
Abstract
Background:
Thoracoscopic lobectomy is a challenging procedure in children with congenital lung malformations (CLMs). This study aims to evaluate the safety and efficacy of thoracoscopic clockwise lobectomy (TCL) in CLMs in children and its potential to be a stylized procedure.
Methods:
All patients with CLMs who received TCL from 2015 to 2019 in our hospital were retrospectively reviewed. Clinical information was extracted from medical records, including patient demographics, operative details, and outcomes.
Results:
A total of 184 patients with a median age of 6.8 months (range, 3–156) and a median weight of 9 kg (range, 6–45) received TCL. Lesions were all located in the lower lobe and included congenital pulmonary airway malformation (n = 133), intralobar sequestration (n = 44), bronchiectasis (n = 4), and congenital lobar emphysema (n = 3). The mean (±standard deviation [SD]) operating time was 46 ± 7.5 minutes (range, 35–113). The mean (±SD) blood loss was 3.5 ± 0.8 mL (range, 1–60). Three patients converted to thoracotomy, and 162 patients did not have a chest tube placed. The postoperative course was uneventful in all patients except 2 patients who developed air leaks and 23 patients who developed a mild fever. The median length of postoperative hospital stay was 2 days. A total of 163 patients were followed up for more than 1 year without any complications.
Conclusion:
TCL is suitable for lower lobectomy and is safe and effective in standard and complicated thoracoscopic lobectomy. It could be recommended as a stylized procedure in treating children with CLMs.
Introduction
Congenital lung malformations (CLMs) are a heterogeneous group of diseases with an increasing incidence among neonates due to progress in prenatal imaging. The most common location of CLMs is the lower lobe.1,2 Considering the relatively high risk of long-term complications of infection and malignant transformation, many pediatric centers propose early surgical resection even in asymptomatic patients. 3 Thoracoscopic lobectomy has gained wide acceptance in adult surgery for its advantages over thoracotomy in terms of hospital stays and postoperative complications. 4 However, there are still many limitations in treating children with CLMs by thoracoscopic lobectomy, such as a broad spectrum of lung diseases requiring different techniques, specific physiological characteristics in children, including narrow thoracic space, and anatomical variations in bronchovascular structures.5,6 Thoracoscopic lobectomy remains a challenging procedure in children with CLMs.
Pediatric centers worldwide have gradually begun to perform thoracoscopic lobectomy for children with CLMs in recent years due to advances in endoscopic surgical equipment and technology. 7 While there are increasing reports in thoracoscopic treatment among children, many operative methods described in other reports have a massive difference in operation steps. Therefore, these methods significantly differ in terms of blood loss, operative time, conversion rate, and postoperative complications.8–11 Furthermore, there is no stylized operative method containing programmed steps that surgeons and assistants can follow during surgery. The absence of a stylized operative method may result in a steep learning curve for beginners of thoracoscopic lobectomy, which is harmful to patients' health and widespread thoracoscopic lobectomy. Therefore, a relatively safe, simple, effective, and stylized thoracoscopic lobectomy for children is urgently needed.
Thus, we tried a “clockwise” procedure. We rotated around the lower lobe bronchus clockwise or counterclockwise to suit the physiological and disease characteristics of the children. This study aims to evaluate the efficacy and safety of thoracoscopic clockwise lobectomy (TCL) and finally to discuss its potential to be used as a stylized procedure.
Methods
Patients
All patients diagnosed with CLMs who underwent TCL at our institution from January 2015 to January 2019 were included in this study. Exclusion criteria included age over 16 years, bilateral lesions, missing data for perioperative information, resection of two or more lobes, patients treated with coexisting diseases during surgery, and patients who underwent the combination of wedge resections or segmentectomy with lobectomy. All patients were evaluated preoperatively by contrast-enhanced chest computed tomography (CT), and pathology reports confirmed the diagnosis of CLMs. Clinical information, including patient demographics, operative time, estimated blood loss, conversion to thoracotomy, chest tube insertion, postoperative complications, and postoperative hospital stay, was extracted from medical records. Evaluation of the patients concerning their health and growth status was obtained in the following ways: the latest outpatient follow-up structured 10-minute telephone calls or the internet follow-up for parents who could not go to the outpatient clinic.
