
Abstract
Purpose:
The effect of metabolic risk factors on the recurrence rate of hiatal hernia (HH) after the initial repair is still controversial. In this study, we evaluated whether a poor preoperative metabolic profile is a risk factor for the recurrence of a HH after surgery.
Methods:
Perioperative patient data were obtained from hospital records. A poor metabolic profile was defined as having two or more metabolic conditions such as diabetes, hypertension, hyperlipidemia, or being overweight. The recurrence rates of HH were measured at 6 months, and again at 12 months after surgery.
Results:
Data were collected from a total of 221 patients. While 87 (39.4%) patients underwent tension-free mesh (TFM) repair, 137 (60.6%) were treated with suture repair. The poor metabolic profile has no effect on the recurrence rates in the suture-repair group. However, patients who underwent TFM repair displayed a significantly higher recurrence rate at the 12-month time point if they had poor metabolic profile, compared to the healthy group (respectively, 20.7% and 3.4%, P < .01). The logistic regression analysis showed that having a poor metabolic profile was an independent risk factor for recurrence after 12 months in the same group (odds ratio: 8.04 confidence interval [CI: 1.2–53.5] P = .03).
Conclusion:
The poor metabolic profile was found to be responsible for high recurrence rates only in patients who underwent TFM HH repair.
Introduction
Hiatal hernia (HH) is one of the most common disorders worldwide. 1 The vast majority of HH cases consist of type 1 HH (90%), which is often associated with treatment-resistant gastroesophageal reflux disease symptoms.1–3 Surgical indication of HH depends on the type of HH and its corresponding symptoms. 4 The major indication for type 1 HH surgery is the presence of reflux symptoms. 5 The choice of surgical techniques has been defined as a significant factor that influences postsurgical complications such as dysphagia, impaired esophageal motility, and also short- and long-term recurrence. 6 Primary suture-cruroplasty has been the mainstay of practice. When only the crural suture technique was performed to cure for HH, there was a higher possibility of dysphagia and recurrence.7,8 At this point, the ideal surgical techniques are unknown. The Mesh reinforcement technique has been utilized to reduce the recurrence rate.
In a meta-analysis, mesh-augmentation was found to be related to a less short-term recurrence rate. 9 However, long-term results were not identified in this study. In a recent meta-analysis, there were no significant differences between these two repair techniques regarding short- or long-term recurrence. 10 Complications such as dysphagia and chest pain due to esophageal erosion, stenosis, fibrosis, and difficulty of reoperation because of the mesh are current problems for the tension-free mesh (TFM) method. Risk factors should be determined to reduce recurrence and complication rates in HH patients, for whom the decision of surgical intervention is made, and the most appropriate type of surgery should be selected for the patient accordingly.
Although it is known that being overweight and advanced age are the most important risk factors for HH, the effect of the poor metabolic profile on recurrence after HH operation is still unknown.4,11,12 In this study, we aimed to retrospectively assess the independent risk factors for recurrence after HH repair surgery and to evaluate the effect of poor metabolic profile on the surgery outcomes.
Materials and Methods
Patient enrollment and data curation
We collected historical data from type 1 HH patients with gastroesophageal reflux symptoms who were admitted to our general surgery clinic from 2017 May to 2021 January. This study was approved by the local Ethics Committee (OEAH-48670771-514.10). Preoperative upper gastrointestinal endoscopy was used to diagnose HH and was performed by an experienced gastroenterologist. All upper gastrointestinal endoscopy findings were recorded, including features of the hernia, hernia size, and other endoscopic pathologies such as esophagitis, gastritis, or ulcers. HH classification was made using the SAGES guideline. Sliding (type 1) HH was defined as when the gastroesophageal junction migrates above the diaphragm and the fundus remains below the gastroesophageal junction. 6
Other types of HH [type 2–3] have not been included in this study. Other exclusion criteria were asymptomatic patients; patients with grades C–D esophagitis; patients who have a history of HH or gastroesophageal surgery, and patients whose follow-up data were not available at 6 and 12 months.
