
Abstract
Introduction:
Many studies focus on comparing outcomes of the open method for inguinal hernia repair (IHR) and the laparoscopic method. However, few studies compare different laparoscopic techniques. With over a dozen different techniques described in the literature for laparoscopic IHR, significant opportunities exist to study the efficacy of each technique. We investigated outcomes of a subcutaneous endoscopically assisted transfixion ligation (SEATL) technique and a percutaneous internal ring suturing (PIRS).
Materials and Methods:
After receiving institutional review board approval, we completed a retrospective chart review of IHR performed at our pediatric tertiary care center between September 2015 and May 2020. We included all patients under the age of 18 years. We separated laparoscopic repairs from total repairs. Laparoscopic repairs were further divided into their respective techniques. Factors involving patient demographics, operative details, and postoperative complications were statistically analyzed using SPSS.
Results:
There was a total of 131 IHRs performed with SEATL and 124 IHRs performed with PIRS. Median operative time (minutes) differed significantly (P = .001) with SEATL at 49 (28–66) and PIRS at 55 (37–76)] minutes. Significantly more incarcerated hernias were repaired with PIRS (n = 13) than with SEATL (n = 3, P = .006). SEATL had a higher number of postoperative complications; the most significant were granulomas (n = 3, P = .09) and recurrent hernias (n = 12, P < .001).
Conclusion:
SEATL had a significantly higher number of postoperative complications. This may be a result of multiple factors including but not limited to the absence of electrocautery, a shorter median operative time, and utilization of absorbable suture. Modifications have been made to this technique to reduce risk of postoperative complications.
Introduction
Inguinal hernia repairs (IHRs) are one of the most common procedures performed by pediatric surgeons around the world. Although the open method remains the most common for pediatric IHR, laparoscopic IHR has increased by 365% between 2009 and 2018. 1 Laparoscopic management of pediatric IHR was introduced by El-Gohary in 1997. 2 Since then, over a dozen different laparoscopic techniques have been developed. 3
With the rise in popularity of laparoscopic IHR, many researchers have set out to examine the differences in efficacy of open IHR compared with various laparoscopic IHR techniques.2,4–8 However, there are few studies directly comparing different laparoscopic techniques. By determining outcome discrepancies among popular laparoscopic techniques for pediatric IHR, we can help improve surgical techniques, postoperative outcomes, and patient satisfaction.
Two laparoscopic techniques that have gained popularity among pediatric surgeons in the past decade are the percutaneous internal ring suturing (PIRS) technique and the subcutaneous endoscopically assisted transfixion ligation (SEATL) technique. The PIRS and SEATL techniques both involve an umbilical trocar for laparoscopy. For unilateral hernias, the PIRS technique adds another incision in the left lower quadrant or right lower quadrant depending on hernia laterality for laparoscopic instrumentation of the peritoneum. In cases of bilateral hernias, two separate suture incisions are made in each lower quadrant, resulting in a total of four incisions.
One side is repaired first before the surgeon moves to the contralateral side. Saline or bupivacaine is injected into the retroperitoneal space behind the internal ring to elevate the peritoneum off the testicular vessels and vas deferens. A stab incision in the skin is made over the internal ring where a spinal needle is then used to direct looped Prolene sutures into the retroperitoneal space. The looped Prolene is used to thread two Ethibond sutures around the patent internal ring. The Ethibond sutures are tied thus highly ligating the hernia sac. In some versions of PIRS, the closed sac is then scored with electrocautery before ports and instruments are removed from the abdomen (Fig. 1).