The study was approved by the Institutional Review Board of West China Hospital, and written informed consent was obtained from legal guardians.
Operative method
We used single-lumen, double-lumen, and bronchial blockers for one-lung ventilation based on the patient's situation. At the same time, we used a proper flow (about 5 mmHg) of carbon dioxide to fill the chest cavity to acquire a better operative field. After adequate anesthesia, the patient was placed in a lateral decubitus position. Two 5 mm working ports are placed at the fifth intercostal of the anterior axillary line and the ninth intercostal space of the posterior axillary line, and a 5 mm thoracoscope port is placed at the eighth intercostal space of the mid-axillary line. We chose the pulmonary hilum approach, which has been reported in our previous study. 12 The operative method is shown in Figure 1. The first step is dissecting the inferior pulmonary ligament using an electrocoagulation hook to expose the inferior pulmonary vein (the anomalous artery from the systemic circulation within the inferior pulmonary ligament is usually clamped at first in patients with intralobar sequestration). The second step is taking the lower lobe bronchus as the center and gradually dissecting the interlobular fissure in a clockwise direction in the left lobe and a counterclockwise direction in the right lower lobe. The third step is to ligate and divide the lower lobe pulmonary artery and then dissect the fissure along the previous direction to expose the adjacent lower lobe bronchial wall. After a circle of dissection and return to the inferior pulmonary vein, the inferior pulmonary vein is ligated and divided. Finally, the lower lobe bronchus is wholly exposed and ligated to complete the procedure. We used absorbable clip and hem-o-lok for vascular and bronchial ligation, separately. The overall direction of the procedure is shown in Figure 2.
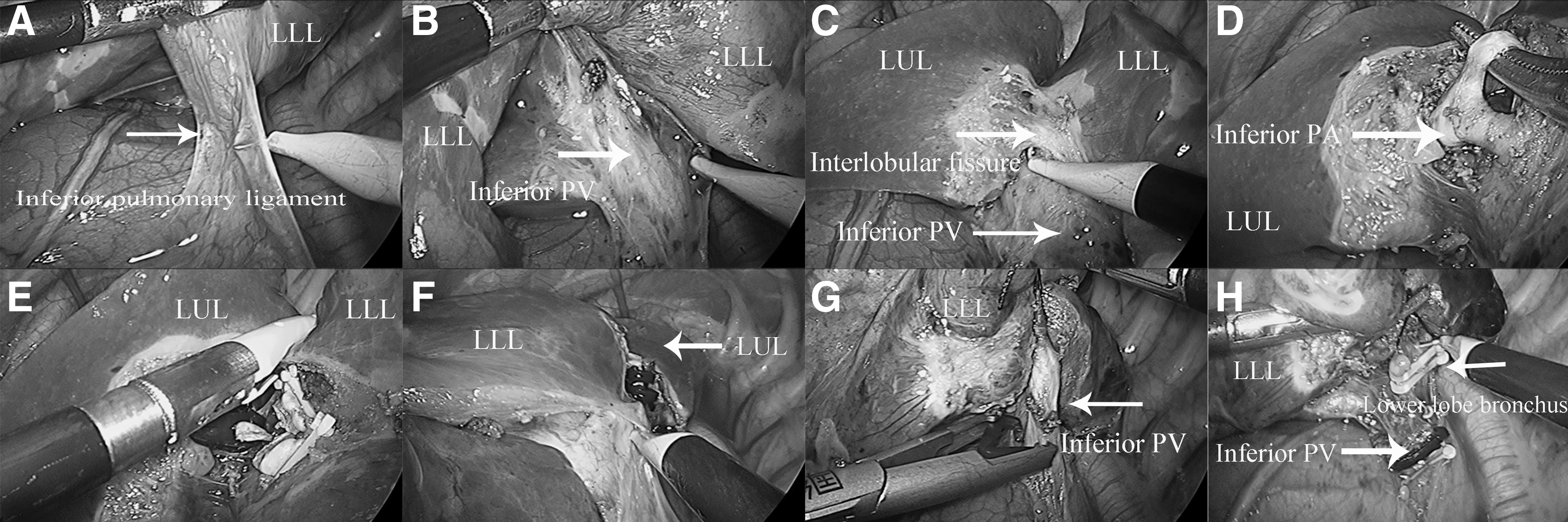
The operative procedure in the left side of lung. After dissecting the inferior pulmonary ligament
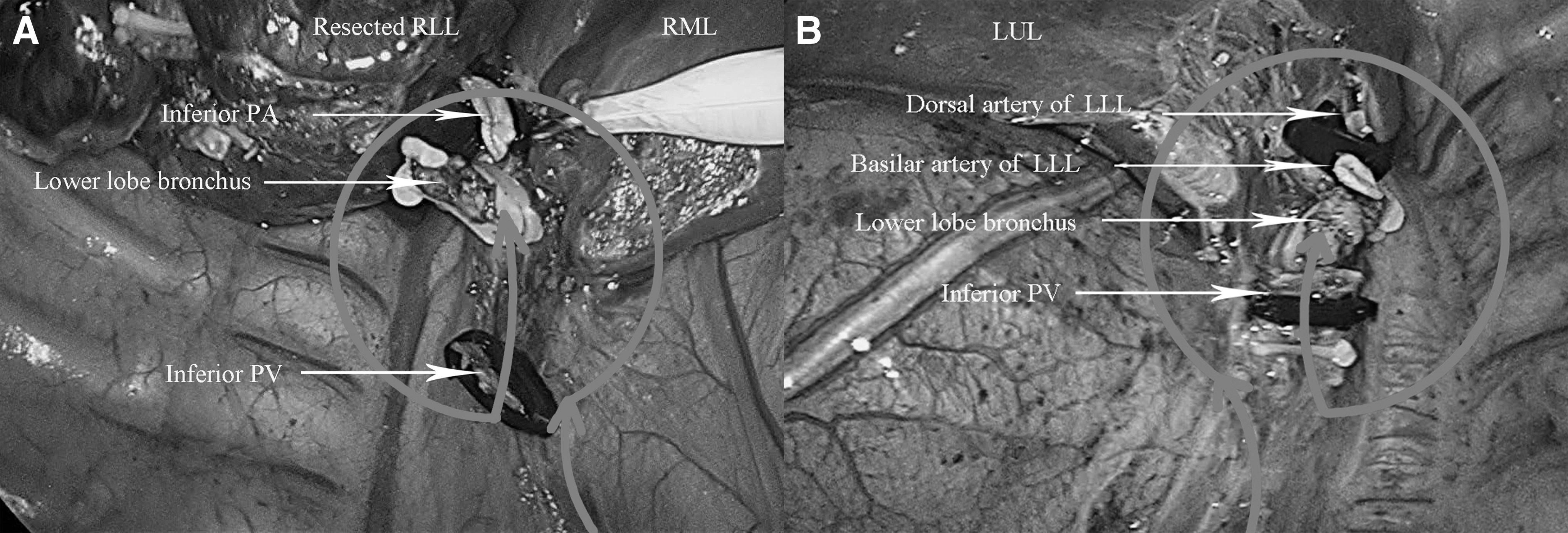
Direction of the operation on different sides of lung. Arrow in gray marks the overall direction of the operation which is counterclockwise in right lower lobe
At the end of the procedure, we routinely flush the pulmonary hilum with warm saline and inflate the lungs to watch for air bubbles due to leaks. Chest drains are not usually placed when no air bubbles or obvious bleeding is seen.
Statistical analysis
SPSS (version 26) was used for statistical analysis. The normal distribution of the continuous variable was expressed as the mean ± standard deviation (SD). The abnormal distribution of continuous variables was expressed as the median and range, and count data were expressed as the rate (%).