Patients' serum C reactive protein (CRP), hemoglobin (Hgb), creatinine, and fasting plasma glucose (FPG) results were obtained from hospital electronic records. Clinical and demographic information such as body mass indexes (BMIs) and past medical history about the comorbid situations including medications were obtained from the patient's charts and electronic databases. Patients who have a BMI ≥25-kg/m2 were considered overweight. History of diabetes mellitus (DM), hypertension (HT), and hyperlipidemia were collected from patients' charts. A poor metabolic profile was defined as a separate group that includes the patients who have two or more metabolic conditions.
The perioperative protocol of TFM repair and assessment of recurrence
All procedures are conducted via a laparoscopic approach with the patient under general endotracheal anesthesia. The anterior to posterior (AP) and transverse diameters of the HH were measured using a sterile ruler before the preparation of the mesh. The AP diameter was measured in centimeters from the beginning at the crural commissure to the upper point of the defect. The distance between both crural edges was considered a transverse diameter. The AP diameter was used in the statistical analysis as
Excluded mesh area is calculated according to the patients' hernia size. The mesh was replaced on the right-left crura by tucker (BD Capsure) and closed hiatus defect. A schematic demonstration of TFM HH repair is shown in Supplementary Figure S3. In the suture-repair technique, as described in previous studies, the HH defect was closed with sutures that would approximate the crural parts.13,14 In both methods, the surgery was completed with a 360° floppy fundoplication with two and a half sutures. We place a nasogastric-feeding catheter after the surgery for 1 day in all patients. Peroral feeding starts on the postoperative first day with only fluid liquids. All patients are being followed up with eating only soft food for 4 weeks.
All of the patients' control endoscopy is performed 6–12 months after operation time. Patients were evaluated clinically and received a standardized questionnaire postoperatively at 6 and 12 months. Questionnaires were self-administered, improvement in symptoms, and satisfaction with the surgery. Medication requirements for reflux symptoms were recorded. Recurrence was determined according to clinical and endoscopic postoperative evaluations.
Statistical analyses
All analyses were performed using SPSS version 21.0 for Windows (IBM, Inc., Chicago, IL). The variables were investigated using visual (histograms, probability plots) and analytical methods (Kolmogorov–Smirnov/Shapiro–Wilk tests) to determine whether or not they were normally distributed. Continuous variables were shown as mean standard deviation (SD) or median (interquartile range) according to their distribution pattern. Continuous variables that do not have normal distribution were compared by the Mann–Whitney U test. The Student's t-test was used to evaluate differences between the two groups in normally distributed continuous variables. The chi-square test or Fisher's exact test was used for comparisons of categorical variables.
For multivariate analysis, the possible factors identified by univariate analysis or recent studies were further entered into the logistic regression analysis to determine independent predictors of 12th-month recurrence. Variables that did not make a significant contribution were excluded from the final model using the backward likelihood ratio stepwise method. Hosmer-Lemeshow goodness-of-fit statistics were used to assess the model. A P value <.05 was considered a statistically significant result.
Results
A total of 221 patients' data were collected. While 87 (39.4%) of patients underwent TFM repair, 137 (60.6%) of them were in the suture-repair group. One hundred twenty-four patients were male and 97 patients were female. Other demographics are shown in Table 1. When the TFM repair and suture-repair groups were compared, the hernia size was significantly higher in the TFM repair group (6.5 cm versus 4.5 cm P < .001). There was no statistical difference between the groups with regard to the 6th and 12th months' recurrence rate. The prevalence of metabolic profiles such as diabetes, hyperlipidemia, and hypertension were similar in both groups.
General Characteristics of the Study Population (n = 221)
Poor metabolic profile was defined as a separate group that includes the patients who have two or more metabolic conditions.
BMI, body mass index; CRP, C reactive protein; IQR, interquartile range Q25–Q75; SD, standard deviation.
