7 The iliopubic tract was first described by Thomson 8 and is identified as a thickening of the transversalis fascia running deep and parallel to the inguinal ligament. 9 The iliopubic tract lies on the posterior aspect of the inguinal region and plays an important role during hernia repair. IPTR was added as a way to reduce the risk of re-recurrence. Adding IPTR eliminates the need for a wide preperitoneal dissection, preserves the previous mesh, and adds a new mesh to cover the full myopectineal orifice. In addition, IPTR can prevent mesh migration.
The purpose of this study was to evaluate the safety and feasibility of adding IPTR to TAPP hernioplasty that overlays a new mesh without removal of the previously implanted mesh in the treatment of recurrent IH after TEP hernioplasty.
Materials and Methods
Patients and data collection
We retrospectively evaluated 2600 patients with IHs who underwent TAPP hernioplasty from January 2015 to December 2020 (Fig. 1). Among patients with recurrent IH, those who underwent primary TEP were included in the study. Because TAPP hernioplasty was performed in both primary IH and recurrent IH at our institution, all patients with recurrent IH after TEP hernioplasty were admitted for reoperation after primary surgery at an external hospital. We collected and analyzed data from the period from first operation to recurrence, gender, age, type of IH at first operation, type of recurrent IH, operation time, complications, postoperative pain, chronic inguinodynia, and re-recurrence. If there was pain even 3 months after surgery, it was defined as chronic inguinodynia. This study was approved by the Institutional Review Board of Damsoyu Hospital.
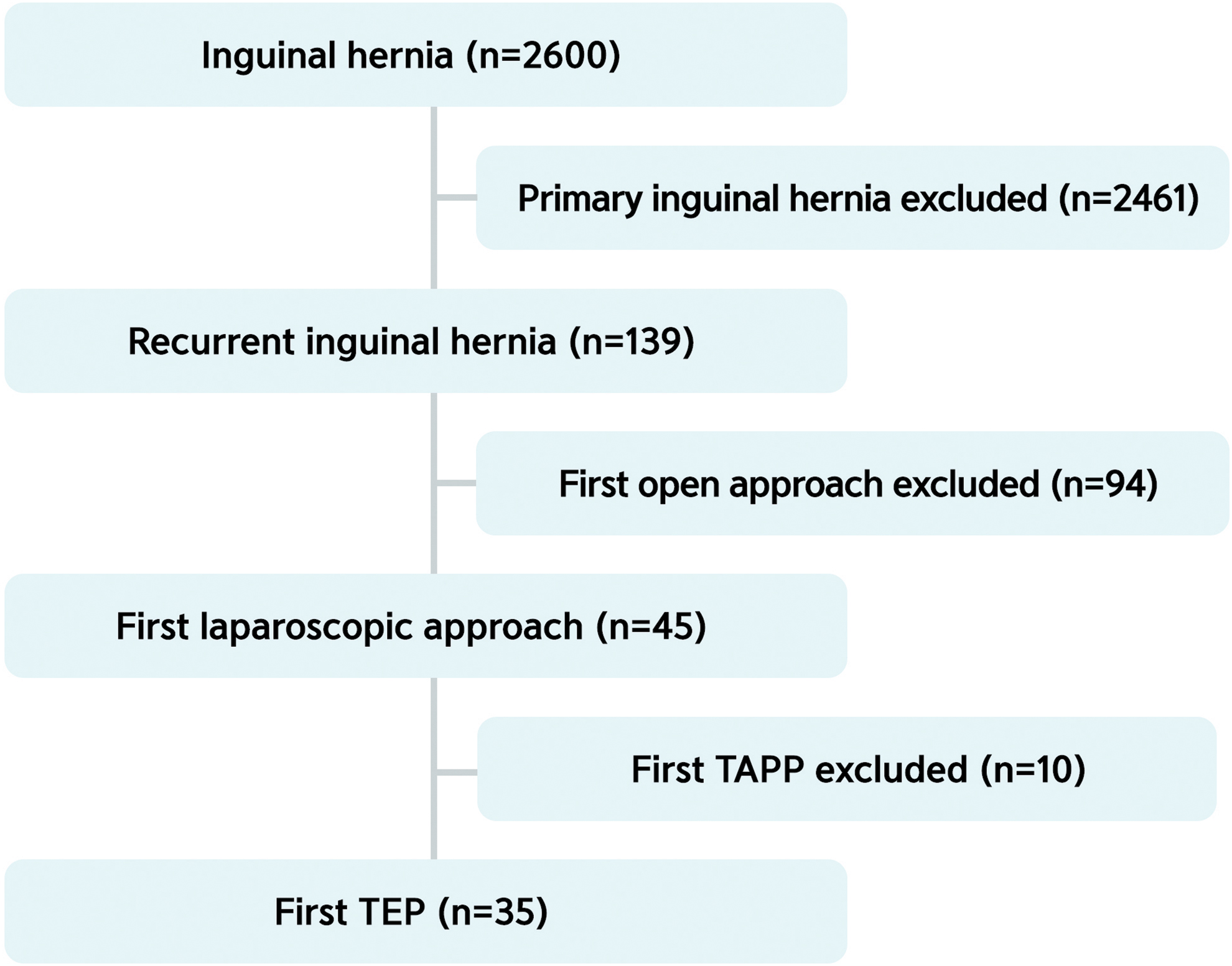
Flowchart of patient inclusion and exclusion. Color images are available online.
Surgical technique
