
Abstract
Objective:
Small anterior branch of gastrocolic trunk (SABGT) can be occasionally observed during transverse colectomy and right hemicolectomy. Improperly dealing with the branch may lead to unwanted bleeding and affect the operation process. The purposes of this study are to analyze the frequencies and injury of SABGT.
Methods:
Intact operation data were collected retrospectively from 39 colon cancer patients who underwent curative laparoscopic transverse colectomy or right hemicolectomy. Frequencies and injury of SABGT were analyzed.
Results:
Eight cases had SABGT, the frequencies of which is 20.5%. Injury of SABGT occurred intraoperatively in 2 patients.
Conclusion:
We suggest that SABGT should be considered in surgical management. Consciously looking for and properly dealing with the branch can minimize the influence on the operation process.
Introduction
The anterior of the pancreatic head is the high bleeding risk region during laparoscopic transverse colectomy and laparoscopic right hemicolectomy. Bleeding in this region is mostly related to the injury of gastrocolic trunk of Henle (GCT) and its branches. 1 Open conversion have to be chosen in some uncontrollable bleeding cases.
GCT is a venous trunk and formed by the convergence of the stomach-draining right gastroepiploic vein (RGEV), anterior superior pancreaticoduodenal vein, and the superior right colic vein (SRCV), and drains into the superior mesenteric vein (SMV) at the inferior border of the pancreas2–5 (Fig. 1). The branches of GCT are highly variable.6–9
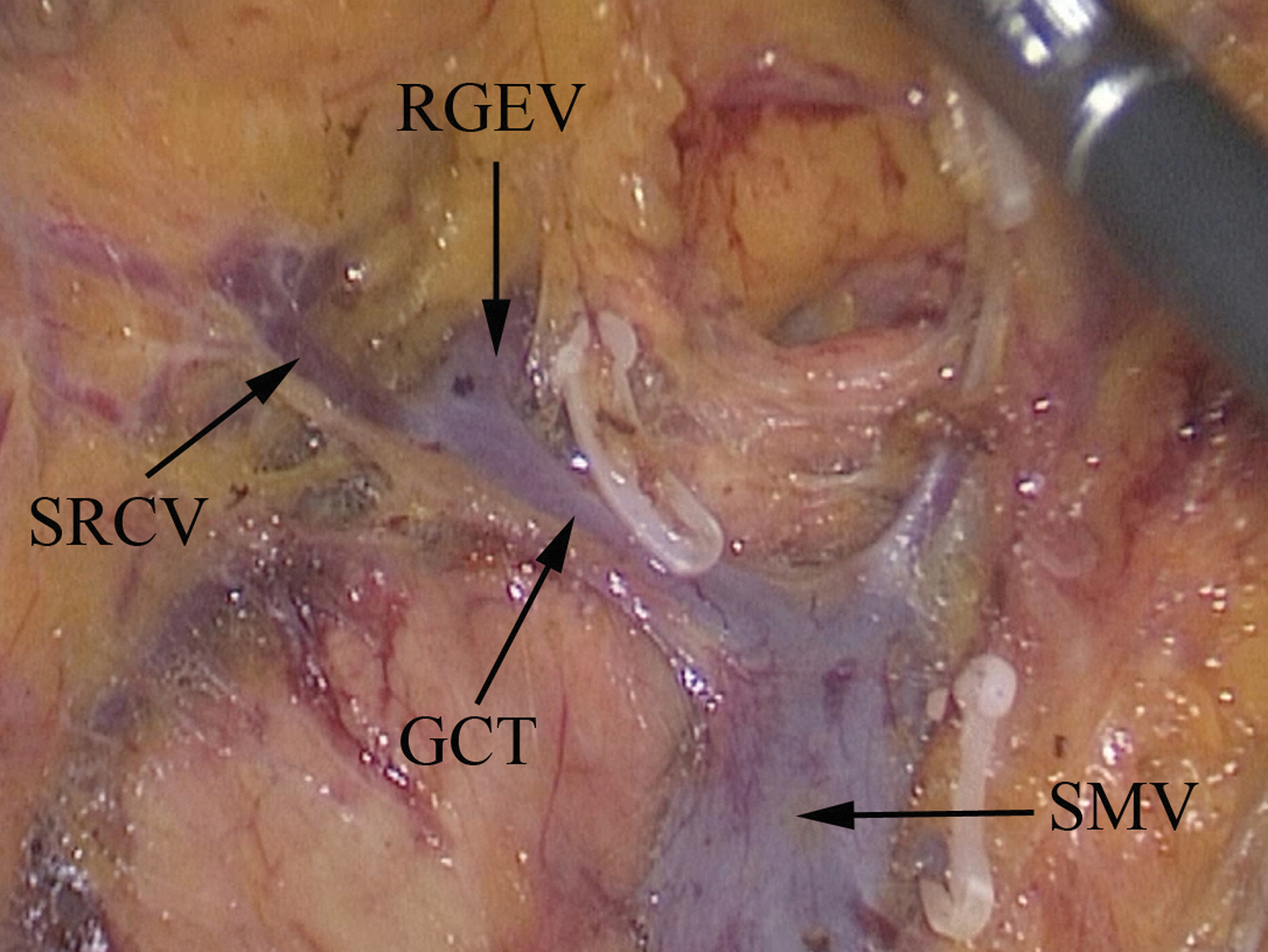
Gastrocolic trunk of Henle and its branch. GCT, gastrocolic trunk of Henle; RGEV, right gastroepiploic vein; SMV, superior mesenteric vein; SRCV, superior right colic vein.