There was no significant difference between the groups in terms of the number of overweight patients. Patients were discharged after a median of 3 days. In addition, there was no significant difference between the mesh and suture groups regarding mean hospitalization time (3.12 SD1.15 and 3 SD1.07, respectively, P = .43). The comparison of demographic and clinical features in TFM repair and suture-repair groups is shown in Table 2.
Comparison of Tension-Free Mesh Suture Repair Versus Repair Groups in Terms of Demographic and Clinical Features
Bold represents statistically significant results.
Normally distributed variables are shown as mean ± SD, non-normally distributed variables were shown as median and interquartile range Q25–Q75.
Poor metabolic profile was defined as a separate group that includes the patients who have two or more metabolic conditions.
BMI, body mass index; CRP, C reactive protein; SD, standard deviation; TFM, tension-free mesh.
There was no statistical difference between poor and good metabolic profiles, including diabetes, hypertension, hyperlipidemia, and body weight, when analyzing recurrence rates from the 12th month in the suture-repair group (Table 3). However, TFM repair subgroup analysis showed that while the recurrence rates were 20.7% in the poor metabolic group, it was 3.4% in patients with normal metabolic profiles, and the difference was statistically significant (P < .01). Total 12th-month recurrence rates in different demographic and metabolic subgroups are shown in Table 3. There was no significant difference between 12th recurrence and nonrecurrence groups with regard to preoperative routine serum analyses such as CRP, FPG, Hgb, and creatinine (Fig. 1).
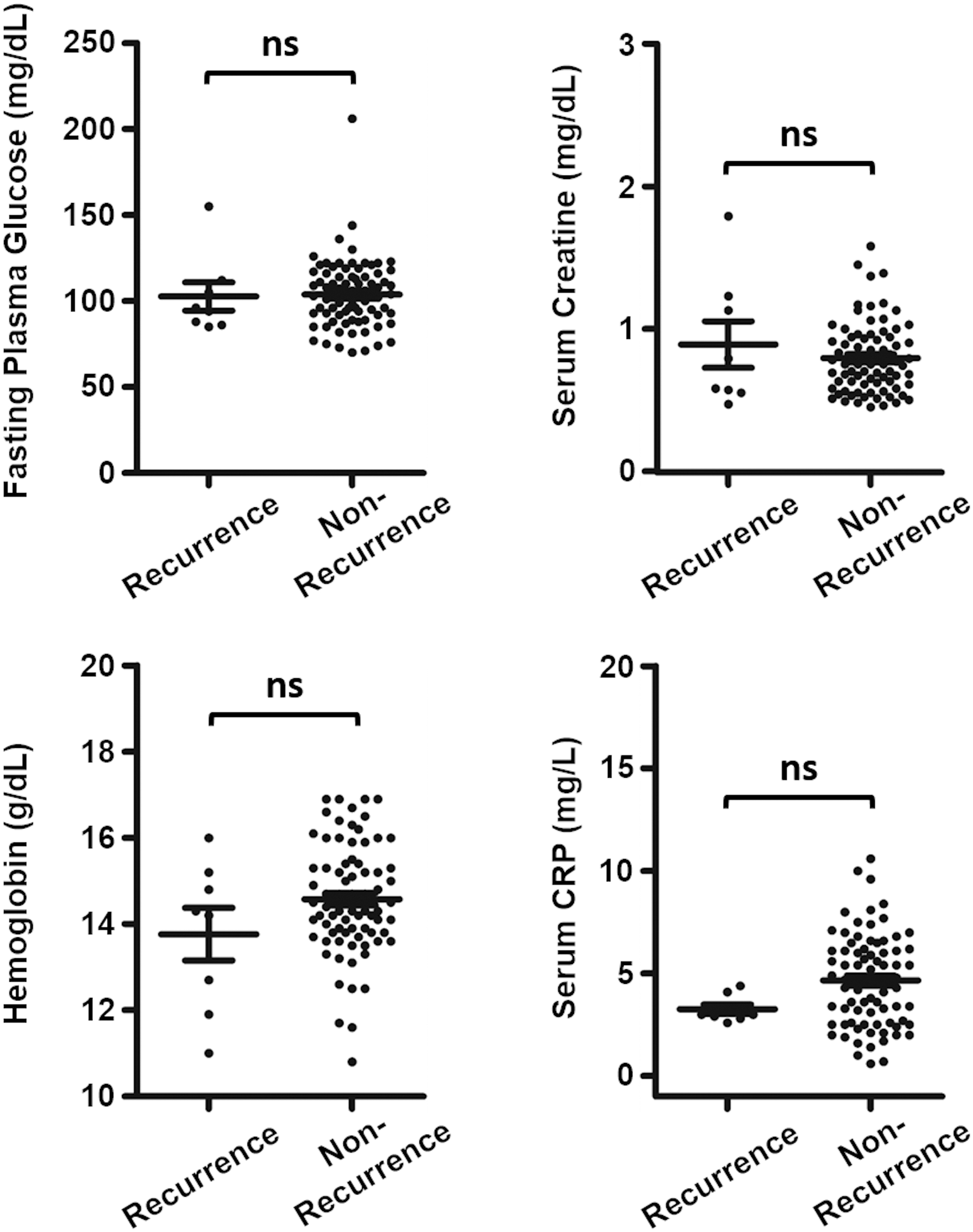
Dot plot graphs of preoperative laboratory parameters in recurrence and nonrecurrence groups.
The Comparison of Metabolic Profiles in Patients Who Underwent to Hiatal Hernia Repair Surgery in Terms of Recurrence Rates at 12-th Month
Fisher's exact test was used.
Poor metabolic profile was defined as a separate group that includes the patients who have two or more metabolic conditions.
BMI, body mass index; TFM, tension-free mesh.
Pneumothorax was seen only in 4 patients as an intraoperative complication. These 4 patients had relatively big HHs (range 6–8 cm). One of these patients underwent standard suture repair. Tube thoracotomy was performed by the chest surgery for those patients immediately during operation and all patients fully recovered postoperatively. We detected only 1 patient with toxic hepatitis as a postoperative complication possibly due to anesthetics. This patient was discharged after serum transaminase levels turned back to normal.