All 35 patients underwent laparoscopic TAPP hernioplasty, including IPTR with a three-port laparoscopic system. The procedures were performed with the patients under general anesthesia and in the supine position. The laparoscopic system used a 5.0-mm camera and 5.0-mm instruments. A 5.0-mm transumbilical incision was used to create pneumoperitoneum using a 5.0-mm trocar, and carbon dioxide pressure was maintained at 8–10 mmHg. Two other 5.0-mm instruments were inserted through separate 5.0-mm stab incisions in the lateral abdomen.
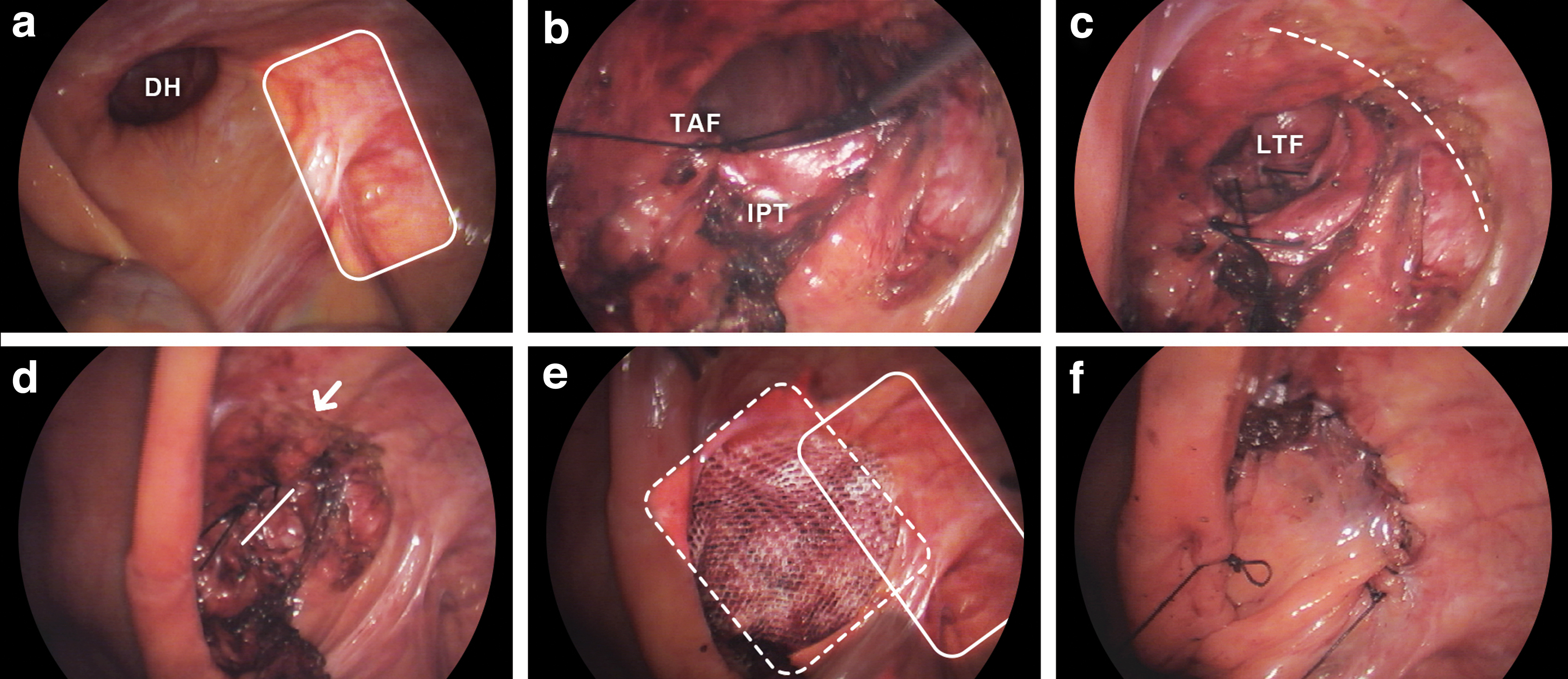
After creating the pneumoperitoneum, we identified the hernia type and previous mesh position (Fig. 2). In the case of indirect IHs (Fig. 3), the deep inguinal ring was closed with IPTR using a nonabsorbable multifilament suture (silk 1–0). The laparoscopic iliopubic tract suture technique was performed with continuous suture as previously reported. 10 The IPTR was performed using continuous running suture in all patients. The iliopubic tract and medial muscular arch of the transversus abdominis muscle were tied. The first stitch was performed with sufficient space for the vas deferens, the spermatic cord vessels, and round ligament to pass through without compression. Next, continuous sutures for IPTR were performed from the medial to the lateral direction.

Types of recurrence.

TAPP with IPTR on recurrent indirect hernia.
The peritoneum was then closed from the lateral to the medial direction using continuous sutures. The genitofemoral nerve divides into a femoral branch and a genital branch. The genital branch of the genitofemoral nerve travels alongside the spermatic cord vessel or round ligament in the inguinal canal. Suture did not cause injury to the genital branch of the genitofemoral nerve because the iliopubic tract that was sutured is located 1 cm from the spermatic cord vessel or round ligament. The femoral branch of the genitofemoral nerve was protected because it passes under the iliopubic tract in the laparoscopic view. 11