Results
From January 2015 to January 2019, 184 patients with CLMs underwent TCL by one surgeon. One-lung ventilation was performed in 160 patients, while double-lung ventilation was performed in the rest. There were 113 males and 71 females, with a median age of 6.8 months (range, 3–156) and a median weight of 9 kg (range, 6–45). All patients underwent lower lobectomy, in which 81 cases were on the left side and 103 cases were on the right side. As shown in Table 1, the pathological diagnosis was congenital pulmonary airway malformation in 133 patients, intralobar sequestration in 44 patients, bronchiectasis in 4 patients, and congenital lobar emphysema in 3 patients. All patients underwent TCL successfully, except 3 patients who were converted to open thoracotomy because of extensive pleural adhesions. There were no intraoperative complications or blood transfusions. The mean (±SD) operative time was 46 ± 7.5 minutes (range, 35–113 minutes), and the mean (±SD) operative blood loss was 3.5 ± 0.8 mL (range, 1–60 mL). Except for 3 patients who underwent thoracotomy and 19 patients who underwent thoracoscopic lobectomy, a chest tube was placed, which was removed within 1–10 days postoperatively. The other 162 patients (88%) did not have chest tubes placed. Postoperatively, all children recovered a regular diet after 6 hours. Twenty-three patients developed mild fever, but all recovered normal body temperature after physical cooling within 1–3 days. Only 2 patients developed small air leakage, which was automatically closed within 5–7 days, without serious complications such as atelectasis, hemorrhage, or bronchopleural fistula (see Table 2).
Clinical Characteristics of 184 Patients with Congenital Lung Malformations
CPAM, congenital pulmonary airway malformation; SD, standard deviation.
Clinical Outcomes of the Patients who Underwent Thoracoscopic Clockwise Lobectomy
SD, standard deviation.
A total of 21 children were lost to follow-up, and 163 patients (88.6%) were followed up for more than 1 year without any complications. All 163 patients had good residual lobe expansion and normal daily activities. There were no postoperative remnant cystic lesions, recurrence, or other complications on the CT scan.
Discussion
CLMs are the dominant lung diseases that require resection in children. Approximately 70% of CLM patients are treated with surgical resection worldwide, usually undergoing thoracoscopic lobectomy, considering the potential recurrent infection and malignant transformation. 13 In this study, we evaluated the safety and efficacy of TCL among children with CLMs. Our data showed good results in terms of operative time, intraoperative bleeding, conversion rate, and postoperative complications.
As our data have shown, the indication for TCL is that the lesions are all located in the lower lobe, which is determined by the spectrum of lung diseases and the anatomical and physiological characteristics of children. The inferior pulmonary ligament is generally used as the starting point and is dissected at first in a thoracoscopic lower lobectomy. There are two options after dissecting the inferior pulmonary ligament: resection of the inferior pulmonary artery or inferior pulmonary vein. Because adult patients that commonly undergo lower lobectomy are dominant malignant diseases, the amount of blood retained in the resected lobe is small. 14 Adult patients are often treated with thoracoscopic single-direction lobectomy that ligates and divides the inferior pulmonary vein first. 15
However, it may increase the risk of anesthesia and surgical complications in children. First, the lung may become congested and edematous because the amount of retained blood in the resected lobe is relatively higher in children than in adults, making it difficult to manipulate with endoscopic instruments. 16 Second, most children have benign congenital malformations and do not need to ligate the pulmonary vein first to prevent potential hematogenous metastasis. Therefore, the pulmonary artery should be ligated first in children, followed by the pulmonary vein and lobe bronchus.
Because the lower lobe bronchus is located between the pulmonary artery and the pulmonary vein, the pulmonary vein and pulmonary bronchus should be bypassed to ligate the pulmonary artery first. We chose to rotate around the lower lobe bronchus to ligate the pulmonary artery, pulmonary vein, and lower lobe bronchus in an orderly manner, with the clockwise direction in the left lobe and counterclockwise direction in the right lobe to ensure that the pulmonary artery was ligated first. The resection is a single directional rotation and progresses in sequence; therefore, it does not require repeated turnover of the pulmonary lobes, which can minimize lung tissue damage and shorten the operative time.
In addition, programmed steps during surgery may reduce the magnitude of movements of instruments and adapt well to the narrow intercostal space and thoracic cavity of children, so the surgical complication rate is low. The interlobular fissure or the vein near the mediastinum is usually the starting point for upper and middle lobe resection. The purpose of ligating the artery and vein in sequence can be achieved by thoracoscopic single-direction lobectomy. Therefore, TCL does not seem to suit upper and middle lobectomy in children.