In the univariate and multivariate logistic regression analysis of the entire study population, only hernia size was identified as an independent risk factor for recurrence at the 12th month (odds ratio [OR]: 1.32 confidence interval [CI: 1.0–1.75] P = .049) (Table 4). In the TFM repair group, the poor metabolic profile was found to be an independent risk factor for recurrence after 12 months (OR: 8.04 [CI: 1.2–53.5] P = .03) (Table 5).
Logistic Regression Analysis Demonstrates the Independent Risk Factors for Recurrence After 12 Months from Hiatal Hernia Repair Surgery (n = 221)
Bold represents statistically significant results.
Male gender was considered as a reference categorical group.
Presence of condition or disease was considered as a reference category for the regression analyses.
Poor metabolic profile was defined as a separate group that includes the patients who have two or more metabolic conditions.
BMI, body mass index; CI, confidence interval; OD, odds ratio.
Logistic Regression Analysis Demonstrates Independent Risk Factors for Recurrence After Surgery in Tension-Free Mesh Group (n = 87)
Bold represents statistically significant results.
Male gender was considered as a reference categorical group.
Presence of condition or disease was considered as a reference category for the regression analyses.
Poor metabolic profile was defined as a separate group that includes the patients who have two or more metabolic conditions.
BMI, body mass index; CI, confidence interval; OD, odds ratio,
Discussion
Mesh repair in HH surgery is a technique that has been used increasingly in recent years and has been shown in some studies to reduce the high risk of recurrence seen in the suture-repair technique.9,15 Despite this, recurrence is still one of the most prevalent problems during the postoperative follow-up. It is still thought that there are other risk factors for recurrence, regardless of the surgical technique. The relationship between hernia size, hernia type, demographic characteristics, mesh features (biological versus other), and recurrence risk has been demonstrated.9,13,16 However, the optimal risk assessment for postoperative short- and long-term recurrence is not well established. In addition, there is no clear information about a possible association between metabolic profile and postoperative recurrence in the literature. For these reasons, we evaluated the effects of preoperative poor metabolic profile on recurrence rates at 1-year follow-up.