In the direct IHs (Fig. 4), we sutured the lax transversalis fascia together during the defect repair to decrease the risk of seroma development. When the defect was closed, the next step was to perform peritoneal dissection to make space for the new mesh. The new polypropylene mesh size was 10 × 8 cm2. A space was secured so that the mesh could fit around the defect. In this process, the mesh placed during the previous surgery was not removed because of the risk of damage to adjacent tissue. The peritoneum was continuously sutured with absorbable multifilament suture (2–0 Vicryl; Ethicon, Inc., Somerville, NJ).
TAPP with IPTR on recurrent direct hernia.
Protocols and follow-up
The patients were permitted to ingest liquid 2 hours after the operation. The protocol at our institution stipulates that patients can be discharged if their condition remains stable, and if they are comfortable while performing daily activities (such as walking and eating). Post-herniorrhaphy pain was evaluated using a 0- to 10-point numeric rating scale (NRS). Routine outpatient follow-up included a physical examination at 1 week and 1 month after surgery. An annual telephone follow-up interview was performed. The follow-up period ranged from 12 to 81 months. Telephone interviews were performed to obtain information on the patients' postoperative status, such as pain and complications.
Results
Patient characteristics and surgical outcomes are shown in Table 1. In all, 35 patients (33 males and 2 females) with recurrent IH after primary TEP hernioplasty were included in the study. Of those, 51% (18/35) of patients had recurrence within 2 years of the first operation. There were 28 recurrent IHs of the same type as in the first operation, and 7 cases of a different type of IH.
Characteristics and Surgical Outcomes of Patients
Categorical variables are represented as n (%) and continuous variables as mean ± standard deviation (range).