Laparoscopy techniques allows us to observe small anatomical structures that cannot be seen in open surgery.10–12 During transverse colectomy and right hemicolectomy small venous branch in front of GCT can be observed occasionally and drains into anterior wall of the GCT in some patients. Improperly dealing with the branch may cause injury and lead to bleeding. The purpose of this study was to analyze the frequencies and injury of small anterior branch of gastrocolic trunk (SABGT).
Materials and Methods
Patients
Intact operation data were collected retrospectively from 39 colon cancer patients who underwent curative laparoscopic transverse colectomy (n = 6) or laparoscopic right hemicolectomy (n = 33) from June 2015 to June 2022 at two centers, including The Second Hospital of Tianjin Medical University, Tianjin, China and The First Affiliated Hospital of Kunming Medical University, Kunming, Yunnan, China. Among the 39 cases with colon cancer, there were 17 males and 22 females, with an average age of 56.9 years. This study was conducted in accordance with the Declaration of Helsinki, and with the approval of the Ethics Committee of the Second Hospital of Tianjin Medical University and the First Affiliated Hospital of Kunming Medical University. Written informed consent was obtained from all the participants.
Operative methods
Laparoscopic transverse colectomy
The procedure was performed according to the principle of complete mesocolic excision. The peritoneum is incised at horizontal part of duodenum level to expose the right side of SMV. Then the dissection along the superior mesenteric vessels is continued cephalad to expose the root of the GCT, and then the imaginary line connecting the GCT and the accessory right colic vein is identified. If SABGT is occasionally identified during the dissection, it should be cut at their roots with vessel clamp. During the operation along the surface of GCT, dissection should be performed carefully toward distal of GCT to find whether SABGT exist or not, and SABGT should be properly dealt with to avoid injury and bleeding of SABGT. The rest of the procedure was performed as described in the literatures.13–15
Laparoscopic right hemicolectomy
The procedure was performed according to the principle of complete mesocolic excision. The inferior approach was used to mobilize the right colonic mesentery. After completing the lateral dissection to the base of the ileal mesentery, the peritoneum is incised between the ridge and the periphery of the SMV. Then the dissection along the superior mesenteric vessels is continued cephalad to expose the root of the GCT, and then the imaginary line connecting the GCT and the accessory right colic vein is identified. If SABGT is occasionally identified during dissection, it should be cut at their roots with vessel clamp (Fig. 3). During the operation along the surface of GCT, dissection should be performed carefully toward distal of GCT to find whether SABGT exists or not, and SABGT should be properly dealt with to avoid injury and bleeding of SABGT. The rest of the procedure was performed according to the literatures.16–20
Observational methods
To avoid the injury of SABGT, the dissection along the superior mesenteric vessels is adopted to expose the root of the GCT. Dissection is continued along the surface of GCT toward distal end to expose its branches, SABGT is carefully looked for to avoid bleeding. Videos of the operation were preserved for further verification. The frequencies and injury of SABGT were analyzed.
Results
The study included 39 patients; 36 cases had a common trunk formed by SRCV and RGEV. Three cases had the SRCV directly draining into SMV and there is no common trunk with the RGEV. Two cases had middle colic vein converging on the GCT. Eight cases had SABGT (Fig. 2), the frequencies of which is 20.5%. SABGT were cut at their roots with vessel clamp (Fig. 3).