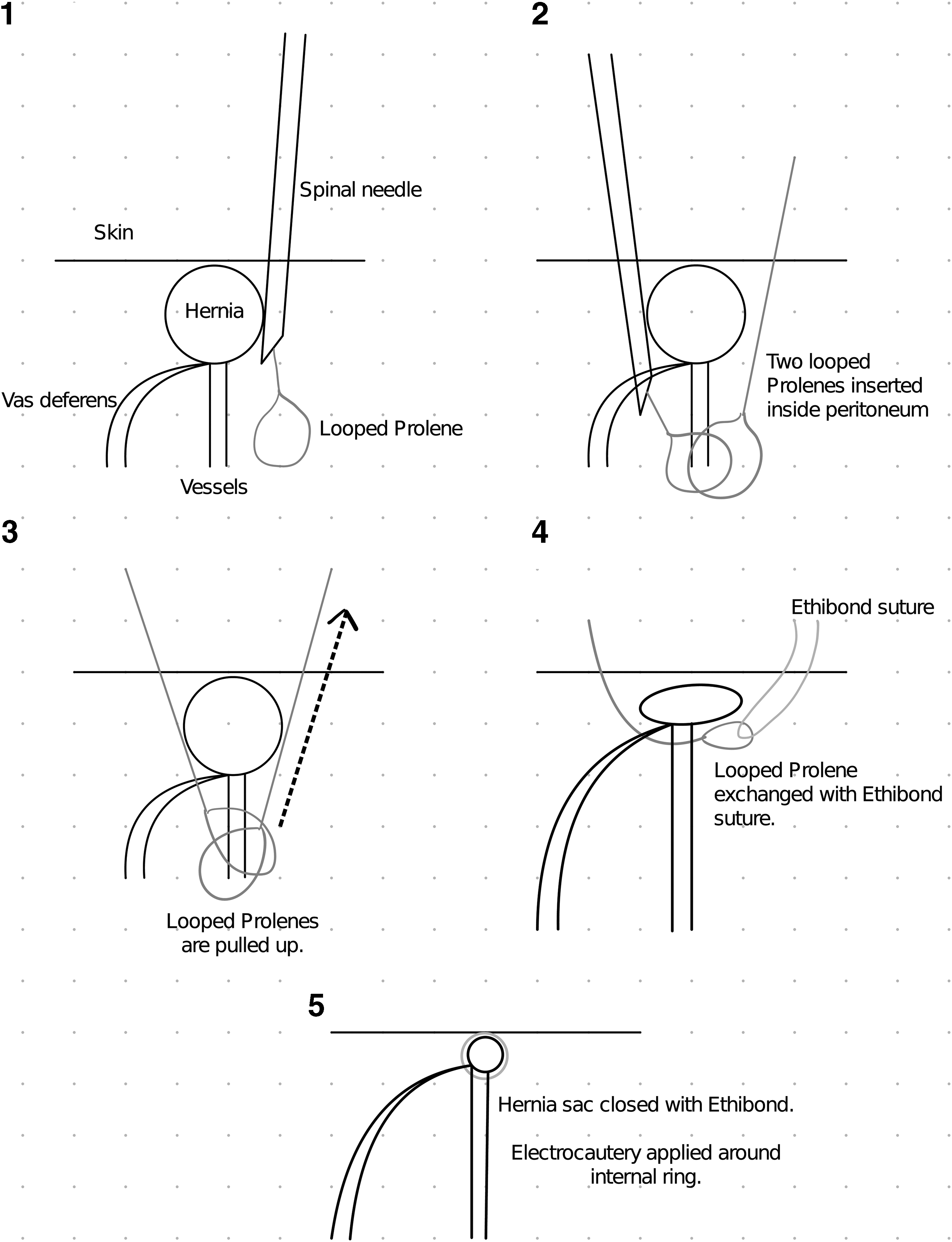
Percutaneous internal ring suturing technique.
The SEATL technique does not use a second laparoscopic instrumentation incision. After gaining peritoneal elevation off the testicular vessels and vas deferens with injected saline or bupivicane, the surgeon passes a curved needle through a stab incision over the patent internal ring, circumferentially around the entire internal ring, and back through the original incision. The needle is then passed a second time transversely across the internal ring and back through the original incision. The suture is tied extracorporeally to highly ligate the internal ring (Fig. 2).