NRS, numeric rating scale.
The mean operation time was 41 minutes. One patient had inferior epigastric vessel injury, which was successfully repaired. The mean period until return to normal activities was 6.4 days. The mean NRS pain score was 0.8 (range 0–2) at 1 month after the operation. Chronic inguinodynia and re-recurrence were not observed.
Discussion
The recurrence rate after TEP hernioplasty has been reported as 2.1% to 3.5%.12,13 The recurrence is major complication of hernia repair. 14 Recurrence remains a major challenge to the surgeon and can result from various causes. There are three main causes of recurrence: technical factors (such as inadequate mesh size or inadequate mesh fixation), surgeon-related factors (such as experience), and patient-related factors (such as weak tissue, poor wound healing, and wound infection).15–17
According to the International Endohernia Society (IEHS) guidelines, the anterior approach usually seems to be the best choice after recurrent IH following TEP hernioplasty because of fibrotic adhesions of the preperitoneal space. 1 IEHS guidelines also state that TAPP is possible by an expert surgeon for treatment of recurrent IH that occurs after TEP hernioplasty grade C. 1 Re-recurrence of recurrent IH is reported to have a higher risk than recurrence of primary IH.6,7
TAPP hernioplasty is capable of accurately determining the type of hernia, the location of the previously implanted mesh, and a contralateral IH. 5 In addition, it is possible to check the anatomical changes of previous surgery, which is advantageous for surgical planning. In this study, we were able to confirm the location of the recurrent defect and the pre-existing mesh in all patients. The peritoneal incision was started around the recurrent defect, avoiding the pre-existing mesh, and preperitoneal dissection was performed. During this process, the pre-existing mesh was not removed according to the level IV recommendation of the IEHS guidelines. 1 Defect closure was achieved through IPTR, and new mesh was implanted. Pre-existing mesh and new mesh cover more than 20 × 15 cm2 in the form of pants-over-vest suturing technique.
There are three main reasons why we added IPTR to TAPP hernioplasty in patients with recurrent IH after TEP. First, IPTR supplements the preperitoneal space required for new mesh implantation. When performing TAPP, it is necessary to dissect the previous mesh, but dissection is difficult because of fibrotic scarring. Second, IPTR prevents mesh migration toward recurrent defects. Third, IPTR is a surgical method that has already been verified in an open approach. This proven surgical method is an effective adjunct to laparoscopic repair.
The Nyhus groin hernia classification system is used worldwide. 18 Nyhus classified recurrent IHs as type IV. IPTR with mesh implantation has been proposed for treating recurrent type IV IH.6,19 There may be concern about pain resulting from IPTR tissue repair; according to many reports, the major reason for performing tension-free surgery was pain. The IPTR suture line is ∼2 cm, and there is almost no tension when suturing. In this study, no chronic pain was identified.
This study has some limitations. Because the focus was on TAPP hernioplasty, there was no control group such as open repair or re-TEP hernioplasty. Only laparoscopic operations were performed, and thus no comparison could be made with open surgery. Although the number of patients (n = 35) included in this study may seem small compared with that included in studies of other conditions, this report showed that the prevalence of recurrence after TEP hernioplasty is low, and there are few reports on IPTR. This was a single-center study, and a multicenter study is needed in the future.
Conclusion
Adding laparoscopic IPTR to TAPP hernioplasty is a safe and feasible operation for the treatment of recurrent IHs after TEP hernioplasty.
Footnotes
Authors' Contributions
The first/corresponding author contributed to the study conception and design. Methodology, material preparation, data collection, writing—original draft preparation, formal analysis, investigations, project administration, and resources were provided and performed by S.R.L. The first/corresponding author read and approved the final article.
Acknowledgments
The author thanks Hyejin Park for performing the primary English grammar correction of this article, and Beom Seok Oh and Young Hyun Lee from the research center of Damsoyu Hospital for assisting with the statistical analysis and organizing the data in this article. The author also thanks Andrea Baird, MD, from Edanz (![]() ) for editing a draft of this article.
) for editing a draft of this article.
Ethic Approval
The study was approved by the International Review Board of Damsoyu Hospital (DSY-2021-008).
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.