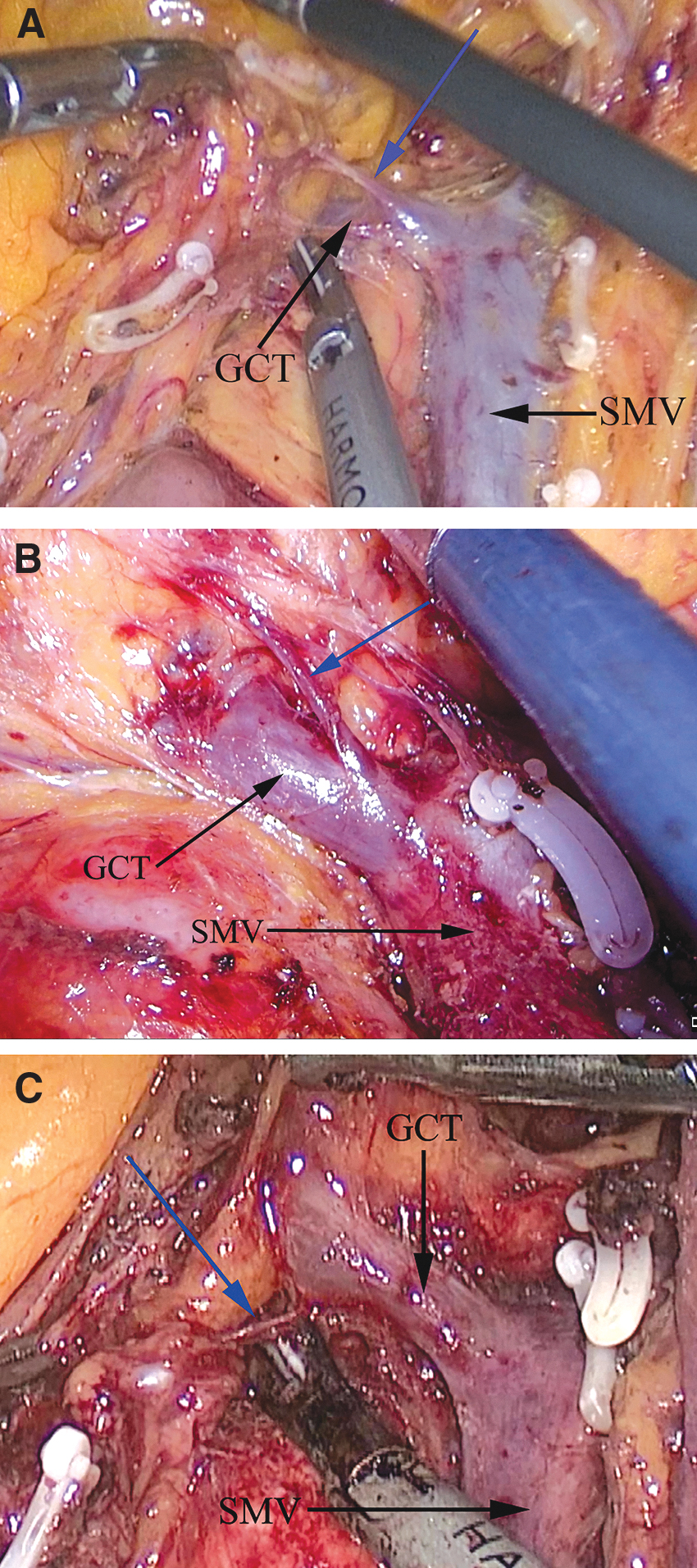
Small anterior branch of gastrocolic trunk (blue arrow). GCT, gastrocolic trunk of Henle; SMV, superior mesenteric vein.

Small anterior branch of gastrocolic trunk was cut at their roots with vessel clamp.
In 2 patients SABGT are very thin. Among which SABGT of 1 patient was ruptured and caused bleeding during retracting the right mesocolon, the other one was also ruptured and caused bleeding during dissecting GCT. The bleeding in 2 patients were stopped, respectively, with ultrasonic scalpel or vascular clamp, and did not have a direct influence on the operation process. No bleeding occurred in the rest of 6 cases with SABGT due to careful exposure and proper dissection, and there was no conversion to open surgery cases.
Discussion
The anterior of the pancreatic head is the high bleeding risk region during laparoscopic transverse colectomy and laparoscopic right hemicolectomy. Improperly dealing with vein in this region may lead to bleeding and conversion to open surgery. 21
The branches of Helen trunk are highly variable, right colic vein and middle colic vein sometimes drained into GCT. These variations increase the risk of intraoperative bleeding.22–25 Therefore, the management of GCT and its branches become the key to controlling the bleeding in the anterior area of pancreatic head. During the operation we observed SABGT in some patients, which increased the risk of bleeding in the anterior area of pancreatic head.
Preoperative computed tomography vein three-dimensional imaging can evaluate the anatomical variation of gastrocolic vein trunk before operation, which is helpful for operators to correctly understand its anatomical structure and choose a reasonable anatomical approach.26–32 However, the SABGT is so thin that imaging examination cannot provide help for operation. Operator needs to pay attention to protecting the SABGT during operation so as to reduce the risk of injury and bleeding of SABGT.
In this study, we clearly exposed the GCT and its branches, consciously look for and properly deal with SABGT to avoid injury and bleeding of SABGT. A total of 39 patients were enrolled, frequencies and injury of SABGT were analyzed through observing the playback of videos of the operation. There was no conversion to open surgery cases. Eight patients had SABGT, the frequencies of which is 20.5%. It is much higher than our initially expected. Six of the 8 patients undergo careful exposure and proper dissection of SABGT, and no injury occurred during operation.
In 2 patients SABGTs were too small to be easily recognized, which were ruptured and caused bleeding during retracting mesocolon and dissecting GCT, respectively. The bleeding in 2 patients were stopped, respectively, with ultrasonic scalpel and vascular clamp, and did not have a great influence on the operation process.
Footnotes
Authors' Contributions
All authors have contributed significantly and are in agreement with the content of the article.
Disclosure Statement
The authors declare no competing financial interest.
Funding Information
This study was supported by grants from the National Natural Science Foundation of China (Grant Nos. 81660302 and 81660238) and the Youth Foundation of the Second Hospital of Tianjin Medical University (Grant Nos. 2019ydey02, 2019ydey09, and 2020ydey20).