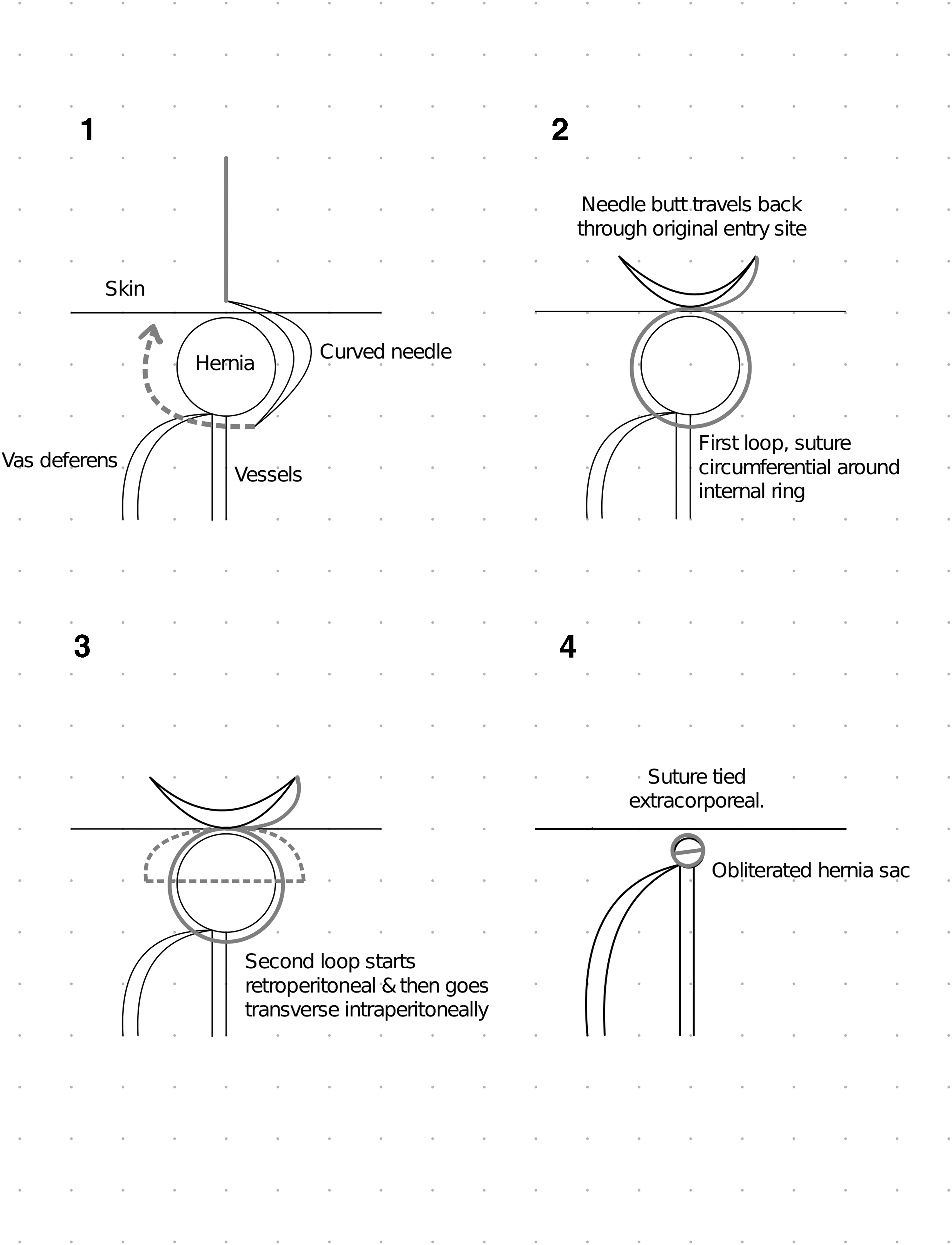
Subcutaneous endoscopically assisted transfixion ligature technique.
The most significant technical differences between PIRS and SEATL is the utilization of laparoscopic instruments to move the peritoneum and the use of electrocautery to create thermal injury at the site of the obliterated hernia sac. Thermal injury of the peritoneum has been shown to decrease recurrence rates after laparoscopic repairs in animal studies. These findings have led to increasing electrocautery application in PIRS. Despite this variation, prior studies have shown conflicting results.9–17 In this study, we investigated the outcomes and efficacy of PIRS and SEATL and explored underlying predictors for adverse postoperative outcomes.
Materials and Methods
After receiving approval from our institution's institutional review board (IRB-30004835), we performed a retrospective chart review between May 2020 and September 2015. Our review included every patient <18 years old who received an IHR at our institution. The stop point was set at September 2015, when laparoscopy for IHR was introduced to our institution. Variables were organized into categories including patient demographics, operative details, postoperative complications, recurrent operative details, and recurrent postoperative complications. Data were collected from operative notes, anesthesia records, follow-up visit notes, and telephone records. Follow-up visits were scheduled 2–3 weeks after surgery.
We used SPSS 28.0 (IBM Corporation, Armonk, NY, USA) to perform all statistical analyses. Categorical variables were analyzed using two-proportion z-test. Continuous variables were analyzed using Mann–Whitney U test. Binary logistic regression was performed to find predictors of recurrent inguinal hernias for both techniques. Continuous variables are presented as median [IQR 1–3]. P values ≤ .05 were considered significant.