The use of mesh in HH repair surgery has been reported at rates of 30% to 50%. 9 In our study, consistent with these data, 40% of patients underwent TFM repair. The biodegradable or permanent meshes are usually preferred in repair for large HHs. Although the main purpose of mesh use is to reduce recurrence rates, long-term recurrence rates were found to be similar in studies comparing mesh repair with suture-repair method.10,13,17 In our study, only biodegradable mesh and suture-repair groups were compared in terms of recurrence rates. In agreement with the previous data, there was no significant difference in recurrence rates between the groups, in which mesh and suture-repair techniques were used.13,17
A comparative study demonstrated that the recurrence rate of HH after laparoscopic fundoplication is significantly higher in patients with large hernias. 16 In our study, when the TFM and suture-repair groups were evaluated together, it was found that hernia size was the only independent risk factor for recurrence. However, this effect was not prominent in TFM repair subgroup analyses.
Metabolic disorders such as DM, HT, dyslipidemia, and obesity are major public health problems all over the world. The association between poor outcomes and surgery is well defined in previous studies. 18 DM is one of the major risk factors for incisional hernia with wound infection, obesity, and suture closure method. 19 Patients with DM have impaired wound healing and are also at high risk for surgical site infection.20,21 These factors increase the probability of incisional hernia development. 22 According to another piece of data, DM is a prognostic risk factor for de novo HH after resection for gastric and esophageal cancer. High BMI is also found to be another risk factor for de novo HH in the same study. 23
In a prevalence study among morbidly obese patients who were undergoing bariatric surgery, HH was present in almost 40% of patients. 24 It was also found that BMI was high in the HH population in our study. Another bariatric surgery study illustrated that intraabdominal pressure (IAP) was elevated in patients with morbid obesity. HT and BMI were also independent risk factors for elevated IAP in obese patients. In addition to this, the presence of IAP may lead to a higher risk for developing different types of abdominal and HHs. 25 According to a recent study, visceral obesity is a predictor of surgical site occurrence and hernia recurrence after open abdominal wall reconstruction. 26
Despite all the findings in support of our hypothesis, DM and being overweight were not risk factors for recurrence in our study. However, poor metabolic profile, which was defined as having two or more metabolic conditions such as DM, HT, dyslipidemia, and high BMI, was an independent risk factor for 12th-month recurrence in the TFM repair group.
In patients with metabolic syndrome, cytokines such as tumor necrosis factor-alpha, interleukin 6, and CRP secreted from visceral adipose tissue create a chronic proinflammatory state. 27 Besides that, this proinflammatory maladaptive response leads to poor outcomes after different types of surgery.28,29 In our study, however, no significant difference was found between the groups with and without recurrence in terms of preoperative serum CRP level.
Even though the retrospective design of our study may cause an issue with the generalizability of the results, we think that our findings based on relatively high numbers of patients-data will encourage future studies. Other limitations of our study are the lack of a group that uses permanent mesh for repair and includes only short-term endoscopic evaluation of HH recurrence.
Conclusions
A poor metabolic profile seems to be an independent risk factor for recurrence in patients who underwent HH TFM repair surgery. A preoperative assessment of the metabolic profile may predict the postoperative recurrence risk. Furthermore, it can be a useful tool for determining the optimal surgical technique and the timing of the surgery.
Footnotes
Authors' Contributions
E.E.: Conceptualization, Methodology, Data curation, and Writing—Original draft preparation, Visualization, and Investigation. E.A.: Supervision and Writing—Reviewing and Editing.
Acknowledgments
We thank the department of biostatistics and bioinformatics of our hospital for data evaluation, graphical design, and advanced statistical analysis.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.