It has been reported that the conversion rate of thoracoscopic lobectomy ranges from 0% to 33%,17,18 and conversion usually occurs in the presence of severe pleural adhesions or vascular injuries. The conversion rate in our study was 1.6%, which is relatively low compared to other series, further proving the safety and effectiveness of this procedure. The presence of severe adhesions due to recurrent infection can cause a limited visual and operative field, significantly increasing the difficulty of the surgery. 19 All 3 patients who underwent conversion to thoracotomy in our study had severe adhesions, consistent with former studies. Because the bronchovascular structures at the pulmonary hilar are separated strictly following the anatomical gap in the procedure, the intraoperative blood loss is slight, with an average of 3.5 mL.
Moreover, most patients do not even need to have chest tubes placed. 20 Regarding surgical complications, postoperative air leakage or bronchopleural fistula is relatively common in thoracoscopic lobectomy, even up to 25%.21–24 In our study, only 2 (1%) patients with incomplete interlobar fissures developed air leaks, which self-healed after prolonging the chest tube placement time or repositioning the chest tube. Twenty-three patients developed a postoperative fever. They all returned to normal body temperature after 2–3 days of physical cooling, which is assumed to be absorption fever related to surgical tissue trauma. Therefore, TCL is a safe and effective surgical procedure. All patients in our series recovered a regular diet after 6 hours postoperatively. Chest CT was performed 1 day after surgery to detect if pleural effusion or bronchial fistula developed. And there are no complications, such as atelectasis, in any patient. In addition, the postoperative hospital stay of most patients in our study was 2 days, which reflects the faster recovery under thoracoscopic surgery.
Patients in our series contain a variety of diseases, ages, and disease characteristics. The lesion size is an essential factor affecting the operation due to the limited operative space in children. The operation is difficult with extensive lesions, and it is more likely to convert to thoracotomy. 25 In our study, the TCL successfully removed the lesion with a maximum diameter of 7.3 cm. In addition, nearly one-third of patients had incomplete interlobar fissures, and 8.2% of patients had anatomical variants of the pulmonary artery in our series. It is dangerous to dissect the superficial interlobar fissure directly to reveal the pulmonary artery that may be completely buried in the lung tissue. 23 It may also accidentally injure the anatomical variants and result in severe consequences.
Consequently, we chose to consecutively open the pleura from the inferior pulmonary vein to the intrafissural parenchyma in a clockwise or counterclockwise direction, and a tunnel was created by dissecting the parenchyma and the pulmonary artery sheath, which can dissect the intrafissural parenchyma in a clear view and prevent errors caused by anatomical variations. Therefore, TCL has wide adaptability and may become a stylized surgical procedure.
The operative time of thoracoscopic lobectomy in children is usually long and varies in different reports. Boubnova reported a mean operative time of 176 minutes for thoracoscopic lobectomy, 9 and another study also reported an operative time often of ∼2.5 hours, ranging from 1.5 to 4 hours depending on the difficulty of the procedure, with a difference of up to 2 hours between different hospitals. 26 The longest operative time in our series was 113 minutes, which is relatively short compared to other series. A possible reason is that TCL is a programmed procedure in which surgeons and assistants can follow programmed steps to resect hilar structures in a clockwise or counterclockwise direction, which may allow beginners to accumulate experience with thoracoscopic lobectomy in a short time and shorten the learning curve.
TCL is an effective and safe procedure, and it may become a stylized procedure for the treatment of CLMs in children. However, there are some limitations of this procedure: first, it is currently only applicable to lower lobectomy but not to upper and middle lobe resection in children; second, this study is a single-center retrospective study and lacks a control group, and the relevant evaluation criteria involved in the study are limited, so further studies are needed to confirm its safety and efficacy.
In conclusion, although it remained explored on the large scale of CLM patients, TCL proved its safety and effectiveness in this retrospective research with its shorter operative time and lower operative and postoperative complication rate. Moreover, with its certain anatomical markers and steps, it is easy to learn and deserves to be recommended as a stylized procedure to treat a certain subset of CLM patients.
Footnotes
Authors' Contributions
Study conception and design: D.L., X.F., K.C., and Y.L. Data acquisition: T.H., R.J., and C.L.; Analysis and data interpretation: G.Y. and Y.W.; Drafting of the article: D.L., X.F., and Q.W.; Critical revision: M.Y. and C.X.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (Grant No. 31201095).