Results
Patient demographics
There was a total of 255 laparoscopic repairs performed between May 2020 and September 2015 at our institution. The SEATL technique was used to repair 131 IHRs. The PIRS technique was used to repair 124 IHRs. Median age at time of operation was 17 [4–71] and 19 [6–53] months for SEATL and PIRS, respectively. Fifty patients who received SEATL and 37 patients who received PIRS had a history of premature birth. SEATL was performed for 32 females and 99 males. PIRS was performed for 25 females and 99 males. Median weight for patients who underwent SEATL was 11 [6.2–21] and 11.5 [6.8–17.2] kg for patients who received PIRS. There were no statistical differences in patient demographics between the SEATL and PIRS groups (Table 1).
Patient Demographic Comparison for Subcutaneous Endoscopically Assisted Transfixion Ligation Versus Percutaneous Internal Ring Suturing
IQR, interquartile range; PIRS, percutaneous internal ring suturing; SEATL, subcutaneous endoscopically assisted transfixion ligation.
Operative details
The median operative time for SEATL was shorter than that for PIRS at 49 [28–66] minutes versus 55 [37–76] minutes, respectively (P = .001). A total of 127 reducible hernias were repaired with SEATL, and 110 reducible hernias were repaired with PIRS (P = .01). The number of incarcerated hernias repaired with PIRS and SEATL was 13 and 3, respectively (P = .006). No significant differences were observed in presence and frequency of concomitant conditions. The most common comorbidities observed and operated on during IHR were umbilical hernias and hydroceles. PIRS primarily utilized Ethibond suture for repairs, with 122 repairs done with Ethibond and 2 done with Vicryl. SEATL repairs were divided with 91 Ethibond repairs and 40 Vicryl repairs (Table 2).
Operative Details Comparison for Subcutaneous Endoscopically Assisted Transfixion Ligation Versus Percutaneous Internal Ring Suturing
Included for significant P values.
IQR, interquartile range; PIRS, percutaneous internal ring suturing; SEATL, subcutaneous endoscopically assisted transfixion ligation.
Postoperative outcomes
A total of 12 inguinal hernias recurred after SEATL repair and 1 inguinal hernia recurred after PIRS repair (P < .001). Median time to follow-up visit was 29 and 24 days for SEATL and PIRS, respectively (P = .582). Median time to recurrent inguinal hernia for SEATL was 172 days. PIRS had one recurrent inguinal hernia that recurred after 42 days. The number of recurrences between SEATL and PIRS was too disparate to identify a significance when comparing median time with recurrence. Other postoperative complications after PIRS included one ecchymosis, two complaints of persistent postoperative pain, and one recurrent hydrocele. SEATL postoperative complications included two complaints of persistent postoperative pain, two wound infections, three stitch granulomas, and one recurrent umbilical hernia (Table 3).
Postoperative Complications Comparison for Subcutaneous Endoscopically Assisted Transfixion Ligation Versus Percutaneous Internal Ring Suturing
Included for significant P values.
IH, inguinal hernia; IQR, interquartile range; PIRS, percutaneous internal ring suturing; SEATL, subcutaneous endoscopically assisted transfixion ligation.
Predictors of recurrent hernias post-SEATL
There were no patient demographic variables that were predictors of recurrence (Table 4). Median operative time for operations preceding recurrent IH was 51 [20.5–70] minutes (P = .71, odds ratio = 0.996). Hernia laterality was not a significant predictor of hernia recurrence. All hernia recurrences occurred after repair of reducible inguinal hernias (Table 5).
Patient Demographic Predictors of Recurrent Hernias Postsubcutaneous Endoscopically Assisted Transfixion Ligation Using Logistic Regression
SEATL, subcutaneous endoscopically assisted transfixion ligation.
Intraoperative Detail Predictors of Recurrent Hernias Postsubcutaneous Endoscopically Assisted Transfixion Ligation Using Logistic Regression
CI, confidence interval; IQR, interquartile range; SEATL, subcutaneous endoscopically assisted transfixion ligation.
Suture type for repair
There were a total of 213 cases repaired with Ethibond and 42 cases repaired with Vicryl. Out of these, six recurrences occurred after Ethibond utilization and seven recurrences occurred after Vicryl utilization. The proportion of recurrences after repair with Vicryl was significantly higher than the proportion of recurrences after repair with Ethibond (P = .002; Table 6).
Suture Type Used for Repair Preceding Recurrent Inguinal Hernias Versus Nonrecurrences for Percutaneous Internal Ring Suturing and Subcutaneous Endoscopically Assisted Transfixion Ligation
Included for significant P values.
Discussion
In this study, we investigated the outcomes of two different pediatric laparoscopic inguinal hernia techniques and recognized a recurrence rate of 9.2% with SEATL, which was significantly higher than the recurrence rate of PIRS (0.8%). The most significant technical difference between SEATL and PIRS is the utilization of electrocautery to create thermal injury. The importance of thermal injury in laparoscopic IHR has been described by few studies with conflicting results.17–19 Blatnik et al. and Ostlie and Ponsky both reported that intentional peritoneal injury during laparoscopic IHR produces a more durable repair and reduces risk of recurrence.17–19
St-Louis et al. suggested that intentional thermal injury may have effects on the characteristics of peritoneal scarring due to the difference in median time to recurrence in their study. 9 However, this difference was not significant, and they did not observe an improvement in recurrence rate after application of intentional thermal injury to the internal ring in their patients. 9 We believe that intentional peritoneal injury by electrocautery was a key contributor to the discrepancy in recurrences between SEATL and PIRS. Without thermal injury, there was an insufficient amount of scar tissue to hold the internal ring defect closed in the case of suture failure or reabsorption.
Our SEATL results showed a significant correlation between recurrent inguinal hernia and suture type used for repair. These findings were also supported by the low number of recurrent inguinal hernias from PIRS that primarily utilized Ethibond, a nonabsorbable suture. Grimsby et al. reported similar findings in their study comparing nonabsorbable and absorbable sutures utilization with the SEAL technique for laparoscopic IHR. 20 They found that suture type was an independent predictor of failure for laparoscopic repair with 13 recurrences using absorbable suture and 2 recurrences using nonabsorbable suture. 20 Other major studies that only used nonabsorbable suture reported lower recurrence rates than studies that only used absorbable suture.20–22
Bharathi et al. performed a short-term outcome study utilizing only absorbable suture. 22 They stated in their discussion that “the early dissolution of absorbable thread before the obliteration of the patency of the sac” may have contributed to their rate of recurrent inguinal hernias. 22 Our results were in concordance with prior studies showing that nonabsorbable suture may be the superior suture for pediatric laparoscopic IHR.
Our study revealed a total of three stitch granulomas post-SEATL. Interestingly, all three stitch granulomas developed after use of Ethibond, a nonabsorbable suture. Postoperative granuloma formation has been described as a complication with nonabsorbable suture utilization in the literature.23–25 Son and Bao reported 15 granuloma formations in their 418 nonabsorbable suture patient cohort and 0 granuloma formation in their 277 absorbable suture cohort. 25 Our results, although not as significant, showed a possible disadvantage with nonabsorbable suture utilization. However, this postoperative complication is not outweighed by the superiority of nonabsorbable suture with more severe complications such as inguinal hernia recurrence.
We recognize as a retrospective study that there are many confounding variables with unaccounted effects on our data including decision making for type of suture; procedure selection for patients; and in some cases, long-term follow-up. Decision making was largely up to the 2 surgeons who performed laparoscopic IHR at our institution, so selection bias was present. However, our study does have some a few notable features. Laparoscopy for pediatric inguinal hernia was introduced to our institution in September 2015. The 2 surgeons who perform SEATL and PIRS learned their respective techniques at the same time. It could be argued that one technique is more difficult to master than the other. However, given the small discrepancy between case load, both surgeons had similar conditions in learning their techniques.
Conclusion
The SEATL laparoscopic technique for pediatric IHRs appears to produce more recurrent inguinal hernias than the PIRS technique. Patients may benefit from modifications to SEATL to reduce risk of recurrent inguinal hernia. Nonabsorbable suture may be superior to absorbable suture in laparoscopic repair of pediatric inguinal hernias.
Footnotes
Authors' Contributions
T.A.D. and V.E.M. had access to all patient information in the study, and also had access to all data in the study and take responsibility for the integrity of the data and accuracy of data analysis.
Concept and design were carried out by T.A.D., J.R.E., and V.E.M.
Drafting of the article was done by T.A.D. and V.E.M.
Statistical analysis was taken care of T.A.D. and G.R.
Obtained funding was taken care of T.A.D.
Administrative, technical, and material support were carried out by J.R.E. and V.E.M.
Supervision was by V.E.M.
Disclosure Statement
No competing financial interests exist.
Funding Information
This article was funded by NIH T35 HL007473 under T35 SHIRT.